Prevalence and correlates of metabolic syndrome in patients with initial-treatment and drug-naïve bipolar disorder: A large sample cross-sectional study
Yilin Fang, Bingchuan Yan, Zhihua Liu, Lin Zhang, Dirceu Mabunda, Dirceu Mabunda, Dirceu Mabunda

TL;DR
This study finds that nearly 18% of bipolar disorder patients who haven't started medication yet have metabolic syndrome, with age and other factors linked to its development.
Contribution
The study is one of the first to examine metabolic syndrome in drug-naïve bipolar disorder patients using a large sample and a novel MetS score.
Findings
Metabolic syndrome prevalence was 17.84% in drug-naïve bipolar disorder patients.
Age, BMI, LDL-C, FT4, and psychotic symptoms were significant predictors of MetS.
Advanced age was linked to higher MetS scores in these patients.
Abstract
Patients with bipolar disorder (BD) are frequently prone to metabolic syndrome (MetS), and their co-morbidity adversely affects patient care outcomes. This study aimed to determine the prevalence of MetS and its clinical correlates among initial-treatment and drug-naïve (ITDN) BD patients.We recruited a cohort of 841 ITDN BD patients. Socio-demographic and clinical data were collected, and patients underwent routine serological testing, which included fasting blood glucose, lipid profiles, thyroid function, and prolactin levels. Psychometric evaluations were also conducted to measure manic, depressive, and psychotic symptoms, as well as illness severity. Additionally, we utilized a transformation approach for continuous variable analysis to compute a MetS score.We found a MetS prevalence of 17.84% among the study participants. Binary logistic regression identified age, body mass index…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
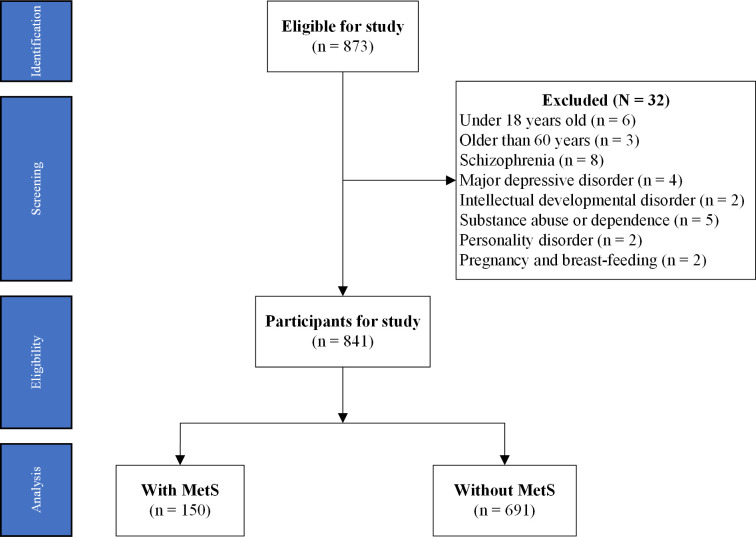 Fig 1
Fig 1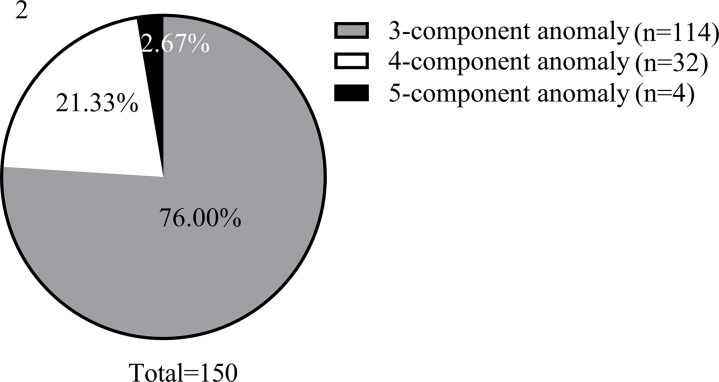 Fig 2
Fig 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBipolar Disorder and Treatment · Diabetes Treatment and Management · Electrolyte and hormonal disorders
1. Introduction
Metabolic syndrome (MetS) is a chronic, non-infectious clinical syndrome characterized by a cluster of vascular risk factors, including insulin resistance, hypertension, abdominal obesity, impaired glucose metabolism, and dyslipidemia [1]. With the global adoption of Western dietary habits [2,3], MetS has surpassed traditional infectious diseases as a significant health threat, increasingly affecting children and adolescents [4,5]. MetS is recognized as a known risk factor that poses a significant threat to somatic health and life expectancy [6,7]. However, the detrimental effects of MetS on patients with BD go far beyond this. The co-occurrence of BD and MetS is associated with worsened executive functioning [8], adverse clinical outcomes [9], and severe cognitive impairments and brain imaging abnormalities [10]. Understanding the clinical features of MetS in BD patients during the initial-treatment and drug-naïve (ITDN) phases and identifying factors that influence its development are crucial for the effective primary prevention of MetS and improving the prognosis in BD.
Emerging evidence suggests a complex relationship between MetS and mood disorders, influenced by clinical, neurobiological, genetic, and environmental factors [11,12]. This link is especially pronounced in individuals with severe mental illnesses such as bipolar disorder (BD), making them vulnerable to MetS [13,14]. While the metabolic adverse effects of antipsychotic medications in BD patients are well-documented [15,16], research focusing on drug-naïve BD populations remains scarce. To date, only a limited number of small-scale studies have explored MetS prevalence in untreated BD patients, reporting heterogeneous rates ranging from 6.5% to 33.3% [17,18]. For instance, a study by Hung Chi et al. involving 60 drug-naïve BD patients in Taiwan reported a MetS prevalence of 16.7% [17], particularly in patients with severe psychiatric disorders who are susceptible to it [18]. These studies, though insightful, are constrained by methodological limitations such as modest sample sizes, regional specificity, and reliance on dichotomous MetS classifications, which fail to capture its severity.
This gap in the literature underscores the need for large-scale, methodologically rigorous investigations to establish robust prevalence estimates and identify clinical correlates of MetS in drug-naïve BD populations. By excluding the confounding effects of psychotropic medications, such studies could elucidate intrinsic metabolic vulnerabilities in BD, offering critical insights for early intervention. Our study directly addresses this gap by examining a large cohort of 841 ITDN BD patients, employing both categorical and continuous MetS assessments. This approach not only refines prevalence estimates but also quantifies metabolic dysfunction severity, advancing understanding of MetS pathophysiology in untreated BD.
2. Participants and methods
2.1. Subjects
The sample size was determined based on prior prevalence studies of MetS in BD cohorts. Assuming an estimated MetS prevalence of 15–25% in untreated BD patients [17,19], a minimum sample of 753 participants was required to achieve 80% power (α = 0.05, two-tailed) for detecting prevalence differences ±5% via χ² tests. Accounting for potential data incompleteness (~10% attrition), the target was set to 811 participants, which also ensured robust multivariate regression analyses (≥10 events per predictor variable [20]).
A total of 841 BD patients with ITDN were prospectively recruited from the Nanyang No. 4 People’s Hospital and Wuhan Mental Health Centre between 10/12/2016 and 10/06/2024. All participants were consecutively enrolled upon their first hospitalization, with eligibility assessed through structured interviews and medical evaluations. Details of the data sources and the study flow are illustrated in Fig 1.
Flow diagram of participants in study.Note: MetS: metabolic syndrome.
The inclusion criteria for participants were as follows:
Diagnosis according to the International Classification of Diseases, 10th edition (ICD-10) for any form of BD, including, but not limited to, bipolar I disorder, bipolar II disorder, manic episodes, depressive episodes, and mixed episodes.First-time hospitalization with no prior exposure to antipsychotics, mood stabilizers, or antidepressants, although use of benzodiazepines was permitted.Age between 18 and 60 years of either sex, and of Han Chinese ethnicity.A score of ≥7 on the 17-item Hamilton Depression Scale (HAMD-17) and/or a score of ≥6 on the Young Mania Rating Scale (YMRS).
Patients were excluded if they:
Were under 18 or over 60 years of age.Had any other psychiatric disorder such as major depressive disorder, schizophrenia spectrum disorder, schizoaffective disorder, personality disorder, substance abuse and dependence, intellectual developmental disorder, etc.Had severe physical illnesses, autoimmune diseases, or acute inflammatory diseases.Patients who were already using hypoglycemic, hypoglycemic, and hypolipidemic medications prior to evaluation were excluded.Were pregnant or lactating.
The study protocol received approval from the Ethics Committee of the Fourth People’s Hospital of Nanyang City (Nanyang Mental Health Centre) under the code 2016-BHD003. Written informed consent was obtained from all participants and/or their guardians.
2.2. Research design
This two-center, cross-sectional study employed a prospective design to evaluate MetS prevalence and correlates in ITDN BD patients. Baseline data were systematically collected during hospitalization, including:
Socio-demographic and general clinical data collection.
Custom Excel forms were used to extract the following information from the electronic case system for included patients: age, age of onset, duration of disease, gender, education, marital status, height, weight, and ethnicity.
Clinical Biochemical parameters and serological tests.
Patients were instructed to fast from 8 PM the previous night, and venous blood samples along with measurements for blood pressure and waist circumference were collected between 6 AM and 8 AM the following morning. All blood samples were immediately processed at the biochemistry laboratory of the attending healthcare facility and analyzed by 11 AM. Key indicators included renal function (uric acid, blood urea nitrogen, blood creatinine), blood lipids (total cholesterol, triglycerides, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol), fasting blood glucose, thyroid function (hyroid-stimulating hormone, free triiodothyronine, free tetraiodothyronine, thyroxine, triiodothyronine) and prolactin levels.
Clinical psychological measures.
Upon admission, patients were evaluated for depressive and manic symptoms, as well as overall illness severity using the Hamilton Depression Scale (HAMD-17) [21], the Young Mania Rating Scale (YMRS) [22], and the Clinical Global Impression Scale-Severity of Illness (CGI-SI) [23], respectively. Additionally, the positive symptom subscale (PSS) of the Positive and Negative Symptom Scale (items P1-P7) was used to assess any comorbid psychotic symptoms in patients [24]. Two attending psychiatrists, who had received uniform training and whose assessments consistently showed correlation coefficients above 0.8 between scales, conducted these evaluations.
Diagnostic criteria for MetS.
According to the standards tailored for the Chinese population by the Chinese Diabetes Society [25], MetS is diagnosed when three or more of the following criteria are met: (1) central or abdominal obesity: waist circumference ≥90 cm for men and ≥85 cm for women; (2) hyperglycemia: fasting blood glucose ≥6.10 mmol/L or 2-hour postprandial glucose ≥7.80 mmol/L, or those diagnosed and treated for diabetes mellitus; (3) hypertension: blood pressure ≥ 130/85 mmHg or those treated for hypertension; (4) elevated fasting triglycerides (TG) ≥ 1.7 mmol/L; (5) reduced fasting high-density lipoprotein cholesterol (HDL-C) < 1.04 mmol/L.
Quantifying MetS severity.
To evaluate MetS severity, it was necessary to convert it from a dichotomous to a continuous variable. First, the mean arterial pressure (MAP) was calculated as one-third systolic blood pressure (SBP) plus two-thirds diastolic blood pressure (DBP). Then, MetS scores were calculated for different genders among Chinese Han adults based on the recent findings of Shujuan Yang et al. [26]:
2.3. Data analysis
We report categorical variables using counts and continuous variables using means and standard deviations. Initially, pie charts were plotted to display the distribution of different MetS subtypes. Subsequently, independent samples t-tests and chi-square tests were used to compare clinical variables between the two subgroups (with and without MetS). A binary logistic regression model was then constructed to identify predictors of MetS development, using MetS as the outcome variable and variables showing significant differences in univariate analyses as independent variables. Finally, a multivariate linear regression model was developed to identify factors predicting the severity of MetS, with MetS scores as the outcome variable and the independent variables identified in the binary logistic regression analyses. Data were analyzed using SPSS version 27.0, with statistical significance set at p < 0.05 (two-tailed).
3. Results
3.1. Prevalence and composition of MetS in the target population
Of the observed target population, 150 cases, or 17.84% (150/841), met the diagnostic criteria for MetS. Fig 2 illustrates the composition of MetS, highlighting that 76.00% of cases exhibited three component anomalies, representing the most common subtype.
Composition ratio for MetS.
3.2. Differences in clinical parameters between subgroups with and without MetS
Table 1 presents a comparison between the subgroups with and without co-morbid MetS, focusing on demographic data and general clinical information. The subgroup with MetS displayed significantly higher levels of several clinical indicators, such as age (t = −2.03, p = 0.042), body mass index (BMI) (t = −4.65, p < .001), low-density lipoprotein cholesterol (LDL-C) (t = −4.31, p < .001), total tetraiodothyronine (TT_4_) (t = −2.83, p = 0.005), free tetraiodothyronine (FT4) (t = −2.66, p = 0.008), Clinical Global Impression Scale-Severity of Illness (CGI-SI) (t = −2.56, p = 0.011), and PSS (t = −4.24, p < .001). Conversely, creatinine (CRE) levels (t = 2.60, p = 0.009) and thyroid-stimulating hormone (TSH) levels (t = 3.43, p = 0.001) were lower in the MetS subgroup.
Table 1: Between-group differences in sociodemographic and general clinical information, grouped by MetS.
3.3. Factors influencing the development of MetS
In Table 2, binary logistic regression models (Backward: Wald) were constructed using MetS as the outcome variable and variables identified in previous univariate analyses (excluding MetS components and scores) as predictors. The analysis revealed that age (B = 0.03, p = 0.006, OR = 1.03, 95% CI: 1.01–1.05), BMI (B = 0.13, p < .001, OR = 1.14, 95% CI: 1.08–1.21), LDL-C (B = 0.45, p = 0.009, OR = 1.57, 95% CI: 1.12–2.20), FT4 (B = 0.97, p = 0.011, OR = 2.65, 95% CI: 1.25–5.63), and PSS (B = 0.37, p < .001, OR = 1.45, 95% CI: 1.37–1.54) significantly positively predicted MetS development. Conversely, CRE (B = −0.04, p < .001, OR = 0.97, 95% CI: 1.01–1.05) and TT_4_ (B = −0.16, p = 0.010, OR = 0.85, 95% CI: 0.75–0.96) were significant negative predictors.
Table 2: Identification of factors affecting the development of MetS: based on a binary logistic regression model.
3.4. Factors influencing the severity of MetS
As depicted in Table 3, multivariate linear regression models were used to identify predictors of MetS severity, with the MetS score as the outcome variable. The results showed that age (B = 0.01, t = 2.60, p = 0.010, 95% CI = 0.00–0.02) and LDL-C (B = 0.18, t = 2.93, p = 0.004, 95% CI = 0.06–0.29) were risk factors for increased MetS severity. In contrast, CRE (B = −0.02, t = −4.08, p < .001, 95% CI = −0.02 - −0.01) and TT_4_ (B = −0.05, t = −2.00, p = 0.047, 95% CI = −0.09–0.00) served as protective factors.
Table 3: Determination of factors affecting the severity of MetS: based on multiple linear regression modelling.
4. Discussion
This study provides novel insights into metabolic dysfunction in BD by uniquely focusing on ITDN patients—a critical yet understudied population that eliminates confounding effects of psychotropic medications. Our cohort (N = 841), rigorously restricted to 18–60 years, minimizes age-related metabolic heterogeneity: younger participants avoid developmental variability (e.g., adolescent hormonal fluctuations), while older adults exclude geriatric comorbidities (e.g., age-driven cardiovascular decline). By employing a dual analytical framework—traditional binary MetS classification and a continuous severity score validated for Chinese Han adults—we capture both diagnostic thresholds and subclinical metabolic gradients. Importantly, age was statistically adjusted in all models and stratified sensitivity analyses confirmed consistent associations across subgroups, reinforcing the robustness of predictors like BMI and LDL-C. This methodological rigor establishes intrinsic metabolic risk profiles in untreated BD, offering a critical baseline for early intervention strategies prior to pharmacotherapy-induced metabolic alterations.
The prevalence of MetS in our ITDN BD cohort (17.84%) is lower than rates reported in treated BD populations (27.5%–53.7%) [13,14,27], aligning with recent findings from drug-naïve studies (6.5%–33.3%) [17,18]. This discrepancy may reflect the absence of antipsychotic exposure in our cohort, a key driver of metabolic dysregulation in BD [16,28]. Notably, Mohd Ahmed et al. (2024) reported a 32.1% MetS prevalence in treated BD patients, attributing elevated risk to antipsychotic polypharmacy and longer illness duration [13]. Similarly, Aziz et al. identified antipsychotic polypharmacy as a significant predictor of MetS in BD, independent of demographic factors [29]. Our lower prevalence underscores the impact of pharmacotherapy on metabolic risk and highlights the need for baseline metabolic profiling in untreated patients.
Our identification of age, BMI, LDL-C, FT4, and psychotic symptoms as predictors of MetS aligns with emerging evidence but also extends prior findings through novel mechanistic insights. While Aziz et al. linked psychotic symptoms to elevated MetS risk via inflammatory pathways in treated BD patients [29], our drug-naïve cohort uniquely implicates LDL-C as a stronger predictor than triglycerides, suggesting lipid dysregulation may precede antipsychotic exposure. This finding contrasts with Mohd Ahmed et al., who emphasized BMI and triglycerides in medicated cohorts [13], highlighting the importance of studying untreated populations to disentangle intrinsic metabolic vulnerabilities. Regarding thyroid dysfunction, our initial statement oversimplified the FT4-MetS link. Beyond incidental associations, thyroid hormones critically regulate metabolic homeostasis through: (1) Lipid Metabolism: FT4 upregulates hepatic lipase activity, accelerating triglyceride hydrolysis and LDL oxidation [30], consistent with our observed LDL-C elevations. (2) Insulin Signaling: Hyperthyroxinemia induces mitochondrial oxidative stress and adiponectin suppression, impairing glucose tolerance even in euthyroid BD patients [31]. (3) Autoimmune-Inflammatory Crosstalk: BD patients exhibit higher anti-thyroid antibody prevalence (e.g., anti-TPO) [32], which synergizes with pro-inflammatory cytokines to promote adipose dysfunction and central obesity [33].
Obesity, or BMI, has traditionally been an independent risk factor for MetS, and BD patients are no exception [18,34]. Our study additionally determined that an increase in BMI per unit leads to a 14% increased risk of developing MetS. Furthermore, we cannot ignore the predictive role of psychotic symptoms for MetS. Unfortunately, studies exploring this predictive ability in BD populations are relatively rare. However, patients with co-morbid MetS have been similarly observed to have more severe psychotic symptoms in patients with schizophrenia spectrum disorders and major depressive disorders, and the predictive ability of the latter for the former component has been affirmed [35–37]. Genetic studies suggest that a shared genetic etiology may be a plausible explanation for the association between the two [38,39]. The association between psychotic symptoms and MetS severity, though underexplored in drug-naïve BD, mirrors findings in schizophrenia [36,37]. This supports a shared biological substrate (e.g., dopamine-glucose metabolism interplay) across severe mental illnesses [38].
The traditional way of defining MetS based on dichotomization has some loopholes as this fails to demonstrate the degree of MetS abnormality, thus limiting its applicability in the clinical setting. To ameliorate these shortcomings, we computed MetS scores and explored in depth the factors that influence the severity oh degree. The present study found that increasing age induces deterioration and exacerbation of MetS. It is well known that MetS is also labelled as one of the classic examples of “age-related metabolic disease” [40]. A combination of aging-induced mitochondrial dysfunction, genetic and environmental factors make age a natural risk factor for the increased incidence and severity of MetS [41,42]. This has been reported in other types of severe psychiatric disorders, in addition to the patients with BD [18,34,43].
However, our study has limitations. The cross-sectional design restricts our ability to infer causality. The scarcity of research on MetS in ITDN BD populations limits the depth of our discussions, and the exclusion of adolescents, who are also affected by MetS, restricts the generalizability of our results. Future research should employ rigorous longitudinal designs to better understand these associations.
5. Conclusions
In summary, this study not only highlights the prevalence of MetS in BD patients with ITDN, but also elucidates clinical factors that are critical to understanding its development and severity. Thyroid dysfunction, high BMI, and co-morbid psychotic symptoms predict MetS development, and higher age implies a more worsened degree of MetS. These findings provide potential targets for MetS prevention and intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Silveira Rossi JL, Barbalho SM, Reverete de Araujo R, Bechara MD, Sloan KP, Sloan LA. Metabolic syndrome and cardiovascular diseases: going beyond traditional risk factors. Diabetes Metab Res Rev. 2022;38(3):e 3502. doi: 10.1002/dmrr.3502 34614543 · doi ↗ · pubmed ↗
- 2Rodríguez-Monforte M, Sánchez E, Barrio F, Costa B, Flores-Mateo G. Metabolic syndrome and dietary patterns: a systematic review and meta-analysis of observational studies. Eur J Nutr. 2017;56(3):925–47. doi: 10.1007/s 00394-016-1305-y 27605002 · doi ↗ · pubmed ↗
- 3Shab-Bidar S, Golzarand M, Hajimohammadi M, Mansouri S. A posteriori dietary patterns and metabolic syndrome in adults: a systematic review and meta-analysis of observational studies. Public Health Nutr. 2018;21(9):1681–92. doi: 10.1017/S 1368980018000216 29559025 PMC 10261419 · doi ↗ · pubmed ↗
- 4Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep. 2018;20(2):12. doi: 10.1007/s 11906-018-0812-z 29480368 PMC 5866840 · doi ↗ · pubmed ↗
- 5Noubiap JJ, Nansseu JR, Lontchi-Yimagou E, Nkeck JR, Nyaga UF, Ngouo AT, et al. Global, regional, and country estimates of metabolic syndrome burden in children and adolescents in 2020: a systematic review and modelling analysis. Lancet Child Adolesc Health. 2022;6(3):158–70. doi: 10.1016/S 2352-4642(21)00374-6 35051409 · doi ↗ · pubmed ↗
- 6Li D, Wang L, Zhou Z, Song L, Chen S, Yang Y, et al. Lifetime risk of cardiovascular disease and life expectancy with and without cardiovascular disease according to changes in metabolic syndrome status. Nutr Metab Cardiovasc Dis. 2022;32(2):373–81. doi: 10.1016/j.numecd.2021.10.014 34893414 · doi ↗ · pubmed ↗
- 7Saccaro LF, Aimo A, Panichella G, Sentissi O. Shared and unique characteristics of metabolic syndrome in psychotic disorders: a review. Front Psychiatry. 2024;15:1343427. doi: 10.3389/fpsyt.2024.1343427 38501085 PMC 10944869 · doi ↗ · pubmed ↗
- 8Dalkner N, Bengesser SA, Birner A, Fellendorf FT, Fleischmann E, Großschädl K, et al. Metabolic syndrome impairs executive function in bipolar disorder. Front Neurosci. 2021;15:717824. doi: 10.3389/fnins.2021.717824 34456679 PMC 8385126 · doi ↗ · pubmed ↗