Synchronous Bladder Metastasis From Chromophobe Renal Cell Carcinoma: A Report of a Rare Case
Jose L Romero Uribe, Victor Cornejo Davila, Jose Cruz Ruiz

TL;DR
A rare case of kidney cancer spreading to the bladder in a young woman is reported, emphasizing the need for aggressive treatment.
Contribution
This paper presents a rare case of synchronous bladder metastasis from chromophobe renal cell carcinoma.
Findings
A 29-year-old female presented with a chromophobe RCC tumor that had metastasized to the bladder.
Histopathological analysis confirmed the chromophobe RCC variant in both the kidney and bladder specimens.
Aggressive surgical intervention achieved complete resection of the tumors.
Abstract
Renal cell carcinoma (RCC) is the most frequent form of kidney cancer and represents a small percentage of all adult cancers. Metastasis of RCC to the bladder is exceptionally uncommon, with only a limited number of cases documented, the majority being of the clear cell subtype. Instances involving the chromophobe variant are particularly rare. We report the case of a 29-year-old female presenting with anemia, gross hematuria, and left flank pain. Abdominal computed tomography (CT) revealed a left renal mass with features suggestive of a perinephric abscess, along with a bladder lesion. Cystoscopy with transurethral resection of the bladder tumor (TURBT) and percutaneous drainage of the abscess were performed, followed by left radical nephrectomy. Histopathological examination of both renal and bladder specimens confirmed the eosinophilic variant of chromophobe RCC (chRCC). A partial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
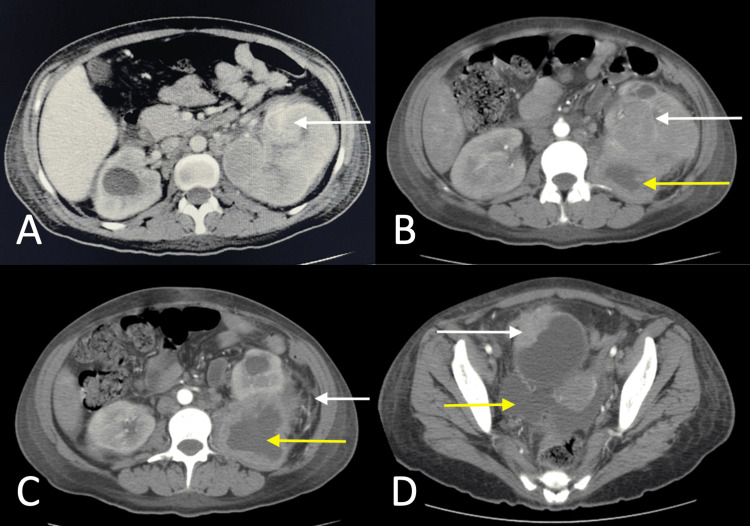 Figure 1
Figure 1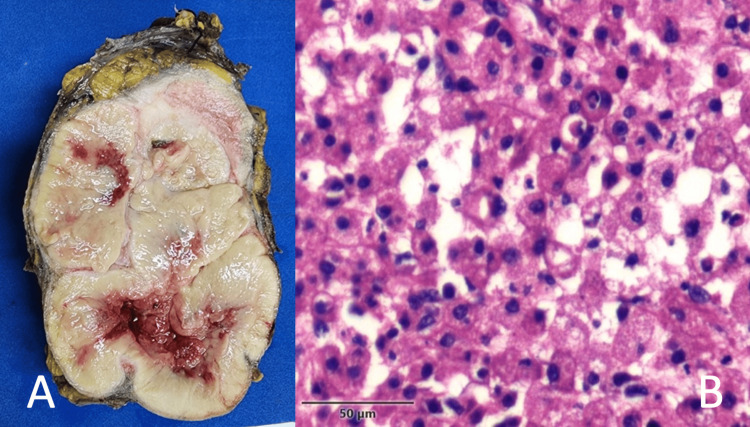 Figure 2
Figure 2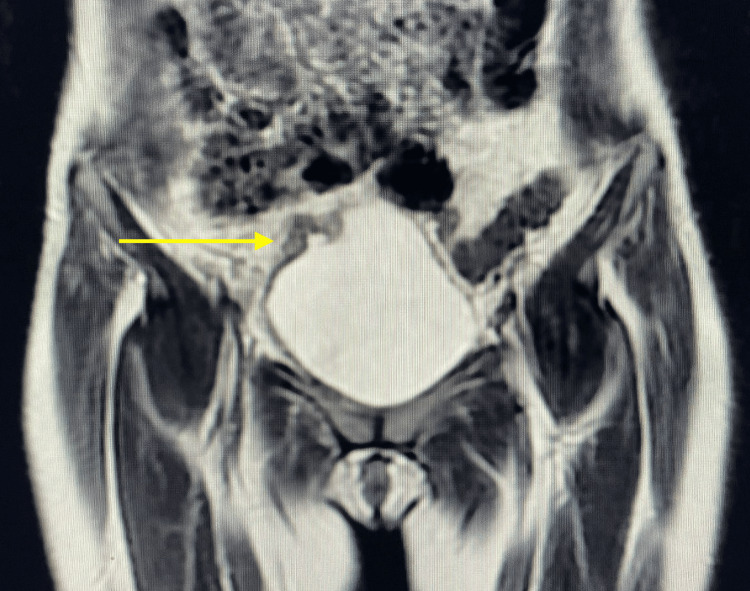 Figure 3
Figure 3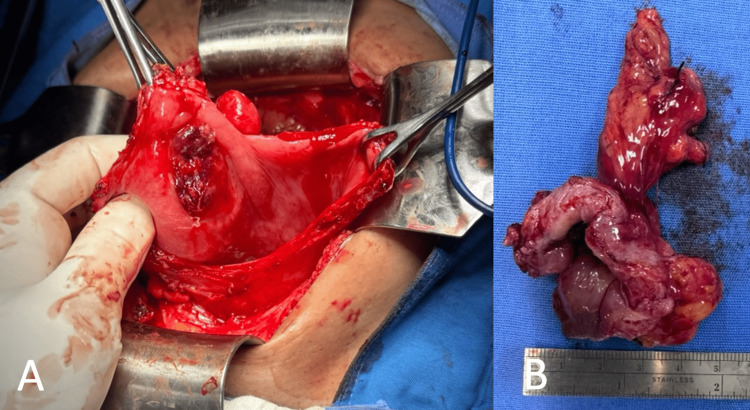 Figure 4
Figure 4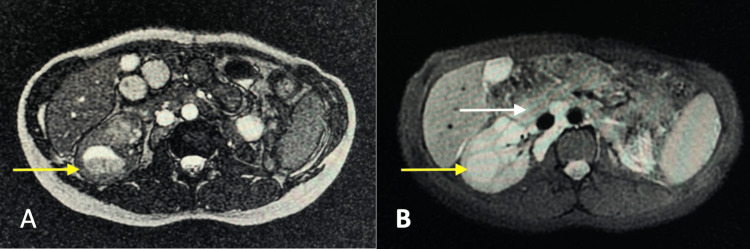 Figure 5
Figure 5| Test | Parameter | Measured value | Units | Reference range |
| Blood work | Hemoglobin | 5.1 | mg/dL | 13.0-18.0 |
| RBC | 15 | x106/uL | 4.70-6.10 | |
| WBC | 18.6 | x103/uL | 4.0-11.03 | |
| Platelets | 395 | x103/uL | 140.0-450.0 | |
| Glucose | 92 | mg/dL | 70-100 (fasting) | |
| Creatinine | 1.9 | mg/dL | 0.60-1.30 | |
| Blood urea nitrogen | 40.0 | mg/dL | 8.4-25.7 | |
| Prothrombin time (PT) | 15 | sec | 9.4-12.5 | |
| Activated partial thromboplastin time (APTT) | 28 | sec | 28.1-39.7 | |
| International normalised ratio (INR) | 1.3 | INR | 0.8-1.2 | |
| Urinalysis | Appearance | Red | - | Clear, pale, yellow, amber |
| Protein | Negative | - | Negative | |
| Blood | >100 RBCs | - | 0-3 | |
| Leukocytes | 20-30 WBCs | - | 0-2 | |
| Nitrite | Negative | - | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary and Genital Oncology Studies · Bladder and Urothelial Cancer Treatments · Urological Disorders and Treatments
Introduction
Renal cell carcinoma (RCC) is a heterogeneous group of malignancies arising from the renal epithelium and accounts for approximately 2-3% of all adult malignancies. Among its histologic subtypes, the chromophobe variant (chRCC) represents 5-7% of RCC cases and typically demonstrates a more indolent course than the most common clear cell RCC [1,2]. Despite its generally favorable prognosis, chRCC can occasionally metastasize. The eosinophilic variant of chRCC is characterized by distinct histological features, including abundant granular eosinophilic cytoplasm, prominent cell borders, and perinuclear clearing or halos. While it shares these morphological traits with oncocytoma, it can be distinguished by cytogenetic abnormalities and immunohistochemical markers such as CK7 and CD117 positivity. Despite its unique histologic appearance, it generally shares a similar prognosis with the classic variant [3].
Metastases are present in approximately one-third of patients with RCC at the time of diagnosis, and an additional one-third develop metastatic disease during follow-up [2]. The bladder is an exceptionally rare site of dissemination, comprising less than 2% of all RCC metastases [4,5]. Bladder metastases are more commonly associated with the clear cell subtype. Synchronous bladder metastases of chRCC are exceedingly rare, with only isolated cases described in the literature [6,7]. We report a rare case of synchronous bladder metastasis from chRCC in a young woman.
Case presentation
A 29-year-old female presented with a two-year history of chronic left flank pain. She also reported episodes of gross hematuria with clot formation, resulting in anemia. Constitutional symptoms included fatigue and intermittent fever. Physical examination revealed pallor and tenderness over the left costovertebral angle. Laboratory findings demonstrated severe anemia (hemoglobin: 5.1 g/dL), leukocytosis, gross hematuria, and evidence of acute kidney injury (AKI stage I) with a serum creatinine of 1.9 mg/dL (Table 1).
A contrast-enhanced CT urography revealed an atypical heterogeneous left renal mass with perinephric fat stranding and abscess, and an intravesical tumor on the right bladder wall (Figure 1). No metastases to the lungs or liver were detected on staging CT.
Contrast-enhanced axial CT images in the corticomedullary (A) and nephrographic phases (B, C, D).(A, B) Heterogeneous left renal mass primarily involving the mid and lower poles, with extension toward the upper pole (white arrows). The lesion shows heterogeneous enhancement, increasing from 15 to 50 Hounsfield Units (HU), with central non-enhancing areas suggestive of necrosis. The mass measures approximately 8.5 × 7 × 5 cm. Retroperitoneal lymphadenopathy is present. No definite evidence of renal vein invasion is seen. Abscess formation is noted in the lower pole (yellow arrow).(C) Perinephric fat stranding (white arrow) and abscess formation in the lower pole of the left kidney (yellow arrow).(D) Bladder tumor involving the right lateral wall with perivesical extension (white arrow), accompanied by ascites (yellow arrow).
Initial management included transfusion of two units of packed red blood cells, resulting in a hemoglobin level of 9.5 g/dL, along with administration of broad-spectrum antibiotics. The patient underwent cystoscopy with transurethral resection of the bladder tumor (TURBT) and percutaneous drainage of the perinephric abscess. By postoperative day 6, she was asymptomatic with clinical improvement. Abscess culture grew Escherichia coli sensitive to ertapenem, and a 10-day course of antibiotics was completed. A left radical nephrectomy was subsequently performed. Histopathological analysis revealed an eosinophilic variant of chRCC extending into the perinephric tissues, consistent with pT3a disease. Three regional lymph nodes, two paraaortic and one hilar, were positive for metastatic involvement (pN1), and similar histopathological features were observed in the bladder biopsy (Figure 2).
(A) Gross specimen of the left kidney showing a well-circumscribed tan-pink mass with central hemorrhage and necrosis. (B) Histological section (H&E stain, 400×) showing polygonal tumor cells with prominent cell borders, perinuclear clearing, and pale eosinophilic cytoplasm, consistent with the eosinophilic variant of chromophobe renal cell carcinoma (RCC).
Given the absence of systemic disease and a favorable postoperative course, an MRI was performed prior to the planned partial cystectomy (Figure 3), and the intervention was deferred for two months. According to the treating urologist, the decision to delay surgical management of the bladder lesion was based on concerns that performing both the radical nephrectomy and the transurethral resection of the bladder lesion in a single operative session could significantly increase surgical morbidity. Therefore, the procedures were staged to minimize perioperative risk and ensure optimal patient safety. Nonetheless, concurrent surgeries may be feasible in appropriately selected patients.
Coronal T2-weighted MRI demonstrating a large intravesical mass arising from the right lateral bladder wall. The lesion appears hyperintense relative to muscle, with well-defined borders and mass effect on the bladder lumen, consistent with bladder metastasis (yellow arrow).
Histological examination confirmed metastatic chRCC with extension into perivesical fat but negative margins (R0 resection) (Figure 4). Final staging was pT3a pN1 M1. The patient remained asymptomatic but was lost to follow-up due to her marginalized situation, including poor economic status and a long distance from the medical center. She eventually developed abdominal pain, systemic symptoms, and renal failure. MRI revealed disease progression, demonstrating retroperitoneal lymph node conglomerates and a right renal mass, which may suggest progression of RCC metastasis (Figure 5). The patient was managed expectantly without adjuvant therapy, and no evaluation for genetic cancer syndromes was performed. The patient died nine months after the initial diagnosis.
(A) Intraoperative view during partial cystectomy showing an infiltrating sessile bladder tumor. (B) Gross specimen from the partial cystectomy.
(A) Balanced turbo field echo (BTFE) MRI sequence showing a left renal mass with heterogeneous signal intensity (yellow arrow). (B) Diffusion-weighted MRI (b-0) demonstrating the same renal mass (yellow arrow) along with enlarged retroperitoneal lymph nodes (white arrow), suggestive of disease progression from renal cell carcinoma.
Discussion
Bladder metastasis from RCC is rare, more often seen in the metachronous setting, with a median interval of 33 months after nephrectomy [8,9]. The pathophysiology of bladder involvement remains unclear. Proposed mechanisms include hematogenous dissemination, retrograde lymphatic or venous spread, and direct intraluminal tumor cell seeding. In this case, hematogenous dissemination appears to be the most plausible route, given the absence of contiguous spread, the vascular nature of RCC, and the isolated bladder lesion without evidence of regional lymphatic involvement [10,11].
Most reported cases involve the clear cell subtype. Metastases from chRCC are even less common and may present with hematuria or urinary obstruction, depending on the site involved in the bladder [12].
There is no standardized treatment protocol for bladder metastases of RCC due to their low frequency; however, the same principles for metastatic RCC treatment are applied, with aggressive surgical resection, if feasible, and systemic targeted therapies, if available. In the bladder, treatment options usually involve partial or radical cystectomy because metastases usually involve the muscle and not just the epithelium [5,6], such as this case. Complete surgical excision can improve short-term outcomes in patients with isolated metastases [4,6].
Targeted therapies, including vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF) inhibitors, as well as immune checkpoint inhibitors (ICIs), have demonstrated effectiveness in metastatic RCC, particularly in tumors with clear cell histology [2]. However, evidence supporting their efficacy in chRCC is limited due to its rarity and biological differences [13]. However, the benefit of systemic therapy in chRCC remains less clear. In selected patients with isolated metastasis and good performance status, observation after complete surgical resection might be an option [6,8], but we should keep in mind that complete resection can result in effective disease control. In this case, even though R0 resection was achieved, the disease progressed in less than a year, which probably highlighted the aggressiveness of this presentation at such a young age.
Although evidence is limited, everolimus-based treatments appear to show the most promising activity in patients with chRCC. In the ASPEN phase II trial, everolimus monotherapy in metastatic chRCC (non-clear cell) achieved a 33% objective response rate (ORR) (two out of six patients responded) [14]. Responses to ICI monotherapy or ICI-based combination therapies are variable; it has shown limited efficacy in chRCC, suggesting potential resistance to ICI, but selected patients may benefit. No statistically significant difference has been found regarding overall survival when comparing sunitinib and everolimus [13]. Evidence for chRCC is limited, but it may offer opportunities for future targeted therapies.
This case is remarkable due to the synchronous metastasis presentation of a less common variant, the bladder involvement with no other obvious sites of metastases, and the patient's young age. This case also highlights the importance of fully assessing symptoms such as flank pain in young patients, especially if it’s accompanied by systemic symptoms or hematuria; even though most etiologies will be benign in this age group, other serious underlying conditions, including malignancies, can be diagnosed as well. The case shows the need to provide better healthcare to marginalized patients as well, since it can affect the disease outcome.
Conclusions
Bladder metastasis from chRCC is extremely rare and presents significant diagnostic and therapeutic challenges. Complete surgical resection of both primary and metastatic lesions has been associated with improved outcomes, particularly in cases of isolated metastasis. This case highlights the need for awareness of atypical metastatic patterns and supports aggressive surgical intervention as a viable treatment strategy in carefully selected patients. It also contributes to the limited body of literature on this topic and underscores the importance of a thorough evaluation in patients presenting with hematuria and renal masses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Comprehensive review of chromophobe renal cell carcinoma Crit Rev Oncol Hematol Garje R Elhag D Yasin HA Acharya L Vaena D Dahmoush L 10328716020213375325010.1016/j.critrevonc.2021.103287 · doi ↗ · pubmed ↗
- 2Kidney cancer, version 3.2022, NCCN Clinical Practice Guidelines in Oncology J Natl Compr Canc Netw Motzer RJ Jonasch E Agarwal N 71902020223499107010.6004/jnccn.2022.0001 PMC 10191161 · doi ↗ · pubmed ↗
- 3Eosinophilic variant of chromophobe renal cell carcinoma Proc (Bayl Univ Med Cent) Podduturi V Yourshaw CJ 3rd Zhang H 57582820152555280010.1080/08998280.2015.11929188 PMC 4264712 · doi ↗ · pubmed ↗
- 4Metastatic renal cell carcinoma to the bladder: case report [Article in Spanish]Rev Mex Urol Corona-Montes VE Jiménez-Cisneros E Chablé-Montero F 16832023
- 5The metastasis pattern of renal cell carcinoma is influenced by histologic subtype, grade, and sarcomatoid differentiation Medicina (Kaunas) Park HK 18455920233789356310.3390/medicina 59101845 PMC 10608745 · doi ↗ · pubmed ↗
- 6Clear-cell renal cell carcinoma single urinary bladder metastasis: a case report and review of the literature J Surg Case Rep Zachos I Mitrakas L Karasavvidou F Karatzas A Tzortzis V 02022202210.1093/jscr/rjac 475PMC 958671036299912 · doi ↗ · pubmed ↗
- 7Synchronous urinary bladder metastasis of chromophobe renal cell carcinoma BMJ Case Rep Bansal D Singh P Nayak B Kaushal S 02017201710.1136/bcr-2017-220780 PMC 553514128679514 · doi ↗ · pubmed ↗
- 8Metachronous metastasis of renal cell carcinoma to the urinary bladder: a case report Ther Adv Urol De Groote R Larcher A Goossens M 29321020172934409510.1177/1756287217738986 PMC 5761917 · doi ↗ · pubmed ↗