Performance of the low-cost phenotypic thin-layer agar MDR/XDR-TB Colour Test (first generation, 1G, Color Plate Test) for identifying drug-resistant Mycobacterium tuberculosis isolates in a resource-limited setting
Binyam Mebrat, Juan I. Garcia, Yimtubezenash Woldeamanuel, Kelemework Adane, Amberlee Hicks, Melaku Tilahun, Sebsib Neway, Lelisa Oluma, Abay Atnafu, Jonathan Gelfond, Carlton A. Evans, Jordi B. Torrelles, Shu-Hua Wang, Liya Wassie

TL;DR
A low-cost test for detecting drug-resistant tuberculosis was found to be faster and as accurate as existing methods in a study from Ethiopia.
Contribution
The study evaluates the performance of a low-cost, rapid phenotypic test for drug-resistant TB in a resource-limited setting.
Findings
The Colour Test provided results significantly faster than the IPM and MGIT assays.
The Colour Test showed high accuracy compared to both IPM and MGIT for detecting drug resistance.
The Colour Test could improve accessibility and speed of TB drug-susceptibility testing in resource-constrained areas.
Abstract
The accessible, easy to use and timely, diagnosis of tuberculosis (TB) drug-susceptibility, including multi-drug resistant (MDR-) TB and extensively-drug resistant (XDR-)TB is often challenging, particularly in resource-constrained settings. We therefore evaluated the phenotypic thin-layer agar based MDR/XDR-TB Colour Test, which is also referred to as the “First Generation (1G) Color Plate Test (TB-CX)” performance for detecting resistance of Mycobacterium tuberculosis (Mtb) isolates to selected anti-TB drugs versus other tests routinely used in our setting. A cross-sectional study was conducted on Mtb clinical isolates stored at the Armauer Hansen Research Institute TB laboratory in Addis Ababa, Ethiopia. Drug-susceptibility testing was performed on 78 Mtb isolates for isoniazid, rifampicin, and moxifloxacin using the Colour Test and the Indirect Proportional Method (IPM) “in house”…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
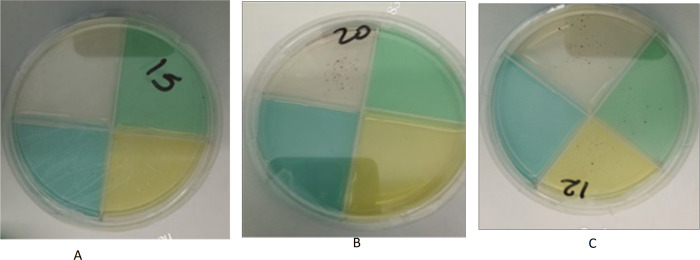 Figure 1
Figure 1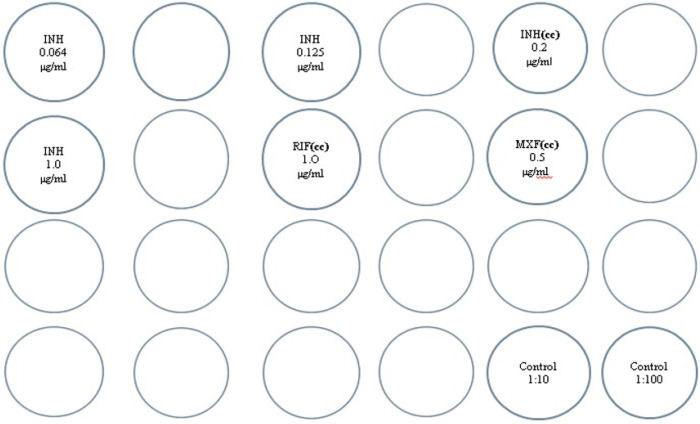 Figure 2
Figure 2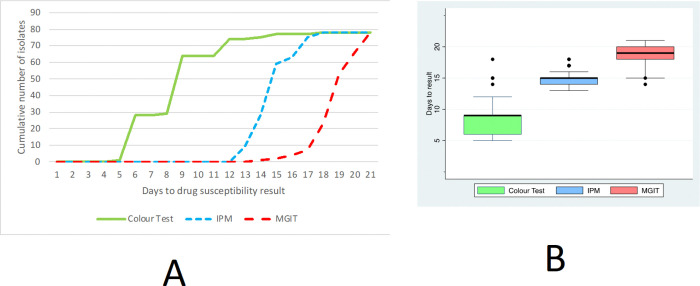 Figure 3
Figure 3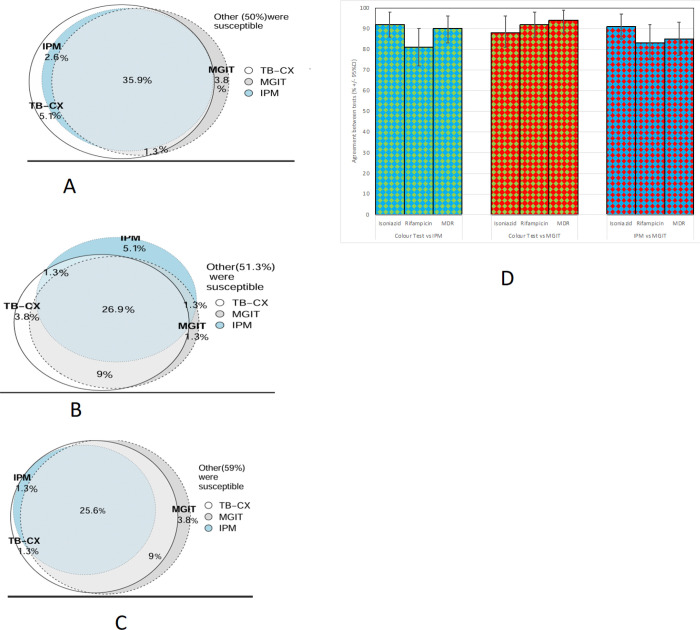 Figure 4
Figure 4- —AHRI
- —International Center for the Advancement of Research & Education (I·CARE), Texas Biomedical Research Institute (San Antonio, TX, US), The Ohio State University (Columbus, OH, USA)
- —National Institute of Allergy and Infectious Diseases of the National Institutes of Health (NIH/NIAID), NIH/NIAID the Interdisciplinary NexGen TB Research Advancement Center (IN-TRAC) at Texas Biomedi
- —Global Health Trials/UKRI/MRC/DHSC/Wellcome Trust, IFHAD: Innovation for Health and Development
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Mycobacterium research and diagnosis · Antibiotic Resistance in Bacteria
INTRODUCTION
Tuberculosis (TB) is caused by Mycobacterium tuberculosis (Mtb) complex (1). The World Health Organization (WHO) has estimated that in 2023 there were 10.8 million cases, resulting in 1.25 million deaths, including 161,000 deaths in individuals living with HIV (2). With the decline of COVID-19, TB is once again the world’s most frequent cause of death from a single infectious agent and caused almost twice as many deaths as HIV/AIDS(3).
Difficulties in TB diagnosis are important barriers to global attempts to end the TB pandemic (4). Due partly to limitations in the timely diagnosis of drug-resistant (DR)-TB, and a shortage of phenotypic and genotypic tools in resource-limited areas, multi-drug-resistant (MDR)-TB is increasing globally (5). In recent years, the development and evaluation of rapid and low-cost phenotypic culture methods have been considered to be priorities to fulfil ‘The End TB Strategy’ milestones (6). These include liquid media-based culture, microscopic observation drug susceptibility assay (MODS), the nitrate reductase assay, and the colorimetric redox-indicator assays (7–9).
Although genotypic methods of TB diagnosis are effective, rapid, and detect resistant clinical isolates (10), they are often costly and some require skilled personnel and also sophisticated equipment and maintenance (11). A low-cost, phenotypic method that has been developed is the thin layer agar (TLA) based MDR/XDR-TB Colour Test (abbreviated to “TB-CX”), which is also referred to as the “First Generation (1G) Color Plate Test (TB-CX)” (12, 13). The TB-CX is designed for use in resource-constrained settings to provide timely, relatively bio secure and accurate results to complement or replace conventional culture methods in the field, such as the Mycobacteria growth indicator tube (MGIT) DST assay, and Löwenstein-Jensen (LJ) culture DST. This has the potential to facilitate early TB treatment of patients with MDR-TB (13), either by direct testing of specimens collected from patients (most frequently sputum), or by indirect testing of Mtb isolates that have already been cultured from patient specimens.
The current study aimed to evaluate the performance of the TB-CX to detect drug resistance in Mtb by indirect testing of isolates compared to two existing DST methods: the indirect proportion method in 7H10 agar (IPM assay) and the MGIT assay.
METHODS
Study setting
A cross-sectional study was conducted on stored Mtb clinical isolates, archived at the Armauer Hansen Research Institute (AHRI) TB laboratory, in Ethiopia, from 2020 to 2022. A purposive sampling method that was focused on the quality of samples by evaluating storage condition, the absence of leakage and availability of linked clinical data was used to select 105 Mtb stored isolates from the TB laboratory repository.
Demographic and clinical data, including age, sex, and data on previous history of anti-TB treatment were collected using a standard data collection form. Ethical approval was obtained from the Research Ethics Committee of the Department of Microbiology, Immunology and Parasitology, College of Health Sciences, Addis Ababa University, and the AHRI/All Africa Leprosy and Tuberculosis Rehabilitation and Training Center (ALERT) Ethics Review Committee (Protocol number PO-07/23). All data were de-identified, and only coded samples and their linked clinical data were used in the study.
Laboratory preparation ofMtbbacterial suspensions for DST
Mtb clinical isolates were stored in cryopreservation media (i.e., 7H9 broth supplemented with a final concentration of 25% glycerol), to optimise preservation. Additionally, the quality of storage conditions was rigorously evaluated and used as a critical criterion in the selection process. Selected Mtb clinical isolates (n = 105) were sub-cultured on LJ media. Those that grew on LJ culture media (n = 78) were then considered for further analyses.
Colonies were identified and suspended in 5 drops (~ 200 μl) of sterile distilled water. The tubes were shaken by hand for 1 min and suspensions were allowed to settle for 15 min. A Mtb suspension with an optical density (assessed by eye as cloudiness) of McFarland grade 0.5 was prepared for inoculation of MGIT DST and McFarland 1 was prepared and diluted accordingly for the inoculation of the TB-CX and IPM assays.
Laboratory assessment of DST
Three laboratory assays were used for laboratory assessment of DST: the TB-CX and IPM assay for isoniazid, rifampicin and moxifloxacin DST, and MGIT DST for isoniazid and rifampicin only.
The TB-CX
This test was manufactured at Texas Biomedical Research Institute, in San Antonio, Texas and shipped to Ethiopia within 2 weeks of manufacture at room temperature. All TB-CXs were shipped together in two batches to Ethiopia and this shipping took approximately 5 days and the TB-CX was shipped as commercial airline ‘hold’ baggage in standard suitcases, so may have been subjected to freezing and or high temperatures in transit. Upon arrival, plates were stored at 2 to 8°C until ready to use (9, 12–15). Including transit time, the interval between manufacture of the TB-CX and their inoculation was up to 35 days. The TB-CX is based on a thin layer of 7H11 agar media containing oleic acid, albumin, dextrose, catalase (OADC), glycerol, and selective agents to inhibit other bacterial and fungal growth and a colorimetric indicator of microbial growth (12). The TB-CX contains four quadrants: a clear ‘control’ quadrant not containing any anti-TB drug, and the 3 other quadrants containing isoniazid, rifampicin, and moxifloxacin, following the critical concentrations (CC) recommended by the WHO for 7H11 of 0.2 μg/ml for isoniazid, 1.0 μg/ml for rifampicin, and 0.5 μg/ml for moxifloxacin. To distinguish drug-containing quadrants a food colorant was added (green food colorant for isoniazid quadrant, yellow for rifampicin’s quadrant and blue for moxifloxacin quadrant). (Fig. 1A). Mtb growth on the TB-CX was identified by visualizing red colonies with naked eye or using a 40X magnifier (13, 14). The TB-CXs were inoculated with two drops (~ 80 μl) 1:10 and 1:100 of dilutions of McFarland 1 suspensions in each quadrant for each isolate (15). Each TB-CX was inspected for red colonies until at least 11 colonies were seen in the control quadrant or until 42 days after inoculation (9, 12, 14, 15). To detect drug susceptibility a minimum of eleven red colonies needed to be observed in the control quadrant and no red colonies in the drug containing quadrant (Fig. 1B). To detect drug resistance a minimum of eleven red colonies need to be observed in the control quadrant and at least growth of one red colony in the drug containing quadrant. The TB-CX has similarities with the agar proportion method with the 1% critical threshold (15). By definition, mono-drug resistance for isoniazid, rifampicin, or moxifloxacin were defined when growth was observed in the control quadrant and concurrently with growth in the drug-containing quadrants. MDR-TB was defined when concurrent growth occurred in the control, isoniazid, and rifampicin quadrants. Pre-XDR TB was defined when concurrent growth occurred in the control, isoniazid, rifampicin, and moxifloxacin quadrants (Fig. 1C). However, resistance/susceptibility was considered uninterpretable if the number of colonies in the drug containing quadrant was less than 1% of the colony count in the detection quadrant. A DST result was reported as uninterpretable if less than 11 colonies grew in the control quadrant until 42 days of incubation, regardless of growth in the drug-containing quadrant. An isolate was considered to be negative for Mtb if there was no growth on any of the quadrants for 42 days. Both batches of TB-CX underwent quality control in Texas and Ethiopia that involved analysis using H37Rv pan susceptible strain and a strain with known drug-resistance to isoniazid, rifampicin and moxifloxacin.
The 24-well indirect proportion method (IPM)
A modified IPM assay adapted for 24-well agar plates containing 7H10 medium was used (16). Growth was evaluated according to the proportion method by comparing the 1:100 diluted controls to the drug containing wells as illustrated in Fig. 2. The following WHO CC for the IPM assay drugs were used to differentiate susceptible from resistant isolates: 0.2 μg/ml for isoniazid, 1.0 μg/ml for rifampicin, and 0.5 μg/ml for moxifloxacin (i.e., the same concentrations as were used in the TB-CX (16, 17). Plates were placed in a rack, covered with adhesive tape on the plates for safety reasons and incubated at 37°C for about 21 days. A strain was reported susceptible if there was more growth in the 1:100 diluted control than in the drug-containing well with the CC of the drug; and resistant, if there was more growth in the drug-containing well containing the CC than in the 1:100 diluted control. The test was repeated if there was equal growth (16).
MGIT DST
MGIT SIRE (streptomycin, isoniazid, rifampicin and ethambutol) kits were processed using BACTEC MGIT 960 mycobacterial detection instrument (BACTEC MGIT 960, BD Diagnostics, Franklin Lakes, NJ) according to manufacturer′s guidelines, and using isoniazid and rifampicin CC of 0.1 μg/ml and 1 μg/ml, respectively (i.e., a lower isoniazid and equal rifampicin concentration to those used in the TB-CX and IPM) (13, 14, 17). Mtb isolates were sub-cultured and incubated at 37°C in the MGIT equipment, until the device indicated a positive tube. DST was performed using one 7-ml MGIT tube as a control and another tube for each of isoniazid and rifampicin. When 1% or more of the test population grew in the presence of the CC of the drug, an isolate was defined as resistant (16).
Analysis
Time-to-culture growth for DST interpretation was calculated in days from the date of inoculation to the date of interpretable/valid results. Data were entered into Excel spread sheets, cleaned, and imported to statistical package for social sciences (SPSS, version 27) for statistical analyses. Data that had a skewed distribution such as time to test positivity were summarized by their median and inter-quartile ranges (IQR) and compared. Data that had an approximately normal distribution were summarised by their mean and standard deviation (SD) or 95% confidence intervals (95%CI). Proportions were stated as percentages with their 95%Cl. All 95%CI were calculated using the Wald formula. The diagnostic accuracy of the TB-CX was evaluated by determining its accuracy, sensitivity, specificity, and positive and negative predictive values (PPV, NPV), using the IPM assay and MGIT DST as reference assays for comparison. Accuracy was defined as the proportion of all results that were correct (i.e., the sum of true positive and true negative results divided among all results and expressed as a percentage) (18). Test agreements between the tests were analysed using κ-values. The two-sample Z-test of proportions was used to compare the proportions and their 95%CI for the different diagnostic tests. The McNemar chi^2^ test was also used to assess the statistical significance of specific paired comparisons.
RESULTS
The characteristics of the study population are shown in Table 1. 78 isolates were derived from patients who were 55% male, with a mean age of 30 years (SD = 14), and 52 (67%) arose from sputum samples of pulmonary TB patients whereas 26 (33%) were isolated from lymph node aspirates from patients with extra-pulmonary TB. The majority of the samples analysed, 62/78 (79%), were collected from newly diagnosed TB patients; of the remaining 6/78 (7.7%) had treatment failure, 5.1% (4/78) had a prior history of TB treatment with anti-TB medications, 3/78 (3.8%) were relapse and 3/78 (3.8%) had unknown TB treatment outcomes results. 29/78 (37%) were unknown where as 10% (5/49) of the Mtb isolates were collected from people living with HIV (PLWH),other.
Performance evaluation of the TB-CX vs. IPM
The TB-CX sensitivity compared to IPM to detect isoniazid, rifampicin, and moxifloxacin resistance alone or isoniazid combined with rifampicin (MDR-TB) was 97%, 82%, 100%, and 100%, respectively, and its specificity was 89%, 80%, 99%, and 86%, respectively. The TB-CX diagnostic accuracy for isoniazid, rifampicin, and moxifloxacin resistance detection, and MDR-TB detection was 92%, 81%, 97%, and 90%, respectively. Agreement between the TB-CX and IPM had a kappa value of 0.84 (Table 2).
Performance evaluation of the TB-CX vs. MGIT
The agreement between the TB-CX and MGIT DST to detect isoniazid, rifampicin, and MDR-TB were 88%, 92% and 94%, respectively (Table 3). For the detection of isoniazid, rifampicin resistance, and MDR-TB, the performance of the TB-CX compared to the reference MGIT, yielded a sensitivity of 91%, 93%, and 90%, and specificity of 87%, 92%, and 96%, respectively.
Performance evaluation of the IPM vs. MGIT
When compared to the MGIT DST, the sensitivity and specificity of IPM for detecting isoniazid resistance was 88% and 94%, respectively; and for detecting rifampicin resistance was 73% and 90%, respectively (Table 4). In addition, the sensitivity and specificity of IPM for detecting MDR-TB was 72% and 96%, respectively. The agreement between IPM and MGIT was 91%, 83% and 85%, respectively.
Time to Mtb Culture Growth Detection for DST
The turnaround time in days for the TB-CX ranged 5–18 (mean 8.6, median 9, IQR = 6–9, SD = 2.6); for IPM ranged 13–19 (mean 15, median 15, IQR = 15, SD = 0.90); and for MGIT ranged 14–21 (mean 19, median 19, IQR = 18–20, SD = 1.4) (Fig. 3A&3B). The turnaround time for the TB-CX was significantly (p < 0.001) faster than the IPM and then the MGIT test.
Comparative analysis of DST methods for isoniazid, rifampicin and MDR-TB
Among the 78 isolates tested, 50% (39/78) were classified as susceptible by all three DST methods (TB-CX, IPM, and MGIT). The TB-CX identified 5.1% (4/78) of isolates as isoniazid-resistant, despite being susceptible by both IPM and MGIT, with an overall agreement of 86% (67/78) in detecting isoniazid resistance (Fig. 4A). For rifampicin resistance, 47% (37/78) of the isolates were susceptible across all three methods, while 3.8% (3/78) were identified as rifampicin-resistant exclusively by the TB-CX method, resulting in an overall agreement of 78% (61/78) among the three methods (Figure B). Regarding MDR-TB, one isolate (1.3%, 1/78) was classified as MDR-TB solely by the TB-CX method, with an overall agreement of 85% (66/78) among the three DST methods (Fig. 4C&Figure 4D). Additionally, for moxifloxacin susceptibility, 97% of the isolates were susceptible in both the IPM and TB-CX methods, while 1.3% (1/78) were resistant only in the TB-CX method, and another 1.3% (1/78) were resistant in both the TB-CX and MGIT methods. Notably, moxifloxacin was not tested using the MGIT method.
DISCUSSION
This study evaluated the performance of the TB-CX as an alternative testing method for the detection of Mtb resistance to isoniazid, rifampicin, and moxifloxacin in clinical isolates. When compared to IPM and MGIT DST, the TB-CX showed good performance (sensitivity, specificity and diagnostic accuracy) in detecting resistance to isoniazid, rifampicin, moxifloxacin and MDR-TB. The TB-CX agreed with IPM and MGIT with similar frequency to the IPM and MGIT agreed with each other.
Our results indicate that the time to determine Mtb resistance/susceptibility was significantly shorter using the TB-CX compared to IPM and MGIT, an important advantage of the TB-CX in early detection of Mtb drug resistance. The turnaround time of the TB-CX in this study was slightly shorter than previously reported (9, 19), which may be due to the higher bacterial load in the 1 McFarland bacterial suspension compared to that in most sputum samples. In this study, stored Mtb isolates were sub-cultured in LJ tubes, and subsequently used for both the TB-CX and IPM test.
Specifically, compared to MGIT DST, a gold standard for phenotypic DST, the TB-CX exhibited good sensitivity (91%) for detecting isoniazid resistance, but was relatively lower than the reported 98% in a study conducted in Estonia using 201 archived Mtb clinical isolates (12). Additionally, the TB-CX showed strong sensitivity (93%) and specificity (83%) for detecting rifampicin resistance, which was comparable with the 98% sensitivity observed in similar studies comparing the TB-CX with MGIT DST (9, 12). The TB-CX had 100% sensitivity for the detection of MDR-TB, comparable to other studies at 95–99% as well as 86% specificity; although this was slightly lower than reported in other similar studies (9, 12). When compared to IPM assay, it also showed excellent sensitivity (97%) and specificity (90%) for detecting MDR-TB plus moxifloxacin resistant isolates, with a 93% agreement rate.
Interestingly, using the same samples, the sensitivity of the TB-CX to detect rifampicin resistance (93%) was greater than the sensitivity of the IPM test to detect rifampicin resistance (73%) using MGIT as a reference standard. The rifampicin CC of 1 μg/ml used in the IPM test was higher than the 0.5 μg/ml recommended in the latest WHO technical report on CC rifampicin for 7H10 media; however, only limited data are available to determine if the rifampicin CC for 7H11 could be lowered, as reported for 7H10 (20). The increased CC threshold in the CC for the IPM test might explain the decreased sensitivity of the IPM assay to detect rifampicin resistance compared to the TB-CX, as we could expect an increase in false susceptible results (truly resistant strains misclassified as susceptible) and thus, lowering IPM sensitivity.
When compared to the IPM assay, the TB-CX demonstrated a sensitivity of 97% for detecting isoniazid-resistant Mtb isolates. Our study has shown a higher sensitivity than that reported in North East Ethiopia(9), where the sensitivity was only 59%. This could be explained by the fact that our study used archived clinical isolates with standardized inoculum suspensions that may increase the sensitivity of TB-CX when compared to decontaminated sputum samples. Comparable to other studies (9, 12, 21), the TB-CX showed a sensitivity of 82% and a specificity of 80% for rifampicin resistance detection when compared with MGIT DST.
Although no other studies evaluated moxifloxacin resistance, the TB-CX had a sensitivity of 100% and a specificity of 99% in detecting moxifloxacin resistance, which is comparable to a study that evaluated ciprofloxacin (9). These results show excellent agreement between 7H10/7H11 media as previously reported (22), although studies with larger numbers of quinolone resistant Mtb are needed for full assessment.
While TB culture is often prone to contamination, and hence resulting in misdiagnosis or missed diagnosis (14), a method that minimizes contaminations is ideal. The contamination rate for the reference IPM method was compared to the TB-CX. None of the isolates tested by TB-CX showed contaminations, but two of these isolates (2.4%) showed contamination with the IPM method. Similar to the current study, no contamination was reported with other TB-CX studies published previously (9, 12, 14). 7H11 agar has been proposed as an improvement of 7H10 agar (23, 24). The TB-CX has additional reagents to minimize contaminations, such as carbendazim, a fungicide, and Selectatab (11), which is a selective supplement used to suppress the growth of common sputum contaminants.
Despite the potential limitations of the study in using archived Mtb isolates and hence the lack of sensitivity results using fresh specimens (e.g. sputum or lymph node biopsy), our study showed that the TB-CX was quick and simple to use for identifying drug-susceptible, and drug-resistant (including MDR-TB), using stored clinical isolates with good sensitivity and specificity, with shorter time to positive results when compared to IPM and MGIT DST. Because the TB-CX is inexpensive (US$1.2), easy to use, and does not require highly trained personnel, it could be a reliable and economically viable option for DST in resource-limited settings. Diagnosing DR-TB with WHO-approved phenotypic and genotypic methods is often challenging in resource-limited settings, like Ethiopia, since some tests require expensive equipment like MGIT, GeneXpert, and/or sequencing equipment, which also require training, calibration, maintenance, and expensive supplies.
Future studies may evaluate the application of targeted next generation sequencing of DR-TB strains, to also identify rpoB mutations. Conventional phenotypic culture such as LJ and agar-based DST methods also have drawbacks as these take a longer time to deliver test results, which impact patient diagnosis, treatment, and follow-up (13). Future studies may consider implementing the TB-CX for DST of first and second-line anti-TB drugs other than moxifloxacin, using a larger sample size and a variety of other specimens, such as decontaminated sputum samples, stools (for paediatric TB diagnosis and DST), cerebrospinal fluid, and lymph node biopsies. If the TB-CX can improve accuracy in 1st or 2nd line drug resistance detection and turnaround time compared to MGIT SIRE, it could be a major advancement to simplify and decentralize DST capacities in high TB burden, resource constrained settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van Soolingen D, Hoogenboezem T, De Haas PEW, Hermans PWM, Koedam MA, Teppema KS, A Novel Pathogenic Taxon of the Mycobacterium tuberculosis Complex, Canetti: Characterization of an Exceptional Isolate from Africa. International Journal of Systematic and Evolutionary Microbiology. 1997;47(4):1236–45.10.1099/00207713-47-4-12369336935 · doi ↗ · pubmed ↗
- 2World Health Organization. Global tuberculosis report. 2023.
- 3WHO. Global tuberculosis report. 2024.
- 4Jeong Y-J, Park JS, Kim HW, Min J, Ko Y, Oh JY, Deaths from tuberculosis: differences between tuberculosis-related and non-tuberculosis-related deaths. Frontiers in Public Health. 2023;11.10.3389/fpubh.2023.1207284 PMC 1050231437719730 · doi ↗ · pubmed ↗
- 5Dheda K, Mirzayev F, Cirillo DM, Udwadia Z, Dooley KE, Chang K-C, Multidrug-resistant tuberculosis. Nature Reviews Disease Primers. 2024;10(1):22.10.1038/s 41572-024-00504-238523140 · doi ↗ · pubmed ↗
- 6Arinaminpathy N, Mukadi YD, Bloom A, Vincent C, Ahmedov S. Meeting the 2030 END TB goals in the wake of COVID-19: A modelling study of countries in the USAID TB portfolio. PLOS Glob Public Health. 2023;3(10):e 0001271.37870997 10.1371/journal.pgph.0001271 PMC 10593207 · doi ↗ · pubmed ↗
- 7Martin A, Panaiotov S, Portaels F, Hoffner S, Palomino JC, Angeby K. The nitrate reductase assay for the rapid detection of isoniazid and rifampicin resistance in Mycobacterium tuberculosis: a systematic review and meta-analysis. Journal of Antimicrobial Chemotherapy. 2008;62(1):56–64.18407918 10.1093/jac/dkn 139 · doi ↗ · pubmed ↗
- 8Moore DA, Evans CA, Gilman RH, Caviedes L, Coronel J, Vivar A, Microscopic-observation drug-susceptibility assay for the diagnosis of TB. N Engl J Med. 2006;355(15):1539–50.17035648 10.1056/NEJ Moa 055524 PMC 1780278 · doi ↗ · pubmed ↗