Effect of Blood Pressure Control on Cardiovascular Events in Patients with Chronic Kidney Disease: A Systematic Review
Anas E Ahmed, Khaled W Halawany, Faizah S Alyahyawi, Abdullah H Khormi, Hussain M AlQibti, Othman M Saifain, Talal M Alqarni, Jana S Alqurashi, Rose M Alabdali, Shoog T Alowaimer

TL;DR
This review finds that controlling blood pressure can reduce cardiovascular risks in patients with chronic kidney disease, but careful treatment is needed to avoid kidney harm.
Contribution
The study systematically evaluates the effectiveness of blood pressure interventions in reducing cardiovascular events among CKD patients.
Findings
Intensive blood pressure control significantly reduces cardiovascular events in CKD patients.
RAAS blockers and SGLT2 inhibitors show cardiovascular benefits but may increase risks like acute kidney injury.
Nutraceuticals demonstrate potential anti-inflammatory and BP-lowering effects.
Abstract
Cardiovascular disease remains the leading cause of morbidity and mortality in patients with chronic kidney disease (CKD), with hypertension, common in this population, contributing significantly to vascular damage and cardiovascular risk. This systematic review evaluates the impact of blood pressure (BP) control on cardiovascular outcomes in individuals with CKD. A comprehensive search of PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Scopus, and Web of Science up to May 5, 2025, identified randomized controlled trials (RCTs) and prospective comparative studies assessing BP interventions and cardiovascular outcomes in CKD populations. Methodological quality was appraised using the Modified Downs and Black checklist. Of the 11,606 studies screened, 10 met the inclusion criteria. Interventions included intensive BP targets, renin-angiotensin-aldosterone system (RAAS)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
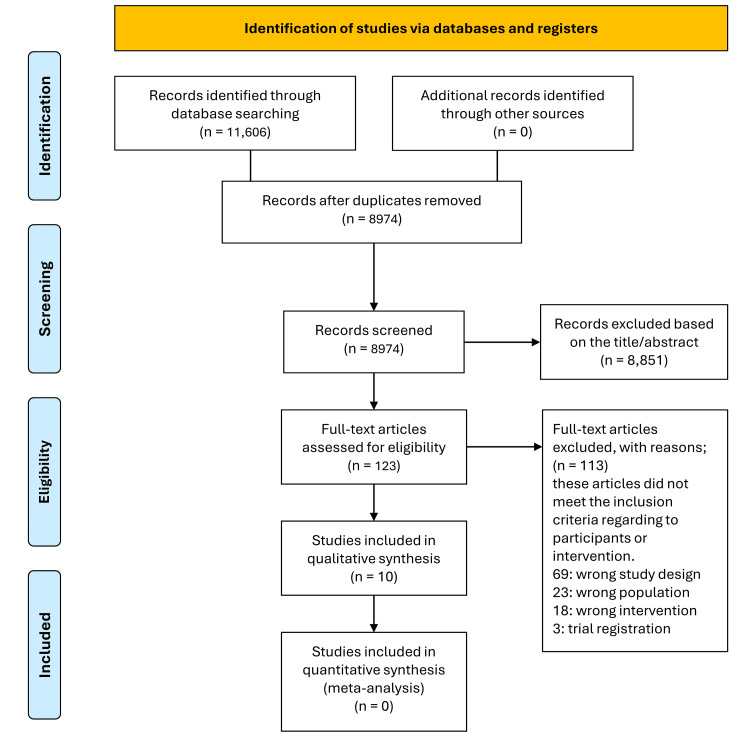 Figure 1
Figure 1| Author(s), Year | Study design | Country | Participants | CKD stage/type | Intervention | Comparator | Outcomes | Results |
| Hammer et al., 2019 [ | RCT (Double-blind, placebo-controlled) | Germany | 97 patients (50 Spironolactone, 47 Placebo); Mean age 60.3 ± 13.2 yrs | ESRD on hemodialysis | Spironolactone 50 mg daily for 40 weeks | Placebo daily for 40 weeks | Primary: LVMi change; Secondary: BP, LVEF, walk test, NYHA class, hyperkalemia, renal function | No significant LVMi change; hyperkalemia more frequent in treatment group; 0 deaths in treatment vs 4 in placebo group |
| Al Hamarneh et al., 2017 [ | Subgroup analysis of RCT (RxEACH) | Canada | 290 CKD patients (147 intervention, 143 control); Mean age ~61 yrs | eGFR <60 or ACR ≥3 mg/mmol | Pharmacist-led CV risk management | Usual care | CV risk score, BP, LDL, HbA1c, smoking cessation, medication use | CV risk ↓20%, SBP ↓10.5 mmHg, LDL ↓0.2 mmol/L, HbA1c ↓0.7%; more med adjustments in intervention |
| Barati Boldaji et al., 2020 [ | Randomized crossover trial | Iran | 41 ESRD patients on hemodialysis; Age 24–65 yrs | ESRD on hemodialysis | Pomegranate juice 100 mL 3×/week for 8 weeks | Usual care (crossover) | BP, lipids, IL-6, MDA, TAC | SBP/DBP ↓; IL-6 & MDA ↓; HDL & TAC ↑; LDL unchanged |
| Ng et al., 2016 [ | Feasibility RCT (Double-blind, placebo-controlled) | UK | 16 randomized; Target CKD stage 3 | Stage 3 CKD, non-diabetic | Spironolactone 25 mg daily for 40 weeks | Placebo | Arterial stiffness (PWV), hyperkalemia, renal function | Trial terminated early due to poor recruitment; feasibility data only |
| Cheung et al., 2017 [ | RCT (SPRINT subgroup analysis) | United States | 2646 CKD patients; Mean age 72 yrs | Stage 3 CKD (eGFR 20–59), non-diabetic | Intensive SBP target <120 mmHg | Standard SBP <140 mmHg | CVD events, mortality, eGFR decline, SAEs | HR for CVD 0.81; all-cause death HR 0.72; more renal decline and hyperkalemia in intensive group |
| Zinellu et al., 2016 [ | RCT | Italy | 24 patients with stage 3–4 CKD; Mean age 60 yrs | Stage 3–4 proteinuric CKD | Telmisartan + Ramipril for 6 months | Telmisartan alone | PSH, IMT, BP, proteinuria | IMT ↓, BP ↓, PSH ↑ with combination therapy; no GFR change |
| Mayne et al., 2024 [ | RCT (Double-blind, EMPA-KIDNEY substudy) | UK & Germany | 660 CKD patients; Mean age 64 yrs | eGFR ≥20 to <45, or 45–90 with uACR ≥200 mg/g | Empagliflozin 10 mg daily for 18 months | Placebo | Fluid overload (bioimpedance), CV events, weight, BP | Fluid overload ↓0.24 L; SBP ↓2.6 mmHg; CV composite HR 0.91 (NS) |
| Saengpanit et al., 2018 [ | RCT (Open-label) | Thailand | 50 ESRD patients on hemodialysis; Mean age ~52 yrs | ESRD on hemodialysis | Sodium thiosulfate IV 12.5 g twice weekly for 6 months | Usual care | CAVI, cfPWV, CAC, hsCRP, hemodynamics | CAVI ↓0.53, cfPWV ↓0.93 m/s, CAC stable; few mild side effects |
| Wu et al., 2015 [ | RCT (Double-blind, placebo-controlled) | United States | 33 ESRD patients on hemodialysis; Mean age ~54 yrs | ESRD on hemodialysis | Pomegranate extract 1000 mg daily for 6 months | Placebo | BP, CIMT, PWV, CRP, IL-6, PON-1 activity, physical function | SBP ↓24 mmHg, DBP ↓10 mmHg (NS after adjustment); lactonase ↑27%; other outcomes unchanged |
| Vaduganathan et al., 2020 [ | Post hoc analysis of RCT (SPRINT-HF substudy) | United States | 9361 participants (28.4% with eGFR <60); Mean age 66–72 yrs | CKD stages 1–3 (excluded if eGFR <20 or proteinuria >1 g/day) | Intensive SBP <120 mmHg | Standard SBP <140 mmHg | HF events, HF/CV death | HF risk ↑ with lower eGFR and higher UACR; HR for HF in eGFR <60 & UACR >300 = 8.40; treatment effect consistent (P> 0.05) |
| Study | Reporting | External validity | Internal validity – Bias | Internal validity – Confounding | Power | Total |
| Hammer et al., 2019 [ | 10 | 2 | 6 | 6 | 1 | 25 |
| Al Hamarneh et al., 2017 [ | 10 | 3 | 7 | 6 | 1 | 27 |
| Barati Boldaji et al., 2020 [ | 10 | 2 | 6 | 5 | 1 | 24 |
| Ng et al., 2016 [ | 9 | 2 | 5 | 5 | 0 | 21 |
| Cheung et al., 2017 [ | 10 | 3 | 7 | 6 | 1 | 27 |
| Zinellu et al., 2016 [ | 10 | 2 | 6 | 5 | 1 | 24 |
| Mayne et al., 2024 [ | 10 | 3 | 7 | 6 | 1 | 27 |
| Saengpanit et al., 2018 [ | 9 | 2 | 6 | 5 | 1 | 23 |
| Wu et al., 2015 [ | 9 | 2 | 6 | 5 | 0 | 22 |
| Vaduganathan et al., 2020 [ | 10 | 3 | 7 | 6 | 1 | 27 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Pressure and Hypertension Studies · Heart Rate Variability and Autonomic Control · Heart rate and cardiovascular health
Introduction and background
Chronic kidney disease (CKD) affects approximately 10% of the global population and is closely linked to increased cardiovascular morbidity and mortality [1,2]. Cardiovascular disease is the leading cause of death in this group, as patients with CKD face a significantly higher risk of cardiovascular events compared to the general population [3,4]. The decline in renal function adversely affects vascular health, necessitating proactive strategies to reduce cardiovascular risk.
Hypertension, present in most individuals with CKD, is both a cause and consequence of the disease [5,6]. Poor blood pressure control (BP) accelerates kidney damage and contributes to vascular remodeling, atherosclerosis, and left ventricular hypertrophy, key drivers of cardiovascular events [7,8]. Consequently, BP management is a central focus of CKD care guidelines, with recommendations tailored to disease stage and comorbidities. According to the most recent Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, the comprehensive management of CKD involves three therapeutic pillars: BP control, renin-angiotensin-aldosterone system (RAAS) inhibition using angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs), and reduction of proteinuria. ACE inhibitors and ARBs play a foundational role, particularly in patients with albuminuria, due to their dual benefits in lowering BP and mitigating glomerular injury, thereby slowing CKD progression and reducing cardiovascular risk [1-5].
Large clinical trials have shown that lowering systolic BP reduces cardiovascular events in high-risk groups [9,10]. However, the ideal target in CKD remains debated due to potential adverse effects, especially with intensive control strategies. According to the 2021 KDIGO guidelines, a target systolic BP of <120 mmHg is recommended for most patients with CKD (not on dialysis), provided it can be achieved safely, using standardized office BP measurements [11].
Various interventions are used to manage hypertension in CKD, including RAAS inhibitors, sodium-glucose co-transporter-2 (SGLT2) inhibitors, and lifestyle changes [12,13]. Their efficacy and safety can differ based on CKD stage, comorbidities, and treatment intensity, highlighting the need for individualized approaches.
This systematic review aims to evaluate and synthesize evidence from randomized controlled trials (RCTs) and prospective studies on the impact of BP control on cardiovascular outcomes in CKD. It also identifies gaps in the literature to guide future research.
Review
Methods
Literature Search Strategy
This systematic review was conducted and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [14]. A comprehensive search was performed in PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Scopus, and Web of Science, covering all studies published up to May 5, 2025. The strategy used controlled vocabulary (e.g., MeSH terms) and free-text keywords combined with Boolean operators to maximize sensitivity and relevance. The PubMed search string included: (“Hypertension”[Mesh] OR “Blood Pressure”[Mesh] OR “blood pressure control” OR “blood pressure lowering” OR antihypertensive OR “intensive blood pressure control”) AND (“Kidney Diseases”[Mesh] OR “Chronic Kidney Disease” OR CKD OR “renal insufficiency” OR “end-stage renal disease” OR ESRD) AND (“Cardiovascular Diseases”[Mesh] OR “Cardiovascular Events” OR “Heart Failure” OR “Myocardial Infarction” OR “Stroke” OR “Cardiovascular mortality”). Equivalent terms were adapted for other databases. Filters limited results to human adults and English-language publications. Reference lists of the included studies were also manually screened for additional relevant articles by two independent reviewers. Any disagreements were resolved through discussion or consultation with a third reviewer.
Eligibility Criteria
Studies were selected based on the PICO framework (Population, Intervention, Comparison, Outcome, Study design) [15]. We included RCTs and prospective comparative studies, published in English, that enrolled adult patients with CKD stages 3 to 5 or those undergoing dialysis. Interventions comprised any BP control strategy, pharmacological, target-based (e.g., intensive systolic BP control), or non-pharmacological. Comparators included usual care, placebo, or alternative antihypertensive regimens. Studies needed to report at least one cardiovascular outcome such as myocardial infarction, heart failure, stroke, cardiovascular mortality, or validated surrogate markers like arterial stiffness or left ventricular mass index. However, we acknowledge that our initial search string did not explicitly include these terms, which may have limited the identification of studies primarily focused on these surrogate endpoints. Exclusions included case reports, case series, reviews, editorials, conference abstracts, trial registrations, animal studies, and non-English publications.
Data Extraction
Full texts of 10 studies meeting the inclusion criteria were reviewed. Extracted data included study design, country, sample size, CKD stage, BP intervention details (drug class, dose, duration), comparator groups, outcome measures (cardiovascular events, mortality, surrogate markers), and key findings. Any discrepancies were resolved through reviewer discussion.
Quality Appraisal
Methodological quality was assessed independently by two reviewers using the Modified Downs and Black checklist [16], which evaluates 27 items across five domains: reporting, external validity, internal validity (bias and confounding), and statistical power. Studies were classified as excellent (26-28 points), good (20-25 points), fair (15-19 points), or poor (≤14 points). Any scoring disagreements were resolved by consensus.
Results
Study Selection
The systematic search identified 11,606 records from PubMed (1,475), Cochrane Library (2,646), Scopus (2,980), and Web of Science (4,505). After removing duplicates, 8,974 records were screened by title and abstract, and 8,851 were excluded as being irrelevant. Of the 123 full-text articles assessed, 113 were excluded for not meeting the inclusion criteria. Ten studies [17-26] were included in the qualitative synthesis. The PRISMA flow diagram details the selection process (Figure 1).
PRISMA flowchart for the search and selection of the studies
Study Characteristics
Studies were conducted across various countries, including Germany [17], Canada [18], Iran [19], the UK [20], Italy [22], Thailand [23], and the US [21,24-26]. Most were RCTs with double-blind, placebo-controlled, or crossover designs. Two were secondary analyses of the Systolic Blood Pressure Intervention Trial (SPRINT) trial [21,26]. Sample sizes ranged from 16 to over 9,000 participants. Participants were adults with CKD stages 3-5 or end-stage renal disease (ESRD) receiving dialysis, aged approximately 50 to 72 years, with a slight male predominance. Although some included studies reported participants with earlier stages of CKD (stages 1-2), the eligibility criteria for this review were restricted to stages 3-5 and dialysis-dependent ESRD. Stratification by kidney function (estimated glomerular filtration rate (eGFR), albuminuria) was common in subgroup analyses (Table 1).
Interventions included pharmacological agents such as spironolactone [17,20], telmisartan plus ramipril [22], and empagliflozin [25], alongside non-pharmacological approaches like pomegranate supplementation [19,24], intravenous sodium thiosulfate [26], and pharmacist-led cardiovascular risk management [18]. Comparators were standard care or placebo; SPRINT studies compared intensive versus standard BP targets. Outcomes covered cardiovascular events, vascular and renal surrogate markers, BP, and inflammatory markers.
Quality Assessment
As per the Modified Downs and Black checklist, study quality was generally high. Most studies scored well on reporting (up to 10/10) and internal validity (up to 7/7). External validity varied, with lower scores in small or single-center trials [19,22,24]. Some studies had limitations such as early termination [20] or lack of power calculations [19,24]. The highest quality scores (27/28) were observed in three studies [18,21,25]. Overall evidence quality was strong with minor variability due to study size and setting (Table 2).
Effect of Interventions
Intensive systolic BP control (<120 mmHg) reduced all-cause mortality (hazard ratio or HR 0.72) and showed a non-significant trend toward fewer cardiovascular events [21]. Spironolactone showed no benefit on left ventricular mass or ejection fraction in ESRD [17]. Combination of telmisartan and ramipril reduced carotid intima-media thickness [19]. Sodium thiosulfate decreased arterial stiffness and stabilized coronary calcification [26].
Systolic BP reductions were largest in intensive control (−12.3 mmHg) [21] and pomegranate juice (−10.2 mmHg) groups [19]. Pomegranate extract initially lowered systolic and diastolic BP but this lost significance after adjustment [21]. Telmisartan/ramipril significantly reduced BP; monotherapy did not [22]. Empagliflozin caused modest BP reductions [25], pharmacist-led interventions improved systolic BP [18], whereas spironolactone showed no significant BP changes [17,20].
Intensive BP control increased rapid renal decline but not ESRD or severe estimated glomerular filtration rate (eGFR) deterioration [21]. Empagliflozin reduced extracellular fluid overload and loop diuretic use [25]. Sodium thiosulfate did not affect calcium, phosphate, or parathyroid hormone (PTH) levels [26]. RAAS therapies and spironolactone did not significantly change creatinine, proteinuria, urine volume, or GFR [17,22].
Pomegranate supplementation lowered inflammatory and oxidative stress markers IL-6 and malondialdehyde (MDA), increased high-density lipoprotein (HDL) and antioxidant capacity [19]. Pomegranate extract raised antioxidant enzyme activity but did not affect CRP or other markers [24]. Sodium thiosulfate showed a non-significant high-sensitivity CRP decrease [26], empagliflozin improved HbA1c and hematocrit [25], and pharmacist-led care improved glycemic and lipid profiles [18].
Safety profiles varied: intensive BP control increased risks of acute renal failure, hyperkalemia, and hypotension [21], whereas spironolactone increased moderate hyperkalemia events [17]. RAAS combination therapy and sodium thiosulfate showed no serious safety issues [22,26]. Pomegranate treatments were well tolerated [16,21]. Similarly, empagliflozin and pharmacist-led interventions reported good adherence and a few adverse events [18,25].
Discussion
This systematic review of 10 studies demonstrates that targeted BP management in CKD patients is linked to improved cardiovascular outcomes, including reductions in myocardial infarction, heart failure, and cardiovascular mortality. Interventions focusing on intensive systolic BP control below conventional thresholds, whether pharmacological or structured approaches, showed the most pronounced benefits. These findings support the established understanding that effective BP control is crucial to mitigating cardiovascular risk in CKD populations. Most interventions were associated with reductions in systolic BP, with agents such as RAAS inhibitors, SGLT2 inhibitors, and dietary supplements like pomegranate extract demonstrating modest but statistically significant effects in individual studies. However, given the heterogeneity of study designs, populations, and outcome measures, a formal meta-analysis was not performed, limiting the ability to quantitatively synthesize these findings.
Renal outcomes were more variable, with some studies reporting stable or improved renal markers, while others raised concerns about accelerated decline in kidney function or acute kidney injury following intensive BP lowering. This highlights the ongoing clinical challenge of balancing cardiovascular benefits with potential renal risks in CKD management. Additionally, some studies suggested a potential link between BP control and reductions in inflammatory and oxidative stress markers, though evidence remains inconsistent. Safety profiles varied among interventions, with spironolactone and intensive BP reduction associated with higher rates of hyperkalemia and hypotension, underscoring the need for careful patient monitoring. Overall, these findings emphasize that individualized therapy, considering both cardiovascular and renal risks, is essential in optimizing BP management strategies for patients with CKD.
Further large-scale, long-term randomized controlled trials are essential to determine the optimal BP targets in CKD, particularly given the ongoing debate between intensive versus standard control strategies. Existing evidence often derives from heterogeneous populations and surrogate outcomes, limiting its generalizability. Moreover, few studies have stratified patients by CKD stage, presence of albuminuria, or dialysis status, despite the potential for differential responses to treatment. Future research should also aim to assess patient-centered outcomes such as cardiovascular mortality, progression to ESRD, and quality of life, while ensuring representation of key subgroups, including elderly patients and those with diabetic nephropathy. Additionally, trials incorporating newer antihypertensive agents, including SGLT2 inhibitors and mineralocorticoid receptor antagonists, could provide insights into synergistic or comparative effectiveness in various CKD stages.
A notable limitation of this review is the retrospective registration of the protocol on the International Prospective Register of Systematic Reviews (PROSPERO). Although the methodology was defined prior to data extraction and is transparently reported, the lack of prospective registration may reduce confidence in the review’s objectivity. We also acknowledge that restricting the search to English-language publications introduces a potential language bias, which could limit the comprehensiveness and generalizability of our findings. Additionally, while validated surrogate markers such as arterial stiffness and left ventricular mass index were considered eligible outcomes, our initial search strategy did not explicitly include terms for these markers. As a result, some relevant studies focusing on these endpoints may have been missed. To partially mitigate this, we manually screened the reference lists of included studies; however, the possibility of missing pertinent articles remains a limitation.
Conclusions
This systematic review underscores the importance of targeted BP control in reducing cardiovascular risk among patients with CKD. Interventions, ranging from pharmacological therapies such as RAAS and SGLT2 inhibitors to non-traditional approaches like nutraceuticals, demonstrated varying degrees of effectiveness in lowering BP and improving cardiovascular outcomes. While intensive BP control is linked to reductions in cardiovascular events and mortality, it may increase the risk of renal adverse effects, particularly in advanced CKD. Overall, individualized BP management that balances cardiovascular benefits with renal safety is essential. Further large-scale, long-term studies are needed to establish optimal BP targets and identify the safest and most effective interventions across different stages of CKD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010 Kidney Int Mills KT Xu Y Zhang W 9509578820152622175210.1038/ki.2015.230PMC 4653075 · doi ↗ · pubmed ↗
- 2Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017 Lancet GBD Chronic Kidney Disease Collaboration 70973339520203206131510.1016/S 0140-6736(20)30045-3PMC 7049905 · doi ↗ · pubmed ↗
- 3Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization N Engl J Med Go AS Chertow GM Fan D Mc Culloch CE Hsu CY 1296130535120041538565610.1056/NEJ Moa 041031 · doi ↗ · pubmed ↗
- 4Clinical epidemiology of cardiovascular disease in chronic renal disease Am J Kidney Dis Foley RN Parfrey PS Sarnak MJ 0932199810.1053/ajkd.1998.v 32.pm 98204709820470 · doi ↗ · pubmed ↗
- 5Hypertension in CKD: core curriculum 2019 Am J Kidney Dis Ku E Lee BJ Wei J Weir MR 1201317420193089836210.1053/j.ajkd.2018.12.044 · doi ↗ · pubmed ↗
- 62017 ACC/AHA/AAPA/ABC/ACPM/AGS/A Ph A/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines J Am Coll Cardiol Whelton PK Carey RM Aronow WS 024871201810.1016/j.jacc.2017.11.00629146535 · doi ↗ · pubmed ↗
- 7Effects of blood pressure level on progression of diabetic nephropathy: results from the RENAAL study Arch Intern Med Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ Brenner BM 1555156516320031286057810.1001/archinte.163.13.1555 · doi ↗ · pubmed ↗
- 8Management of hyperkalemia in patients with kidney disease: a position paper endorsed by the Italian Society of Nephrology J Nephrol Bianchi S Aucella F De Nicola L Genovesi S Paoletti E Regolisti G 4995163220193111968110.1007/s 40620-019-00617-y PMC 6588653 · doi ↗ · pubmed ↗