Comparative Evaluation of the Cavity Preparation Design on Mandibular First Molars in Typodont Teeth After Neurosculpting in Undergraduate Dental Students
Khushi A Desai, Khyati G Pandya, Ankit Arora, Sonali Kapoor, Harshil R Bhadang

TL;DR
This study shows that neurosculpting exercises improve dental students' cavity preparation skills on typodont teeth.
Contribution
Demonstrates the effectiveness of neurosculpting exercises in enhancing psychomotor skills in dental education.
Findings
The experimental group showed significant improvement in cavity preparation scores after neurosculpting exercises.
NSE led to statistically significant improvements in outline form and undercut scores.
NSE had a more pronounced effect on the experimental group compared to the control group.
Abstract
Introduction Psychomotor skill development forms the cornerstone of competency in procedure-oriented professions, and dentistry is no exception. The dental practice is a complex interplay of neuroplastic abilities encompassing fine motor control, dexterity, visuospatial awareness, precise visuomotor coordination, finger dexterity, hand-arm steadiness, and multi-limb coordination for executing intricate procedures. Neuroplasticity is neuronal plasticity of the brain that occurs during learning motor skills. Hence, optimizing training methods becomes paramount. This study explores the potential of neurosculpting exercises (NSE) to enhance dental education by specifically targeting fine motor skills, dexterity, and neuromuscular coordination. The study aimed to evaluate the effects of the difference in class one cavity preparation design on typodont teeth done by undergraduate students…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
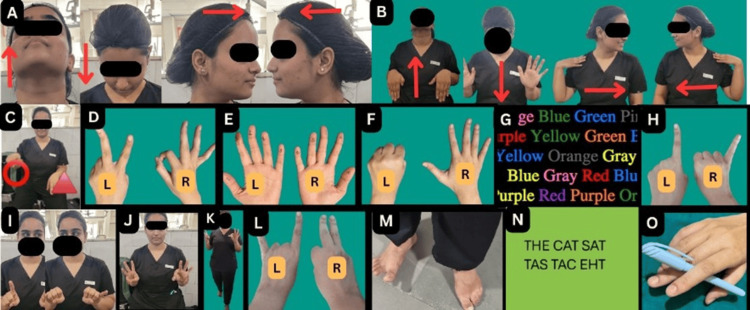 Figure 1
Figure 1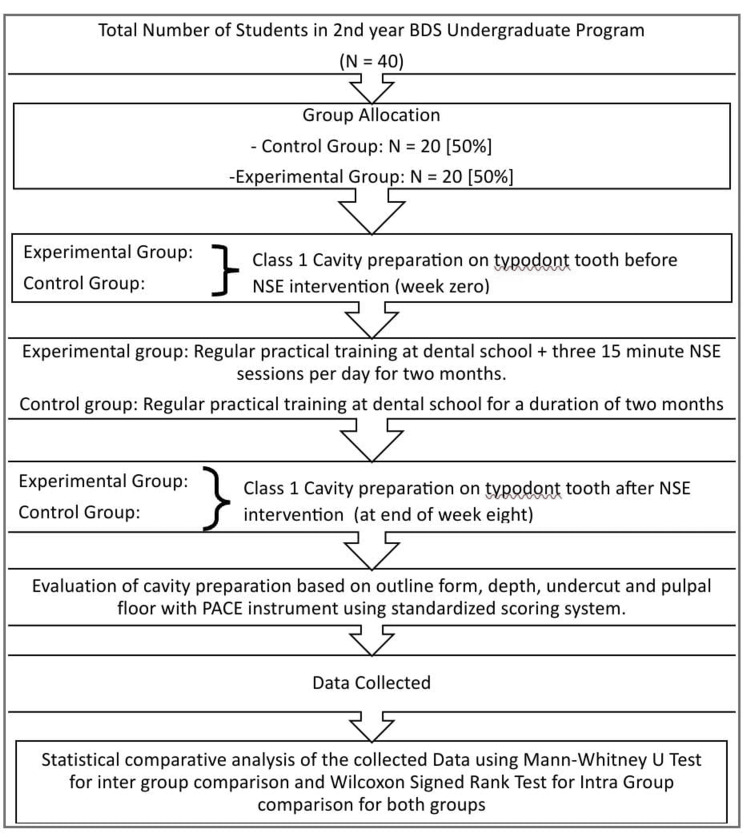 Figure 2
Figure 2| Name of exercise | Technique | Enhancer |
| Exercise 1: head exercise (A) | Move the head gently-up, down, left, and right | Builds focused attention |
| Exercise 2: arm-head exercises (B) | With both your arms raised in front of you (front raise) and the palms facing toward you and wrists down, slowly move your head up, then the head moves down, the palms facing away, wrists up. When the head moves to the right, the hand touches the left shoulder, and when the head moves to the left, the hand touches the right shoulder. Gradually increase speed | Focus enhancer |
| Exercise 3: circle-triangle exercise (C) | With both arms extended, draw a circle in the air with your right hand while simultaneously drawing a triangle with your left hand. Move in a clockwise direction and gradually increase speed (air drawing) | Brain engagement |
| Exercise 4: OK-peace hand sign exercise (D) | Make an "OK" sign with your right hand and a "peace" sign with your left hand. Quickly switch the signs between your hands, maintaining the opposite symbol in each hand. Increase speed as you become more comfortable | Mental challenge |
| Exercise 5: five-on-finger exercise (E) | Numbers 1 to 5 are randomly written on the fingers of both hands (in a different order). Starting from thumb to pinky finger, left hand: 1-4-2-3-5 and right hand: 4-1-2-5-3. The trainer calls out the numbers from 1 to 5 and 5 to 1. The students raise their fingers for the corresponding number | Increases focus and boosts neuroplasticity |
| Exercise 6: open-closed finger exercise (F) | The left hand forms a fist, while the right palm is open. The left hand will open fingers in the following order: pinky, ring, middle, index, and thumb. The right hand is open, and the fingers are closed one at a time in the following order: thumb, index, middle, ring, and pinky. Begin by softly moving one hand at a time, then both hands together. Gradually increase speed | Focused attention |
| Exercise 7: Stroop test (G) | Flashcards display a succession of words written in a variety of font colors. Students must vocally identify the hue of the font. They are not required to say the word, only the color of the font. The first round is slower, and the second is faster | Selective attention |
| Exercise 8: index pinky raise exercise (H) | Raise the right index finger while keeping the remaining fingers closed like a fist. Raise the left pinky finger while keeping the remaining fingers closed like a fist. Then, swap by raising the right pinky finger while keeping the remaining fingers closed like a fist, and the left index finger while keeping the remaining fingers closed like a fist. Begin with each hand slowly, one by one. Then both hands are brought together at the same time, and the speed is increased | Improves concentration |
| Exercise 9: finger-eye coordination exercise (I) | Do it without moving your head. The right index finger is raised, and the eyes look left. The left pinky finger is raised, and the eyes look to the right. Swap this finger pattern between the hands for 1 minute. The head should be kept straight and not moved. Do not look too far in one direction to avoid eye strain | Focused attention, stimulation of both sides of the brain, and builds brain resilience |
| Exercise 10: thumb-finger touch exercise (J) | Initiate the exercise using your right hand, bringing your thumb to touch the tip of each finger, starting with the index finger and progressing toward the pinky. Then perform the same action with your left hand, touching your thumb to the fingertips in reverse order, commencing with the pinky and concluding with the index finger. Begin using one hand at a time. Exercise with both hands simultaneously, gradually increasing the speed. Then, exercise with your palms facing downward | Develops focus and concentration |
| Exercise 11: thumb-finger step-up exercise (K) | Coordinate a walking-in-place exercise that includes alternating thumb-to-fingertip touches. Start by taking three steps forward while touching your right thumb to each fingertip in order (starting with the index and moving to the pinky) and simultaneously touching your left thumb to each fingertip in reverse order (starting with the pinky and moving to the index). After completing this, repeat the process while moving three steps backward | Increases complexity and brain challenge |
| Exercise 12: horn-finger exercise (L) | To form a "horn sign," extend your right hand's index and pinky fingers while extending the middle and ring fingers of your left hand. Start by practicing with each hand separately, then alternate the hand positions | Concentration booster |
| Exercise 13: foot-heel-toe exercise (M) | Point your right foot outward, heel down, toes up. Point your left foot outward, toes down and heel up. Start by practicing each foot movement separately. Next, practice both moves together and gradually increase the pace | Builds focus, resilience, and coordination |
| Exercise 14: reverse writing exercise (N) | Choose a simple sentence and write it down normally. Then, try writing the same sentence backwards, letter by letter. Simple sentence: "The cat sat." Backward: "tas tac ehT" | Mental agility |
| Exercise 15: pen rolling exercise (O) | Keep a pen between your thumb and index finger. Roll the pen around your palm, beginning with your index finger and progressing to each finger in order (index to pinky). Then, roll the pen back to your index finger | Dexterity and focus |
| Days | Old exercises | New exercises |
| Day 1-Day 4 | Exercise 1 | |
| Day 5-Day 8 | Day 4 | Exercise 2 |
| Day 9-Day 12 | Day 8 | Exercise 3 |
| Day 13-Day 16 | Day 12 | Exercise 4 |
| Day 17-Day 20 | Day 16 | Exercise 5 |
| Day 21-Day 24 | Day 20 | Exercise 6 |
| Day 25-Day 28 | Day 24 | Exercise 7 |
| Day 29-Day 32 | Day 28 | Exercise 8 |
| Day 33-Day 36 | Day 32 | Exercise 9 |
| Day 37-Day 40 | Day 36 | Exercise 10 |
| Day 41-Day 44 | Day 40 | Exercise 11 |
| Day 45-Day 48 | Day 44 | Exercise 12 |
| Day 49-Day 52 | Day 48 | Exercise 13 |
| Day 53-Day 56 | Day 52 | Exercise 14 |
| Day 57-Day 60 | Day 56 | Exercise 15 |
| Outline form | Depth | Undercut | Pulpal floor orientation | |
| Student 01 | ||||
| Student 02 | ||||
| Student 03 |
| Before the NSE intervention: cavity preparation variables | Group | Mann-Whitney U | p-value | |||
| Control N = 20 (50%) | Experimental N = 20 (50%) | |||||
| Mean | SD | Mean | SD | |||
| Outline | 5.35 | 1.18 | 5.36 | 1.07 | 179 | 0.976 |
| Depth | 5.25 | 1.33 | 5.17 | 1.61 | 171 | 0.79 |
| Undercut | 5.50 | 1.53 | 5.14 | 1.35 | 146 | 0.318 |
| Pulpal | 5.62 | 1.27 | 5.89 | 1.31 | 152 | 0.4 |
| After the NSE intervention: cavity preparation variables | Group | p-value | ||||
| Control N = 20 (50%) | Experimental N = 20 (50%) | Mann-Whitney U | ||||
| Mean | SD | Mean | SD | |||
| Outline | 4.98 | 0.83 | 6.22 | 1.06 | 64.5 | 0.001* |
| Depth | 5.23 | 0.90 | 6.50 | 1.10 | 67 | 0.001* |
| Undercut | 5.10 | 1.01 | 6.67 | 1.01 | 52 | <0.001* |
| Pulpal | 5.17 | 0.92 | 6.47 | 1.08 | 66 | 0.001* |
| Total | 20.47 | 2.95 | 25.86 | 3.86 | 44.5 | <0.001* |
| Group | Cavity preparation variables | Before NSE intervention | After NSE intervention | p-value | ||
| Mean | SD | Mean | SD | |||
| Control | Outline | 5.35 | 1.18 | 4.98 | 0.83 | 0.113 |
| Depth | 5.25 | 1.33 | 5.23 | 0.90 | 0.931 | |
| Undercut | 5.50 | 1.53 | 5.10 | 1.01 | 0.208 | |
| Pulpal | 5.62 | 1.27 | 5.17 | 0.92 | 0.121 | |
| Total | 21.73 | 4.41 | 20.47 | 2.95 | 0.09 | |
| Experimental | Outline | 5.36 | 1.07 | 6.22 | 1.06 | 0.004* |
| Depth | 5.17 | 1.61 | 6.50 | 1.10 | 0.001* | |
| Undercut | 5.14 | 1.35 | 6.67 | 1.01 | 0.002* | |
| Pulpal | 5.89 | 1.31 | 6.47 | 1.08 | 0.152 | |
| Total | 21.56 | 4.36 | 25.86 | 3.86 | 0.001* | |
| Cavity preparation variables | Group | Mann-Whitney U | p-value | |||
| Control (N = 20) (50%) | Experimental (N = 20) (50%) | |||||
| Mean | SD | Mean | SD | |||
| Outline | -0.38 | 1.04 | 0.86 | 1.01 | 71 | 0.001* |
| Depth | -0.02 | 1.55 | 1.33 | 1.36 | 90 | 0.008* |
| Undercut | -0.40 | 1.30 | 1.53 | 1.53 | 62 | 0.001* |
| Pulpal | -0.45 | 1.17 | 0.58 | 1.50 | 108.5 | 0.034* |
| Total | -1.25 | 3.09 | 4.31 | 4.35 | 46 | <0.001* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Anxiety and Anesthesia Techniques
Introduction
Learning psychomotor skills necessitates the use of more creative teaching techniques, as these skills encompass both a cognitive/knowledge aspect and a motor aspect, unlike purely cognitive learning [1]. Mastering intricate psychomotor skills is a vital proficiency in dental training. The field of dentistry requires exceptional precision and expertise that necessitate the cultivation of cognitive development, unique dexterity, and motivation, all of which impact motor execution [2]. The progression from novice to specialist entails repeated practice and exposure to facilitate the formation of neuronal links in the brain. It will lead to the automation of the rehearsed movements [3]. This study investigates the potential benefits of combining neurosculpting with preclinical exercises for enhancing fine psychomotor skills. These findings aim to contribute to a growing understanding of how these techniques can work to improve mental agility and control. The brain's capacity for rewiring itself, called neuroplasticity [4], might be the advantage behind observational learning [5]. Since both involve forming new connections, this suggests that neuroplasticity could be critical for improving dexterity and fine motor skills just by watching others perform. Neurosculpting^®^ is the fusion of brain science and mindfulness, wherein Lisa Wimberger teaches few-minute exercises that trigger parts of the brain to activate the prefrontal cortex [6,7]. These exercises aim to improve focus, prefrontal brain activity, and resilience, all of which can strengthen psychomotor skills. They target different brain functions by coordinating physical movements with mental tasks. This neurosculpting exercise (NSE) was designed to develop visuospatial skills and hand-motor coordination relevant to cavity preparations. This is the first study to link neuroplasticity-inducing neurosculpting activities with dexterity skills in dentistry. This study is beneficial as it will help young dentists improve their dexterity abilities and aging dentists retain their dental expertise.
This study supports a fundamental revolution in dental education that prioritizes the development of outstanding psychomotor skills in future aspiring dentists. The aim is to create a standardized and skill-centric approach in the dental curriculum, thereby making practical expertise on par with theoretical knowledge, thereby enhancing the artistry part of dentistry.
Materials and methods
This experimental type of study was conducted from August 11, 2023, to October 20, 2023, in the Department of Conservative Dentistry and Endodontics at Manubhai Patel Dental College and Hospital and Research Center in Vadodara, Gujarat, India. Following approval from the Institutional Ethics Committee (IEC) for research (IEC/MPDC_289/CONS-54/23), the study sought the proposed intervention of NSE.
Aims and objectives
The aim of this study is to evaluate the difference in class one cavity preparation design on typodont teeth done by undergraduate students after NSE. This study investigates the intriguing potential of NSEs to improve dental education. Through the development of students' fine motor skills and neuromuscular coordination, these exercises can help students become even more skilled clinicians. This research has the potential to make a huge impact on dental education. A favorable outcome could revolutionize the field and establish neurosculpting as the driving force behind the breakthrough. The objectives of this study are primarily to evaluate the cavity preparation design (the outline form, depth, undercut, and pulpal inclination using the Perfected for Amalgam Cavity Evaluation (PACE) instrument) of the control and experimental groups before the NSE intervention at week zero, as well as to evaluate the cavity preparation designs for the similar parameters of both the control and experimental groups after the NSE intervention at the end of week eight. Finally, another objective is to compare the scores of both the control and experimental groups (intergroup and intragroup comparisons). The sample size was established based on the number of second-year dental students available during the study period. The sample size represents the entire cohort of students who were available and willing to participate in the study. All 40 second-year Bachelor of Dental Surgery (BDS) dental students were enrolled in the research study. The inclusion criteria were a match for baseline data for class one cavity preparation design with variables of outline form, depth, undercut, and pulpal floor.
All the students (N = 40, 100%) did not have any neuromuscular abnormalities on examination. They were not on any medication or any drug dependency. All students provided written informed consent before the study. The even/odd approach was used to randomly divide all the students into two groups (N = 20, 50% for each group).
Group 1 (experimental group) consisted of 20 (N = 20, 50%) students with even-numbered roll numbers. They attended regular practical preclinical training at the dental school with three 15-minute NSE sessions per day.
The students followed the NSE schedule according to the level of difficulty. The NSE schedule followed a sequence that began with simple head-up-and-down exercises, then progressed to combining and synchronizing head movements with arm exercises, bimanual finger exercises, foot exercises, walking forward and backward doing hand exercises, and the gold standard Stroop test, culminating in the complete highest level of exercises of reverse handwriting and single-hand multiple-finger use by rolling a pen in between fingers (Figure 1). The technique of each exercise and the function that is strengthened are described below (Table 1). The experimental group of students performed these exercises with exquisite focus and proficiency. There was a defined schedule. The students began with Exercise No. 1 and continued it for four days (Day 1 to Day 4). A new NSE, Exercise 2, started on Day 5. Day 5's NSE schedule sequenced exercises from Day 4 and the new NSE for four days (Day 5 to Day 8). This pattern of exercises continued for 15 exercises (Exercises 1 to Exercise 15) up to 60 days (Table 2).
Picture collage illustrating the 15 neurosculpting exercises (NSEs) (A-O) performed by the experimental groupEach picture of the collage demonstrates the head/hand/finger/eyes (I)/legs (M)/walk (K)/Stroop test (G)/reverse writing (N) movements in the respective NSE performed by the experimental group. These NSEs were performed for 15 minutes, three times a day for two monthsThe arrows show the directions of head movements-up, down, left, and rightL: left hand; R: right handA: Exercise 1; B: Exercise 2; C: Exercise 3; D: Exercise 4; E: Exercise 5; F: Exercise 6; G: Exercise 7; H: Exercise 8; I: Exercise 9; J: Exercise 10; K: Exercise 11; L: Exercise 12; M: Exercise 13; N: Exercise 14; O: Exercise 15
Group 2 (the control group) had 20 (N = 20, 50%) students with odd-numbered roll numbers. They undertook regular preclinical practical training sessions at the dental school. These students did not participate in any NSE (Figure 2).
Flowchart illustrating the entire sequence of activities in the neurosculpting exercise (NSE) approachThe figure gives a brief outline of the selection process, procedure steps, and analysis providing a comprehensive overview of how the NSE was implemented in the studyBDS: Bachelor of Dental Surgery; PACE: Perfected for Amalgam Cavity Evaluation
Assessment of cavity preparation
The study employed a single-blinded design. That is to say, the two examiners who evaluated the participants were unaware of whether the student belonged to the NSE intervention group or the control group (received regular practical training only). The reliability of the scoring process was assessed for interexaminer reliability.
In baseline assessment, all students participated in a standardized class one cavity preparation on the right mandibular molar on the typodont tooth at week zero. After the NSE intervention, both groups again participated in standardized class one cavity preparation at the end of week eight. Both assessments were based on outline form, depth, undercuts, and pulpal floor inclination. Students' cavity configuration skills were evaluated with the PACE instrument [8] and using a standardized scoring system (Table 3).
After collecting the before and after intervention score data of both groups, data were assessed using non-parametric equivalents. The independent Student t-test or the Mann-Whitney U test was used for intergroup comparison, and the Wilcoxon signed-rank test was used to analyze intragroup differences. Statistical Package for the Social Sciences (SPSS) 20 software (IBM Corp., Armonk, NY, US) was used for the same.
The students were assessed based on the following marking scheme: 1-2: very poor; 3-4: poor; 5-6: acceptable; 7-8: very good; 9-10: excellent.
The intergroup and intragroup differences in parameters between control and experimental group students were compared using the independent Student t-test or the Mann-Whitney U test and the Wilcoxon signed-rank test depending on the distribution of data. SPSS 20 software (IBM Corp., Armonk, NY, US) was used for the same.
Results
The intergroup comparison before the intervention using the Mann-Whitney U test results yielded the control group’s (N = 20, 50%) cavity preparation design's outline to pulpal mean of range 5.35 to 5.62 (standard deviation (SD) = 1.18 to 1.27) and experimental group’s (N = 20, 50%) mean of range 5.36 to 5.89 (SD = 1.07 to 1.31) (statistically significant p < 0.05). The p-values of range 0.976 to 0.4 were non-significant p-values (all p > 0.05), indicating there were no statistically significant differences between the groups for any of the measures before the intervention. This suggests that the groups were comparable at baseline data concerning outline form, depth, undercut, and pulpal before the start of the study. The overall skill for both groups was at par (Table 4).
Table 4: Intergroup comparison before the NSE intervention using the Mann-Whitney U testSD: standard deviation; NSE: neurosculpting exerciseData have been represented as cavity preparation variables (outline, depth, undercut, and pulpal), mean deviation, SD, Mann-Whitney U values, and p-value of both groups before the NSE interventionp-value is considered significant at p < 0.05
The intergroup comparison of the cavity preparation parameters between the experimental and control groups after the intervention using the Mann-Whitney U test showed that the mean scores for all the variable range of 6.22 to 6.47 (SD = 1.06 to 1.08) and total score of 25.86 (SD = 3.86) were significantly higher in the experimental group than the control group whose mean scores were in the range of 4.98 to 5.17 (SD = 0.83 to 0.92) and total score of 20.47 (SD = 2.95). These indicate that the experimental group scored higher than the control group across all measures. This suggests that the NSE intervention had a substantial and statistically significant positive effect across all measured parameters. The p-values for all parameters were p < 0.001, indicating there was a significant statistical difference (statistically significant at p < 0.001) (Table 5).
Table 5: Intergroup comparisons after the NSE intervention using the Mann-Whitney U testSD: standard deviation; NSE: neurosculpting exercise*Significant valueData have been represented as cavity preparation variables (outline, depth, undercut, pulpal, and total), mean deviation, SD, Mann-Whitney U values, and p-value of both groups after NSE interventionp-value is considered significant at p < 0.05
The intragroup comparison shows that the changes in the control group both before and after intervention were generally mild, and none of these differences reached statistical significance as indicated by the p-values (all p > 0.05). In contrast, the experimental group showed statistically significant improvements after NSE intervention for outline, depth, undercut, and pulpal parameters, with p-values < 0.004, except for pulpal, which did not achieve significance. These results indicate that the intervention was effective in enhancing performance measures in the experimental group compared to the control group using the Wilcoxon signed-rank test (Table 6).
Table 6: Intragroup comparisons before and after NSE intervention using the Wilcoxon signed-rank testSD: standard deviation; NSE: neurosculpting exercise*Significant p-valueData have been represented as cavity preparation variables (outline, depth, undercut, pulpal, and total), mean deviation, SD, and p-valuep-value is considered significant at p < 0.05
The mean difference intergroup comparison using the Mann-Whitney U test detailed the analysis. The lowest p-value among the cavity preparation variables was for outline and undercut: 0.001. The highest p-value of pulpal was 0.034, whereas the overall total p-value was <0.001, which was significant. The mean differences along with statistically significant p-values (p < 0.05) confirm that the NSE intervention led to substantial and significant improvements in the cavity preparation exercises done by the experimental group compared to the control group (Table 7).
Table 7: Intergroup comparison based on mean differenceSD: standard deviation*Significant p-valueData have been represented as cavity preparation variables (outline, depth, undercut, pulpal, and total), mean deviation, SD, Mann-Whitney U values, and p-valuep-value is considered significant at p < 0.05
Discussion
Our study aimed to determine if combining NSE with preclinical training would enhance fine psychomotor skills and dexterity compared to preclinical training alone. We hypothesized that the combined approach would lead to a substantial improvement in mental agility and control during preclinical tasks. As expected, the group receiving NSE and regular preclinical dental training demonstrated a significant advantage in these skills compared to those who received only regular preclinical dental training. Researchers have proved through functional magnetic resonance imaging (fMRI) and repetitive transcranial magnetic stimulation (rTMS) that the areas of the brain involved in fine motor movements are the primary motor cortex, premotor cortex, presupplementary cortex, basal ganglia, supplementary cortex, posterior parietal cortex, and cerebellum [3]. The premotor complex mainly lies in the prefrontal area [9]. Neurosculpting is a process that involves triggering parts of our brain that we do not usually focus on. This activates the prefrontal cortex, which forms the basis for learning and mapping. It involves both hemispheres of the brain. When we combine mental activities with physical activities, it initiates the creation of new neural pathways [10]. Similarly, psychomotor skill learning is a combination of observation and practical learning, which is essential to refine a surgeon’s skills. Muscle memory and fine motor control develop through trial and error during procedures. This also creates new neural pathway connections in the brain, enabling more precise use of surgical instruments, thereby enhancing surgical skills [5]. fMRI shows different patterns of neural activity that occur in the prefrontal cortices, motor cortex, dorsal anterior cingulate gyrus, parietal gyrus, putamen, occipital gyrus, and cerebellum during motor activities. These new neural mechanisms engaged in motor performance and learning may inform NSE as novel interventions to enhance motor skill learning [11]. Dental schools give greater importance to theoretical knowledge, but our research suggests that there may be a potential training gap for developing important fine psychomotor practical skills. Second-year BDS students are a preferred group for participation in major educational research studies. Being early in their dental education (second year), these students have not formed ingrained habits yet. This allows researchers to assess the effectiveness of the training program without pre-existing biases. The evaluations by the examiners are less biased as it was a single-blinded study design. The intervention of NSE in our study included various essential parameters. Scientific research papers have shown that the schedule for NSE is based on repetitions, the number of sessions, and a stipulated time frame. Research reveals that mastering physical skills through brief bursts of practice interspersed with break periods is considerably more successful than pushing through lengthy sessions. Over time, NSE creates new brain pathways or connections. Some estimates place the NSEs’ duration at roughly eight weeks. Research has demonstrated that even very brief training regimens can have positive effects. Programs with 30 sessions, each lasting 10 minutes, can still be successful [4]. Scientists and physiologists draw on research and data that suggest the average attention span for effective learning is around 15 minutes. With this understanding, we have structured our exercises to last for 15 minutes, optimizing our learning potential during each session [12]. Movement science research indicates that strategically structuring work-rest cycles, with longer rest periods than work periods, enhances motor skill learning and performance [13]. Studies on skill acquisition further suggest that spaced practice, achieved through increased time between repetitions and sessions, improves fine motor skills [14]. Based on these findings, our training program incorporates three sessions of 15 minutes each. The findings suggest that rest periods should be longer than the actual work periods. A defined NSE schedule was followed according to the level of difficulty. NSE was structured as a sequential pattern/box pattern of learning. During learning trials, the researchers have found that blocked practice results in superior fine motor skill performance to random practice [15]. A study characterized stable motor patterns as similar to habits, which are defined as entrenched behaviors resistant to change through retraining [16]. This suggests that motor learning is a form of habit formation. Scientific evidence indicates that it takes a median of 59-66 days for individuals to reach peak automaticity in newly formed habits [17,18]. Finger exercises are done as "the brain allocates significant space to sensory information from the face and hand. Interestingly, the hand area has specific, non-overlapping regions for each finger" [19]. The experimental group’s class one cavity preparation parameters like outline, depth, and undercut showed improved scores after the NSE intervention. The pulpal floor showed no distinction, however. Following the intervention, there was a notable improvement in the overall score. There were only a few adjuncts that exhibited improvement. The standardized scoring system used to evaluate the students’ cavity preparation skills provided a clear and consistent method for examiners to score each student’s performance. The results indicated an improvement in psychomotor fine skills within the intervention group; the researchers planned to adhere to ethical principles by offering the same NSE training to the control group. Many efforts have been made to fill the void between undergraduate learning and the real world [20]. The present study is one step ahead and is aimed at working directly on the neural pathways.
A few methodological limitations must be acknowledged in our study. First and foremost, the study had a small sample size as the intake of the institute of one batch is 40 students for the second year. A future extension of this investigation to a larger cohort of subjects would generalize these findings. The adoption of the NSE technique as a part of dental curricular changes would demand a larger sample size. Furthermore, the study duration was only two months as motor learning and habit formation take a median of 59-66 days. A longer study duration would result in more evident neuroplastic changes in the brain thereby enhancing the precision of fine motor skills to a larger extent thereby measuring the long-term effects. Additionally, the surgical variant involved class one cavity preparation in a typodont tooth. The addition of other surgical variants would give more strength to the findings. The NSE was selected per recommendations by Lisa Wimberger [7]. However, multiple NSE other than the exercises in this study following the box sequential learning pattern would help in deeper neuroplasticity. Lastly, a subjective assessment of the effects of NSE and psychomotor skills was done. More objective assessment tools such as blood tests and neuroimaging tests-fMRI and rTMS-can directly measure the brain change and would be a stronger predictor of the neuroplastic changes in the brain.
Conclusions
The experiment yielded a breakthrough: the experimental group achieved significantly better cavity parameters (outline, depth, and undercuts) while minimizing gross errors. NSE improved and enhanced fine motor skills, leading to better results in complex tasks that require precision. Integrating preclinical exercises with neurosculpting techniques may equip future dentists with exceptional surgical precision and mastery. This comprehensive approach could elevate the spectrum of dental skills, ultimately leading to a new generation of highly proficient clinicians. Students entering dental school could have excellent theoretical knowledge but would be lacking in fine motor skills. Therefore, these NSEs could be a boon to refine their dexterity, thereby comprehending their theoretical knowledge. Further research includes neuroplasticity to enhance psychomotor skills for remedial students with poor dexterity. Psychomotor skills and dexterity are vital to dentistry. The aging dentists lose their fine dental skills. Hence, neuroplasticity and aging dentists could be other research topics of interest. This research lays the groundwork for further exploration of methods for achieving flawless results and optimizing dental skills for the best possible outcomes with a commitment to excellence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Psychomotor skill development: learning what and how to do Enhancing Patient Engagement in Pulmonary Healthcare: The Art and Science Blackstock F Pritchard S 2740 Humana Cham 2020
- 2Development of psychomotor skills in dentistry based on motor learning principles: a review World J Dent Khan S Inamdar MNK Munaga S 247251112020
- 3Development and retention of fine psychomotor skills: implications for the aging dentist J Can Dent Assoc Duong JK Gardner K Rucker LM 0762010 http://jcda.ca/article/a 2520633335 · pubmed ↗
- 4Effects of short-term training on behavioral learning and skill acquisition during intraoral fine motor task Neuroscience Kumar A Grigoriadis J Trulsson M Svensson P Svensson KG 101730620152616223810.1016/j.neuroscience.2015.06.065 · doi ↗ · pubmed ↗
- 5Observational learning in surgical skill development Indian J Surg Oncol Rao KN Arora RD Singh A Dange P Nagarkar NM 5405441420233790063610.1007/s 13193-023-01798-6PMC 10611665 · doi ↗ · pubmed ↗
- 6The impact of studying brain plasticity Front Cell Neurosci Mateos-Aparicio P Rodríguez-Moreno A 661320193087300910.3389/fncel.2019.00066 PMC 6400842 · doi ↗ · pubmed ↗
- 7Neurosculpting. Lisa’s story 5 2024 2021 https://www.neurosculpting.com/lisa-wimberger-story/
- 8A self-designed instrument to evaluate cavosurface angle for class I amalgam cavity preparation: a learning aid J Conserv Dent Arora A Acharya SR Ballal V Sharma P 253256152012 https://pmc.ncbi.nlm.nih.gov/articles/PMC 3410336/2287601310.4103/0972-0707.97951 PMC 3410336 · doi ↗ · pubmed ↗