Neonatal Hypoglycemia and Long-Term Pediatric Neurodevelopmental Outcomes: A Systematic Review
Rasha Fawzy Abdelmonem Mahrous, Sally Hassan Ali Hassanin, Raheeq Elssammani Elemam Elbashir, Hind Gasm Elseed, Sarra Elnour Ahmed Elnour, Nojoud Noureldayim Elsayid

TL;DR
This review examines how neonatal hypoglycemia affects children's long-term brain development and finds that severe cases are linked to developmental issues.
Contribution
The study provides a synthesis of 13 studies to clarify the long-term neurodevelopmental risks of neonatal hypoglycemia.
Findings
Severe neonatal hypoglycemia is associated with motor dysfunction and cognitive delays.
Mild hypoglycemia promptly treated does not consistently lead to neurodevelopmental deficits.
Standardized definitions and monitoring are needed to better understand and manage hypoglycemia in newborns.
Abstract
Neonatal hypoglycemia is a common metabolic disturbance with potentially significant implications for neurodevelopment, yet the long-term consequences are not completely understood. This systematic review synthesises evidence from 13 studies to evaluate the association between neonatal hypoglycemia and neurodevelopmental outcomes in children, examining the roles of severity, timing, and clinical management. A comprehensive search across PubMed, Embase, Scopus, and Web of Science yielded 260 records, with 13 studies meeting inclusion criteria after rigorous screening. Methodological quality was assessed using the Newcastle-Ottawa Scale (NOS), revealing that seven studies had a low risk of bias, while six demonstrated a moderate risk. Findings indicate that severe hypoglycemia, particularly when early-onset or recurrent, is consistently associated with adverse outcomes, including motor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
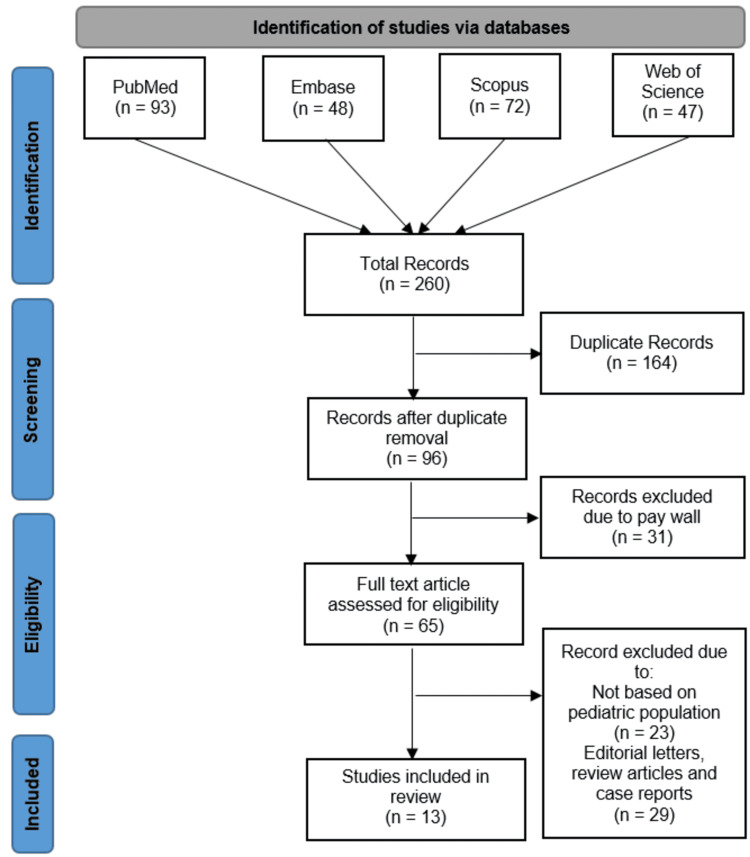 Figure 1
Figure 1| Author (year) | Country | Study design | Sample size | Gestational age (term/preterm) | Definition of Hypoglycemia | Timing of hypoglycemia assessment | Neurodevelopmental outcomes assessed | Age at follow-up | Key findings |
| Brand et al., [ | Netherlands | Prospective observational | 75 | Term (LGA infants) | Plasma glucose <2.2 mmol/L at 1 hour, or <2.5 mmol/L thereafter | At 1, 3, and 5 hours after birth, continued if low | Denver developmental scale, non-verbal IQ test, child behavior checklist | 4 years | No significant differences in developmental or behavior scores; lower reasoning IQ in one subscale but not consistent across definitions; no effect of treatment |
| Kerstjens et al., [ | Netherlands | Community-based stratified cohort | 832 | Moderately preterm (32–35⁶⁄₇ weeks) | NR | Neonatal period (inferred from "neonatal morbidities") | Developmental delay via ages and stages questionnaire | 43-49 months (approx. 3.5–4 years) | Hypoglycemia significantly associated with developmental delay (OR: 2.19; 95% CI: 1.08–4.46) |
| Kaiser et al., [ | USA | Retrospective population-based cohort study | 1395 newborn-student pairs (from 1943 eligible) | 23–42 weeks’ gestation (includes both term and preterm) | Glucose level <35 mg/dL (primary), <40 mg/dL and <45 mg/dL (secondary) | Within the first 3 hours of life (early transient hypoglycemia) | Proficiency in 4th-grade literacy and mathematics achievement tests | 10 years | Early transient hypoglycemia was associated with lower proficiency in literacy and math at 10 years of age |
| Goode et al., [ | USA (national, multisite) | Secondary analysis of RCT longitudinal study | 745 (with glucose data) | Preterm | Stratified into 4 glucose level groups (exact thresholds not specified) | Neonatal period (glucose levels recorded) | Cognitive, academic, behavioral assessments | 3, 8, and 18 years | No significant differences in cognitive/academic skills; fewer problem behaviors at 18 in severe hypoglycemia group but clinically not meaningful |
| McKinlay et al., [ | New Zealand | Prospective cohort Study | 528 | ≥35 weeks (mostly term/preterm late) | Blood glucose <47 mg/dL (2.6 mmol/L) | Intermittent blood glucose for up to 7 days; continuous masked interstitial glucose monitoring | Bayley scales of infant development III; executive function; visual function | 2 years | Neonatal hypoglycemia treated to maintain glucose ≥47 mg/dL was not associated with increased neurosensory impairment or processing difficulties at 2 years. |
| Mahajan et al., [ | India | Prospective cohort study | 72 hypoglycemic neonates (27 symptomatic, 45 asymptomatic) + 70 euglycemic controls | >32 weeks of gestation (both term and preterm included) | Plasma glucose < 50 mg/dL; also analyzed < 40 mg/dL threshold | First week of life (enrollment); neurodevelopment assessed at 6 and 12 months corrected age | Motor and mental development quotients; cerebral palsy diagnosis | 6 months and 12 months corrected age | Hypoglycemia (both symptomatic and asymptomatic) is associated with significantly lower motor and mental scores compared to euglycemia. Worse outcomes with symptomatic hypoglycemia and glucose <40 mg/dL. 8% developed cerebral palsy in the hypoglycemic group. |
| McKinlay et al., [ | New Zealand | Prospective cohort | 614 neonates | Moderate to late preterm and term | Blood glucose <47 mg/dL; severe episode <36 mg/dL; recurrent ≥3 episodes; interstitial glucose <47 mg/dL for ≥10 minutes | Up to 7 days after birth (blood and interstitial glucose measured) | Cognitive function, executive function, visual function, and motor function | 4.5 years | No increased risk of overall neurosensory impairment; increased risk of low executive function and visual motor function, especially with severe, recurrent, or clinically undetected hypoglycemia |
| Wickström et al., [ | Sweden | Population-based cohort | 101,060 | Term (otherwise healthy infants) | Moderate neonatal hypoglycemia (exact glucose threshold not specified) | Early neonatal (<6 hours) and general neonatal period | Any neurological/neurodevelopmental outcome, developmental delay, motor delay, cognitive delay | 2-6 years | Moderate neonatal hypoglycemia associated with increased risk of neurological and neurodevelopmental impairments; ORs up to ~3-fold higher for cognitive delay, especially with early hypoglycemia (<6h) |
| Qiao et al., [ | China | Prospective cohort | 195 infants enrolled; 157 followed with hypoglycemia; 144 control group | NR | Blood glucose level < 2.6 mM | Within 0.5 h after birth, subdivided into: <2 h, 2–24 h, >24 h after birth | Neurodevelopment evaluated by Gesell scoring method (focus on adaptability) | NR | Prolonged/repeated hypoglycemia (A2 and A3 groups) caused poor adaptability. Maternal insulin use and weight gain are associated with severe or persistent neonatal hypoglycemia. |
| Rasmussen et al., [ | Denmark | Cohort follow-up with sibling controls | 71 neonates with hypoglycemia, 32 healthy siblings | ≥35 weeks (exclusion of <35 weeks) | Blood glucose <1.7 mmol/L (<30 mg/dL), treated to >2.5 mmol/L (>45 mg/dL) | Neonatal period (transient hypoglycemia recorded at the neonatal stage) | Cognitive function (Wechsler IV), motor function (Movement ABC-2), behavior (Child behavior checklist) | Mean 7.75 years (hypoglycemia), 9.17 years (siblings) | Lower fine motor scores in the hypoglycemia group within the normal range, especially boys; no difference in cognitive or behavioral outcomes |
| Edwards et al., [ | New Zealand | Exploratory cohort analysis of RCT | 1197 | Late preterm and term | Blood glucose < 47 mg/dL; severe < 36 mg/dL; recurrent = ≥3 episodes | Neonatal period, screening and treatment to maintain glucose ≥47 mg/dL | Neurosensory impairment (blindness, deafness, cerebral palsy, developmental delay, executive function); Bayley III cognitive and motor scores | Corrected age 24 months | Hypoglycemia associated with increased risk of neurosensory impairment (aRR 1.28), especially severe episodes (aRR 1.68); no increased risk for recurrent episodes; lower Bayley-III cognitive and motor scores observed |
| Kennedy et al., [ | New Zealand | Prospective cohort | 101 | ≥36 weeks’ gestation (mostly term) | ≥1 hypoglycemic episode with blood glucose <2.6 mmol/L or ≥10 min interstitial glucose <2.6 mmol/L | Neonatal period (exact timing not specified, but neonatal hypoglycemia episodes) | Executive function, academic achievement, emotional-behavioural regulation, visual memory, prosocial behaviour | 9-10 years | Smaller caudate volume linked with greater emotional and behavioural difficulties and poorer prosocial behaviour. Neonatal hypoglycemia associated with smaller caudate volume but not with clinically relevant neurodevelopmental deficits. |
| Shah et al., [ | New Zealand (Waikato hospital) | Prospective cohort study | 614 recruited (480 assessed at follow-up) | Moderate to late preterm and term infants | Blood glucose <47 mg/dL (2.6 mmol/L) or interstitial sensor glucose <47 mg/dL for ≥10 minutes (episodes >20 min apart) | Up to 7 days after birth, continuous glucose monitoring with masked sensors | Primary: Educational achievement (reading comprehension, mathematics); Secondary: executive function, visual-motor function, psychosocial adaptation, general health | Mean 9.4 years | No significant difference in low educational achievement between hypoglycemia-exposed and unexposed groups; hypoglycemia-exposed children less likely rated below curriculum in reading by teachers. |
| Author (year) | Hypoglycemia severity | Timing of onset | Glucose threshold used | Outcome domain affected | Direction of effect |
| Brand et al., [ | Transient mild to severe | Within the first 1, 3, and 5 hours of birth | <2.2 mmol/L at 1 hour, <2.5 mmol/L afterwards | Reasoning IQ (subscale), Psychomotor development, behavior | No overall negative effect; slight decrease in reasoning IQ only |
| Kerstjens et al., [ | NR | Neonatal period | NR | Developmental delay at preschool age | Increased risk (OR: 2.19; 95% CI: 1.08–4.46) |
| Kaiser et al., [ | Transient (single low glucose) | Within the first 3 hours of life | <35, <40, and <45 mg/dL | Literacy and mathematics achievement | Decreased proficiency |
| Goode et al., [ | More severe neonatal hypoglycemia (vs. mild/no hypoglycemia) | Neonatal period (preterm infants) | NR | Cognitive, academic, behavioral (age 3 to 18 years) | No significant difference in cognitive/academic, fewer behavioral problems at 18 in severe group (not clinically meaningful) |
| McKinlay et al., [ | Neonatal hypoglycemia (blood glucose <47 mg/dL) | Neonatal period (up to 7 days) | 47 mg per deciliter (2.6 mmol/L) | Neurosensory impairment, executive and visual function (processing difficulty) | No increased risk (risk ratio ~1, no adverse effect) |
| Mahajan et al., [ | Symptomatic and asymptomatic | Neonatal period (first week of life) | <50 mg/dL (hypoglycemia), with special focus < 40 mg/dL | Neurodevelopmental outcomes: motor development quotient, mental development quotient, cerebral palsy incidence | Adverse effect (lower motor and mental development quotients; increased cerebral palsy in hypoglycemic infants) |
| McKinlay et al., [ | Any hypoglycemia, severe (<36 mg/dL), recurrent (≥3 episodes), clinically undetected (interstitial episodes) | Neonatal period (birth to 7 days) | <47 mg/dL (blood), <36 mg/dL (severe), <47 mg/dL (interstitial for ≥10 min) | Executive function, Visual motor function, Neurosensory impairment (not increased) | Increased risk for executive and visual motor function impairment; no increased risk for combined neurosensory impairment |
| Wickström et al., [ | Moderate neonatal hypoglycemia | Early neonatal (<6 hours) and overall neonatal period | NR | Any neurological or neurodevelopmental outcome; developmental delay (any, motor, cognitive) | Increased risk (OR >1 for all outcomes) |
| Qiao et al., [ | Neonatal hypoglycemia overall (subgroups A1, A2, A3 with increasing severity) | <2h (A1), 2-24h (A2), >24h (A3) after birth | <2.6 mM | Neurodevelopment (adaptability) | Negative effect: poorer adaptability in A2 and A3 compared to controls |
| Rasmussen et al., [ | Transient neonatal hypoglycemia | Neonatal period | <1.7 mmol/L (<30 mg/dL) for diagnosis; treated with >2.5 mmol/L (>45 mg/dL) | Fine motor function (Movement ABC-2 test), Cognitive function (Wechsler IV), behavior (child behavior checklist) | Lower fine motor scores within normal range, no significant changes in cognitive function or behavior; effect stronger in boys |
| Edwards et al., [ | Any hypoglycemia, severe (<36 mg/dL), recurrent (≥3 episodes) | Neonatal period (first hour after birth) | <47 mg/dL (any), <36 mg/dL (severe), ≥3 episodes <47 mg/dL (recurrent) | Neurosensory impairment, cognitive and motor development | Increased risk for neurosensory impairment (especially severe), lower cognitive and motor scores; no significant risk increase for recurrent episodes |
| Kennedy et al., [ | At least one hypoglycaemic episode (blood glucose <2.6 mmol/L or ≥10 min interstitial glucose <2.6 mmol/L) | Neonatal period (birth, within first days) | Blood glucose <2.6 mmol/L or interstitial glucose < 2.6 mmol/L for at least 10 minutes | Emotional-behavioural difficulties, prosocial behaviour, visual memory, executive function, academic achievement | Smaller caudate volume associated with greater emotional-behavioural difficulties and poorer prosocial behaviour; caudate volume positively associated with visual memory only in non-hypoglycaemic children; no relation to executive function or academic achievement |
| Shah et al., [ | Moderate to mild hypoglycemia (blood glucose <47 mg/dL) | Neonatal period (first 7 days after birth) | Blood glucose <47 mg/dL (2.6 mmol/L) | Educational performance (reading comprehension, mathematics), executive function, visual-motor function, psychosocial adaptation, general health | No significant association with lower educational achievement; slight decreased risk for poor reading ratings by teachers |
| Author (Year) | Selection (max 4) | Comparability (max 2) | Outcome (max 3) | Total score (max 9) | Risk of bias |
| Brand et al., [ | 3 | 1 | 2 | 6 | Moderate |
| Kerstjens et al., [ | 4 | 2 | 3 | 9 | Low |
| Kaiser et al., [ | 3 | 1 | 2 | 6 | Moderate |
| Goode et al., [ | 4 | 2 | 3 | 9 | Low |
| McKinlay et al., [ | 4 | 2 | 3 | 9 | Low |
| Mahajan et al., [ | 3 | 1 | 2 | 6 | Moderate |
| McKinlay et al., [ | 4 | 2 | 3 | 9 | Low |
| Wickström et al., [ | 4 | 2 | 3 | 9 | Low |
| Qiao et al., [ | 3 | 1 | 2 | 6 | Moderate |
| Rasmussen et al., [ | 4 | 2 | 3 | 9 | Low |
| Edwards et al., [ | 4 | 2 | 3 | 9 | Low |
| Kennedy et al., [ | 4 | 2 | 2 | 8 | Low |
| Shah et al., [ | 4 | 2 | 3 | 9 | Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHyperglycemia and glycemic control in critically ill and hospitalized patients · Neonatal and fetal brain pathology · Neonatal Respiratory Health Research
Introduction and background
Neonatal hypoglycemia is among the most common metabolic disturbances encountered in the immediate postnatal period, affecting both term and preterm infants [1]. Characterised by abnormally low blood glucose levels, its early identification and management remain critical due to the heightened metabolic demands of the developing neonatal brain [2]. While transient hypoglycemia is often considered benign when promptly corrected, growing evidence suggests that even short episodes of low glucose may have lasting implications for neurodevelopment [3].
Despite standardised thresholds and treatment protocols, substantial heterogeneity exists in clinical definitions, diagnostic timing, and intervention thresholds across institutions [4]. This inconsistency has complicated the establishment of clear associations between neonatal hypoglycemia and long-term neurodevelopmental outcomes such as cognitive function, executive processing, motor skills, and behavioral regulation [5]. Several observational and cohort studies have reported associations with adverse outcomes, including developmental delay, learning disabilities, and decreased school performance, whereas others suggest no significant long-term sequelae when hypoglycemia is effectively managed [6,7].
The primary objectives of this review are threefold: (1) to evaluate the association between neonatal hypoglycemia and long-term neurodevelopmental outcomes, (2) to assess whether this association varies by hypoglycemia severity, timing, or treatment, and (3) to identify critical gaps in the current evidence base to guide future research. Our findings have important implications for clinical practice, particularly in determining which infants may benefit from closer monitoring, earlier intervention, and targeted developmental support.
Review
Methodology
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [8].
Eligibility Criteria
The review included observational cohort studies (prospective and retrospective) and randomised controlled trials (RCTs) that examined the relationship between neonatal hypoglycemia and neurodevelopmental outcomes in children. Eligible studies had to meet the following criteria: (1) a defined population of neonates (term or preterm) with documented hypoglycemia, (2) a comparison group (euglycemic infants or different hypoglycemia thresholds), (3) assessment of neurodevelopmental outcomes (cognitive, motor, behavioral, or academic) at any age beyond infancy, and (4) publication in English in a peer-reviewed journal. Case reports, reviews, and studies without a control group were excluded.
Search Strategy
A comprehensive literature search was conducted in PubMed, Embase, Scopus, and Web of Science. The search strategy combined Medical Subject Headings (MeSH) and keywords related to neonatal hypoglycemia ("neonatal hypoglycemia," "transient hypoglycemia," "low blood glucose") and neurodevelopmental outcomes ("neurodevelopment," "cognitive impairment," "motor delay," "executive function"). The full search syntax was adapted for each database and is provided in the appendices section of this article (Appendix A).
Study Selection
After removing duplicates, two independent reviewers screened titles and abstracts for relevance. Full texts of potentially eligible studies were then assessed against the inclusion criteria. Conflicts were resolved through discussion or consultation with a third reviewer. The study selection process was documented in a PRISMA flow diagram, detailing the number of records identified, excluded, and included at each stage.
Data Extraction
A standardised data extraction form was developed and pilot-tested on three randomly selected studies to ensure consistency and comprehensiveness in data collection. The form captured key variables including study characteristics (author, year, country, study design, and sample size), population details, exposure assessment, and neurodevelopmental outcomes. To minimise bias and enhance reliability, two reviewers independently extracted data using this form, with any discrepancies between reviewers being resolved through discussion and consensus. This rigorous approach ensured the accurate and systematic collection of relevant data from all included studies while maintaining methodological consistency throughout the review process.
Risk of Bias Assessment
The methodological quality of included studies was assessed using the Newcastle-Ottawa Scale (NOS) [9] for cohort studies, a validated tool that evaluates three domains: selection (4 stars), comparability (2 stars), and outcome (3 stars), with a maximum score of 9 indicating the lowest risk of bias. Studies with a score of ≥7 were classified as high quality, those scoring between 5 and 6 as moderate quality, and those with a score of ≤4 were considered to have a high risk of bias.
Data Synthesis and Justification for No Meta-Analysis
Given the substantial clinical and methodological heterogeneity across studies, including varying definitions of hypoglycemia (e.g., different glucose thresholds, timing of exposure), diverse neurodevelopmental assessment tools, and differences in follow-up duration, meta-analysis was deemed inappropriate. Combining such heterogeneous data statistically would risk producing misleading pooled estimates. Instead, a narrative synthesis was conducted, categorising findings based on hypoglycemia severity, timing, and neurodevelopmental domains affected. This approach allowed for a nuanced interpretation of the evidence while acknowledging variations in study design and population characteristics.
Results
Study Selection
The initial database search across Scopus (n=72), Embase (n=48), Web of Science (n=47), and PubMed (n=93) yielded 260 records, of which 164 duplicates were removed. After screening the remaining 96 records, 31 were excluded due to paywall restrictions, leaving 65 full-text articles assessed for eligibility. Of these, 23 were excluded for not focusing on pediatric populations, and 29 were removed as they comprised editorial letters, reviews, or case reports. Ultimately, 13 studies met the inclusion criteria and were incorporated into the systematic review (Figure 1).
PRISMA 2020 flow diagram of literature search and screening process
Study Characteristics** **
We included 13 studies examining the association between neonatal hypoglycemia and long-term neurodevelopmental outcomes in children [10-22]. The studies varied in design, including prospective cohort studies [10,14-16,18-22], retrospective cohort studies [12], community-based stratified cohorts [11], and secondary analyses of randomised controlled trials [13]. Sample sizes ranged from 72 neonates [15] to 101,060 infants [17], with follow-up periods extending from 6 months to 10 years. The studies encompassed diverse populations, including term, preterm, and large-for-gestational-age (LGA) infants, and employed varying definitions of hypoglycemia, with glucose thresholds ranging from <1.7 mmol/L (<30 mg/dL) to <47 mg/dL (<2.6 mmol/L) (Table 1).
Neurodevelopmental Outcomes by Hypoglycemia Severity
The severity of neonatal hypoglycemia appeared to influence neurodevelopmental outcomes. Severe hypoglycemia (glucose <36 mg/dL or <2.0 mmol/L) was associated with adverse effects, including lower motor and mental development quotients at 6 and 12 months [15], increased risk of neurosensory impairment [20], and poorer executive and visual-motor function at 4.5 years [16]. Symptomatic hypoglycemia was linked to worse outcomes compared to asymptomatic cases, with an 8% incidence of cerebral palsy in the hypoglycemic group [15]. In contrast, milder hypoglycemia (glucose<47 mg/dL) was not consistently associated with neurodevelopmental deficits. For instance, McKinlay et al. [14] found no increased risk of neurosensory impairment at 2 years, and Shah et al. [22] reported no significant differences in educational achievement at mid-childhood. However, Wickström et al. observed a 3-fold higher risk of cognitive delay even with moderate hypoglycemia, particularly when occurring within the first 6 hours of life [17].
Timing of Hypoglycemia** **
The timing of hypoglycemia onset emerged as a critical factor. Early hypoglycemia (<6 hours postpartum) was associated with a higher risk of neurodevelopmental impairments, including cognitive and motor delays [17]. Similarly, Kaiser et al. [12] reported that transient hypoglycemia within the first 3 hours of life was linked to lower proficiency in literacy and mathematics at 10 years. Prolonged or recurrent hypoglycemia episodes also showed negative effects. Qiao et al. [18] found that hypoglycemia lasting >24 hours (A3 subgroup) resulted in poorer adaptability scores, while McKinlay et al. [16] noted that recurrent episodes (≥3) were associated with executive function deficits.
Specific Neurodevelopmental Domains Affected
The impact of neonatal hypoglycemia varied across neurodevelopmental domains. Cognitive outcomes were mixed; some studies reported no significant differences [10,13,19], while others found lower cognitive scores [20] or delays [17]. Motor function was more consistently affected, with lower fine motor scores [19] and increased cerebral palsy risk [15]. Executive function and visual-motor skills were particularly vulnerable, with impairments observed at 4.5 years [16] and smaller caudate volumes linked to emotional-behavioural difficulties at 9-10 years [21]. Behavioral outcomes were less frequently studied, though Goode et al. [13] noted fewer problem behaviors at 18 years in severe hypoglycemia cases, albeit without clinical significance.
Heterogeneity in Findings** **
Notably, several studies reported no significant associations between neonatal hypoglycemia and long-term outcomes. For example, Brand et al. [10] found no overall negative effects in term LGA infants, and Shah et al. [22] observed no differences in academic performance. This heterogeneity may stem from variations in hypoglycemia definitions, treatment protocols, and follow-up durations. For instance, Edwards et al. [20] highlighted that aggressive treatment to maintain glucose ≥47 mg/dL mitigated some risks, underscoring the role of clinical management in shaping outcomes (Table 2).
Risk of Bias Findings
The risk of bias assessment revealed that seven studies demonstrated particularly strong methodology with scores of 9/9, including Kerstjens et al. [11], Goode et al. [13], McKinlay et al. [14, 16], Wickström et al. [17], Rasmussen et al. [19], Edwards et al. [20], and Shah et al. [22]. These studies featured well-defined cohorts, appropriate control for confounding variables, and validated outcome measures. Six studies received moderate scores of 6-8/9 due to limitations such as incomplete adjustment for confounders or smaller sample sizes, including Brand et al. [10], Kaiser et al. [12], Mahajan et al. [15], Qiao et al. [18], and Kennedy et al. [21]. Notably, the study by Mahajan et al. [15] had a relatively small sample size (n=72), while Kaiser et al. [12] used a retrospective design that may have introduced selection bias. Despite these variations, the overall quality of evidence was robust, with most studies demonstrating low risk of bias, supporting the reliability of the systematic review's conclusions. The observed heterogeneity in hypoglycemia definitions across studies, with thresholds ranging from <1.7 mmol/L to <47 mg/dL, suggests the need for standardised criteria in future research (Table 3).
Discussion
Our analysis of 13 studies reveals that while severe, early-onset, or prolonged hypoglycemia appears consistently associated with adverse neurodevelopmental sequelae, the evidence for milder or promptly treated hypoglycemia remains inconclusive. This dichotomy suggests that not all neonatal hypoglycemia carries equal risk, and that timing, severity, and clinical management may be critical moderators of outcomes. The most robust associations emerged for severe hypoglycemia (glucose <36 mg/dL or <2.0 mmol/L), which was linked to motor dysfunction, cognitive deficits, and in some cases, cerebral palsy [15,20]. These findings align with earlier work by Lucas et al. [23] that first established the potential for severe neonatal hypoglycemia to cause permanent neurological damage, particularly when prolonged or recurrent.
The temporal aspects of hypoglycemia emerged as particularly salient in our review. Early hypoglycemia occurring within the first 6 hours of life demonstrated stronger associations with adverse outcomes compared to later-onset episodes [12,17]. This timing effect may reflect the particular vulnerability of the neonatal brain during the immediate transitional period after birth, when cerebral glucose utilisation patterns are undergoing dramatic changes [24]. The finding that hypoglycemia during this critical window predicts poorer literacy and mathematics performance at age 10 years [12] suggests that early metabolic instability may disrupt fundamental neurodevelopmental processes that later manifest as academic difficulties. This temporal sensitivity also helps explain why some studies of later-onset or briefly treated hypoglycemia failed to find significant associations [14,22].
An important nuance in our findings concerns the differential impact across neurodevelopmental domains. Motor function appears particularly vulnerable to neonatal hypoglycemia, with multiple studies reporting impaired fine motor skills [19], visual-motor integration difficulties [16], and, in severe cases, cerebral palsy [15]. This pattern mirrors neuropathological studies showing selective vulnerability of motor pathways to hypoglycemic injury [25]. Cognitive outcomes were more variable, with some studies showing clear deficits [17,20] while others found no significant differences [10,13]. This inconsistency may reflect differences in the cognitive measures used, with more sensitive, domain-specific assessments (e.g., executive function) more likely to detect subtle deficits than global IQ measures [26].
The role of clinical management in modifying outcomes emerged as a critical consideration. Studies where hypoglycemia was aggressively treated to maintain glucose ≥47 mg/dL [14,16,20] generally found better outcomes than studies with less stringent treatment protocols. This suggests that current approaches to monitoring and treating neonatal hypoglycemia may be preventing some, though not all, of the potential neurodevelopmental consequences. However, the optimal threshold for intervention remains uncertain, as even carefully managed hypoglycemia was associated with subtle executive function difficulties in some studies [16,21]. These findings extend previous work by Tin [27], suggesting that while severe hypoglycemia clearly requires treatment, the risks of milder hypoglycemia may depend on additional factors such as duration and underlying neonatal vulnerabilities.
Population differences also appear important in interpreting these findings. The studies in our review included diverse populations from healthy term infants [10] to high-risk preterm neonates [13], and the impact of hypoglycemia varied accordingly. Preterm infants, who already face multiple neurodevelopmental risks, showed particular vulnerability to additional hypoglycemic insults [11,13]. This aligns with the concept of "double jeopardy" in neonatal neurology, where multiple risk factors interact to amplify neurodevelopmental risk [28]. Conversely, in otherwise healthy term infants, the neurodevelopmental impact of hypoglycemia appeared more modest [10,22], suggesting greater resilience or compensatory capacity in this population.
The neurobiological mechanisms underlying these associations warrant consideration. The finding that neonatal hypoglycemia is associated with reduced caudate volume and related emotional-behavioral difficulties at school age provides important clues about potential neural substrates [21]. The caudate nucleus, part of the basal ganglia, is rich in glucose transporters and particularly metabolically active during early development [29]. Its vulnerability to hypoglycemic injury may help explain some of the executive function and behavioral regulation difficulties observed in follow-up studies. Similarly, the visual-motor integration problems reported by McKinlay et al. may reflect hypoglycemia's impact on posterior cortical regions known to be sensitive to metabolic stress [16].
Our review highlights several important gaps in the current evidence base. First, there remains striking heterogeneity in how neonatal hypoglycemia is defined and measured across studies, ranging from single glucose measurements to continuous monitoring protocols. This variability makes comparisons across studies challenging and underscores the need for consensus definitions, as called for by the Pediatric Endocrine Society [30]. Second, few studies have examined potential protective factors that might mitigate hypoglycemia's effects, such as breastfeeding patterns or early developmental enrichment. Third, most studies have focused on early and middle childhood outcomes, with limited data on adolescent or adult functioning. This is particularly important given that some neurodevelopmental effects may not become apparent until higher cognitive demands emerge later in development.
The clinical implications of these findings are significant but nuanced. While our review supports vigilance for severe or prolonged neonatal hypoglycemia, it also suggests that the neurodevelopmental risks of milder, transient hypoglycemia may be overstated in some clinical contexts. This aligns with recent shifts toward more targeted approaches to neonatal glucose management [31]. However, the identification of specific high-risk scenarios, particularly early-onset, severe, or recurrent hypoglycemia, should inform clinical monitoring protocols and early intervention strategies. The finding that hypoglycemia's effects may be domain-specific (affecting motor and executive functions more than global cognition) suggests that follow-up assessments should include targeted evaluation of these vulnerable domains.
Limitations
Several limitations of this review must be acknowledged. First, the included studies varied considerably in their methodologies, populations, and definitions of hypoglycemia, limiting direct comparability. Second, despite our comprehensive search, we cannot exclude the possibility of publication bias favoring studies with positive findings. Third, most studies were observational in design, precluding definitive causal conclusions about the relationship between hypoglycemia and outcomes. Fourth, the review was limited to English-language publications, potentially omitting relevant studies published in other languages. Finally, the long-term significance of some of the more subtle neurodevelopmental differences reported remains uncertain, particularly in the absence of adult outcome data.
Conclusions
Neonatal hypoglycemia, particularly when severe, early-onset, or prolonged, is associated with adverse neurodevelopmental outcomes across multiple domains. However, the risks appear moderated by factors including clinical management, population characteristics, and hypoglycemia severity and timing. These findings support current clinical guidelines emphasising prompt identification and treatment of significant neonatal hypoglycemia while suggesting that universal screening and aggressive management of mild, transient hypoglycemia may not be warranted. Future research should focus on establishing consensus definitions, identifying biomarkers of brain injury risk, and developing targeted intervention strategies for infants at the highest neurodevelopmental risk. Clinicians should remain vigilant for hypoglycemia in high-risk neonates while adopting a balanced approach that considers both the potential risks of hypoglycemia and the costs of over-treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Transitional neonatal hypoglycemia and adverse neurodevelopment in midchildhood JAMA Netw Open Roeper M Hoermann H Körner LM Sobottka M Mayatepek E Kummer S Meissner T 07202410.1001/jamanetworkopen.2024.3683 PMC 1096641338530314 · doi ↗ · pubmed ↗
- 2Neonatal hypoglycemia and neurodevelopmental outcomes: yesterday, today, tomorrow Eur J Pediatr De Rose DU Perri A Maggio L Salvatori G Dotta A Vento G Gallini F 1113111918320243818063510.1007/s 00431-023-05405-2 · doi ↗ · pubmed ↗
- 3Hypoglycemia in the preterm neonate: etiopathogenesis, diagnosis, management and long-term outcomes Transl Pediatr Sharma A Davis A Shekhawat PS 335348620172918481410.21037/tp.2017.10.06PMC 5682372 · doi ↗ · pubmed ↗
- 4Neonatal hypoglycemia and neurodevelopmental outcomes-an updated systematic review and meta-analysis Life (Basel) Diggikar S Trif P Mudura D 14202410.3390/life 14121618 PMC 1167768739768326 · doi ↗ · pubmed ↗
- 5Neonatal glycaemia and neurodevelopmental outcomes: a systematic review and meta-analysis Neonatology Shah R Harding J Brown J Mc Kinlay C 11612611520193040881110.1159/000492859 · doi ↗ · pubmed ↗
- 6Neonatal dysglycemia: a review of dysglycemia in relation to brain health and neurodevelopmental outcomes Pediatr Res LagacéM Tam EW 142914379620243897296110.1038/s 41390-024-03411-0 · doi ↗ · pubmed ↗
- 7Exploring the long-term impacts of neonatal hypoglycemia to determine a safe threshold for glucose concentrations Eur J Pediatr Garg M Devaskar SU 26318420254011922310.1007/s 00431-025-06082-z PMC 11928350 · doi ↗ · pubmed ↗
- 8The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ Page MJ Mc Kenzie JE Bossuyt PM 0372202110.1186/s 13643-021-01626-4PMC 800853933781348 · doi ↗ · pubmed ↗