Spatial distribution of pathogenic fungal isolates from clinical samples in Uganda: Diagnostic gaps and trends, January 2020 - May 2024
Priscilla Atim, Samuel Gidudu, Bernard Ssentalo Bagaya, Andrew Kambugu, Grace Najjuka, Atuhaire D. Winfred, Benedict Kanamwanji, Esther Nabende, Adella Atukunda, Jonathan Kabazzi, Sylvia Joyoo, Hildah Tendo Nansikombi, Alex Riolexus Ario

TL;DR
This study analyzed fungal infections in Uganda from 2020 to 2024, finding most cases in women aged 16–35 and highlighting diagnostic gaps.
Contribution
The study provides the first detailed analysis of fungal pathogen distribution in Uganda over a five-year period.
Findings
Candida species were the most common fungal pathogens, especially in women and young adults.
Diagnostic capacity for fungal infections in Uganda is limited, with disruptions noted during the pandemic.
Most infections were identified in Kampala and Mbarara districts, suggesting regional hotspots.
Abstract
Pathogenic fungi cause approximately 13 million infections and 1.5 million deaths worldwide each year, yet surveillance and diagnosis remain inadequate in resource-limited settings. In Uganda, fungal infections affect approximately 4,099,357 per 45 million people annually, resulting in severe invasive diseases if untreated. This study describes laboratory-confirmed pathogenic fungal isolates from clinical samples in Uganda from January 2020 to May 2024, and highlights gaps in diagnostic capacity. We abstracted data from the National Microbiology Reference Laboratory database, disaggregated pathogenic fungal isolates by the sex and age group of the patients, sample type, and isolated species, district, and year of isolation. Pathogenic fungal isolates were confirmed by culture and biochemical tests. Using Epi Info 7 software, we analyzed frequencies. Among 8,136 clinical samples…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
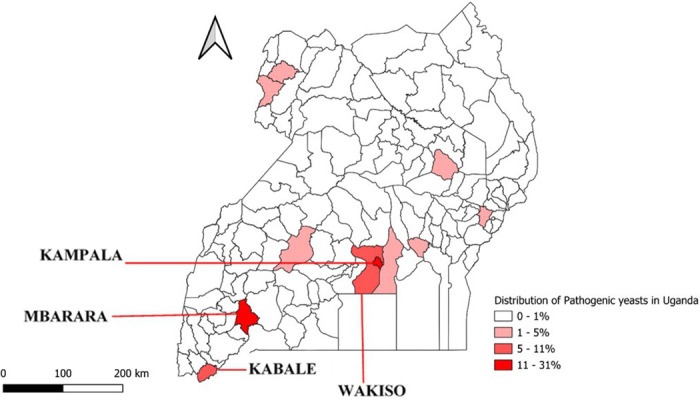 Fig 1
Fig 1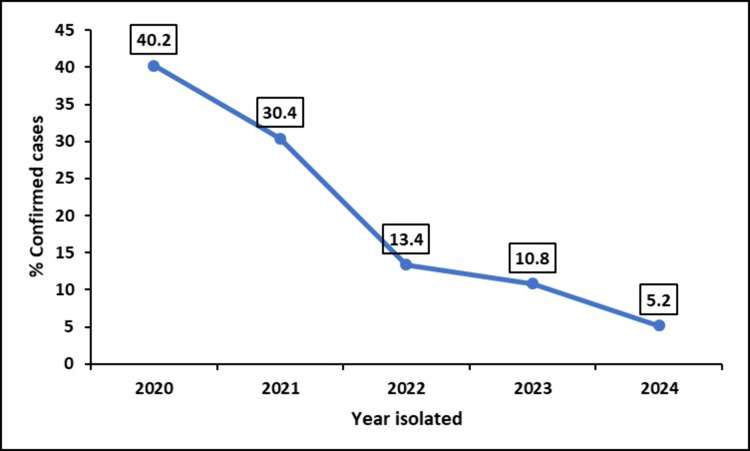 Fig 2
Fig 2- —http://dx.doi.org/10.13039/100009054U.S. President’s Emergency Plan for AIDS Relief
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Plant Pathogens and Fungal Diseases
Introduction
Pathogenic fungi cause a spectrum of fungal infections, ranging from superficial to life-threatening invasive diseases [1]. Globally, they are responsible for a staggering 13 million fungal infections and 1.5 million deaths each year, especially among immunocompromised patients [2]. In 2024, the annual burden of fungal infections in Uganda was estimated to be approximately 4,099,357 cases [3]. These infections are common opportunistic infections associated with chronic diseases such as HIV, tuberculosis, diabetes mellitus, chronic lung diseases, cancer and asthma [4]. They also frequently affect severely ill patients in intensive care units, patients undergoing invasive medical procedures, and those taking immunosuppressants and broad-spectrum antibiotics [4]. Although fungal infections are commonly reported in immunocompromised patients [5], emerging evidence indicates an increasing number of cases in immunocompetent individuals [6–8]. However, the actual burden of fungal infections in Uganda remains unknown due to lack of comprehensive diagnostic capacity and surveillance.
In response to the growing threat of fungal pathogens, the World Health Organization (WHO) has increased its efforts to improve the surveillance of pathogenic fungi. As a result, WHO published its first fungal pathogen priority list in 2022 [9]. On the critical list are C. albicans, C. auris, C. neoformans and A. fumigatus; while other high-priority pathogens include C. glabrata, Histoplasma spp., Mucorales, Fusarium spp*., C. tropicalis,* and C. parapsilosis [9]. Among these, the Candida spp., C. neoformans and A. fumigatus are the leading causes of fungal-related morbidity and mortality in humans [10]. In Uganda, Candida spp. are often isolated from high vaginal swabs, while and C. neoformans is commonly isolated from cerebrospinal fluid samples, in HIV patients [3].
Despite initiatives such as AIDS control programs that have improved outcomes for HIV/AIDS patients with opportunistic infections [11], inadequate fungal diagnostics remain a critical barrier to effective disease management. In Regional Referral Hospital laboratories (RRHs), fungal diagnosis relies on direct microscopy, culture and Cryptococcal Antigen Lateral flow assays (CrAg). At the National Microbiology Reference Laboratory (NMRL), fungal pathogens are confirmed by culture and biochemical tests. However, the laboratories do not perform antifungal susceptibility testing due to lack of infrastructure. These constraints not only contribute to underreporting and misdiagnosis [12] but also inadequate public health interventions [13,14].
This study describes laboratory-confirmed pathogenic fungi isolated from clinical samples in Uganda from January 2020 to May 2024, highlighting the need for improved diagnostic infrastructure and surveillance.
Methods
Study design and setting
We conducted a descriptive analysis of laboratory-confirmed pathogenic fungal isolates from January 2020 to May 2024. Data were obtained from the National Microbiology Reference Laboratory (NMRL) database. The NMRL, a government laboratory accredited by the College of American Pathologists (CAP), conducts routine sample testing requested by clinicians in Kampala and Wakiso districts which serve as central healthcare hubs. Additionally, NMRL performs quality checks by retesting isolates received from all regional referral hospitals (RRHs) in Uganda, ensuring the quality and completeness of the national fungal pathogen dataset.
Procedure for fungal detection in Uganda
Samples are referred to the NMRL using a national microbiology request form. In regional referral hospitals, fungi are diagnosed in the laboratory using direct microscopy, culture and CrAg tests, which are cost-effective methods commonly available in RRHs. Samples are then referred to NMRL for confirmation and further identification. If the RRHs do not have preliminary testing capacity, the samples are still directly referred to the NMRL. Once received, patient data are transferred to the NMRL information system, which automatically assigns a unique laboratory identification. At NMRL, fungi are identified using a combination of culture on Sabouraud Dextrose Agar (SDA), germ tube testing to differentiate C. albicans, India ink for C. neoformans, biochemical urea testing for urease-producing fungi.
Clinical sample types were also categorized into superficial and deep samples. Superficial samples were obtained from non-sterile body sites, including cutaneous samples, mucosal samples, catheter swabs and urine samples. Deep samples were collected from sterile internal body sites, such as CSF, blood, pleural fluid.
Data abstraction, sources and analysis
We abstracted data on pathogenic fungal isolates from January 2020 to May 2024 from the NMRL database. The data included the sex and age group of the patients, sample type, isolated fungal species, district, and year of isolation. These data were then entered into Epi Info 7 software for analysis. We computed the frequency and proportion of confirmed pathogenic fungal isolates by the sex and age group of the patients, isolated species, sample type, district and year of isolation.
All data were accessed for research purposes between 01/05/2024 and 30/05/2024. No Personal Identifiable Information (PID) was used in this study, as all PIDs were blinded and replaced with laboratory-generated code numbers to ensure anonymity. Data were securely stored within NMRL, with restricted access requiring authorization.
Ethical considerations and consent to participate
Our study utilized routinely generated secondary aggregated data with no personal identifiers in health facility outpatient and in-patient monthly reports, obtained from the NMRL database. The Uganda Public Health Fellowship Program operates under the Ministry of Health (MoH) and is part of the National Rapid Response Team, and has been granted permission to access and analyze surveillance data in the DHIS-2 and other data such as survey and field investigation data to inform decision making in the control and prevention of outbreaks and public health programming. Additionally, the MOH has also granted the program permission to disseminate the information through scientific publications. This analysis was authorized by MoH and classified as non-research, and as per our memorandum of understanding, it was exempt from full Institutional Review Board review, primarily aimed at public health practice. We stored the abstracted data set in a password-protected computer and only shared it with the investigation team. This study adhered to the principles outlined in the declaration of Helsinki and was conducted in accordance with national guidelines. All procedures involving human data were performed in compliance with these ethical standards.
Results
Description of confirmed pathogenic fungal cases
Among the 8,136 clinical samples tested, pathogenic fungi were confirmed in 744 (9%) samples from January 2020–May 2024. Among the 744 confirmed fungal isolates, most were from female (92%), aged 16–35 years (68%). C. albicans was the most common (65.4%) Table 1.
Table 1: Confirmed pathogenic fungal isolates in Uganda, January 2020-May 2024.
Pathogenic fungal species isolated by sample type
Candida and Cryptococcus were the only fungal genera isolated. The majority of the laboratory-confirmed pathogenic fungal isolates (526/744, 71%) were detected in high vaginal swab (HVS) samples (Table 2). Of all analyzed clinical samples, 93.7% were classified as superficial, while 6.3% were classified as deep. Cutaneous samples were not present in the dataset. C. albicans was predominantly detected in superficial samples, whereas C. neoformans was detected only in deep samples (CSF). Isolates from HVS samples included C. albicans (378/487, 78%) and non-albicans Candida spp. (148/228, 65%). The laboratory did not have the capacity to identify specific non*-albicans Candida* spp. All CSF samples that tested positive for fungal infections (29 (100%) were infected with C. neoformans (Table 2).
Table 2: Pathogenic fungal isolates by sample type in Uganda from January 2020 to May 2024.
The percentage of confirmed pathogenic fungal isolates by district ranged from 0–32%. The majority of confirmed pathogenic fungal isolates were from Kampala (32%) and Mbarara (26%) districts (Fig 1).
Proportion of confirmed pathogenetic fungal isolates by district in Uganda from January 2020–May 2024.(Map drawn using QGIS 3.32.2, link to base layer shape file. https://www.naturalearthdata.com/downloads/).
We observed a gradual decline in the number of confirmed pathogenic fungal isolates from 40% in 2020 to 5% in 2024 (Fig 2).
Proportion of confirmed pathogenic fungal isolates over time in Uganda from 2020 to 2024.
Discussion
This study identified a sex, age and geographical disparity in the distribution of pathogenic fungal isolates in Uganda, with most cases detected among females and youths. The majority of pathogenic fungal isolates in our dataset were among persons from Kampala and Mbarara districts.
Our findings confirm that Candida spp., remain the most predominant fungal pathogens in Uganda [15], accounting for 66% of all isolates. While these results are consistent with global trends, [16,17], they highlight the need for improved diagnostic capacity to identify and manage non-albicans Candida spp., which are emerging as significant pathogens with varied antifungal resistance patterns [17–19]. Although the laboratory was able to identify C. albicans, it lacked the capacity to identify other Candida spp. or perform antifungal testing. Clinical fungal diagnosis in Ugandan laboratories is largely limited to the genus level of Candida and Cryptococcus, with no diagnostic capacity for other clinically significant fungi. This gap in diagnosis impedes effective clinical management and antifungal stewardship [3].
C. neoformans was identified in all the CSF samples that tested positive. Previous studies in Uganda have shown a high prevalence of cryptococcosis as an opportunistic infection in HIV patients with a rate of 60% [20]. Our results were consistent with these estimates. While many HIV/AIDS patients are diagnosed and treated through AIDS control programs that have been established in the country [11], these findings emphasize the need to expand diagnostic capacity and provide additional support to the National Microbiology Reference Laboratory [11]. This would ensure consistent and accessible diagnosis of cryptococcal meningitis across the healthcare system.
Our results showed that the majority of pathogenic fungal isolates were from females, consistent with the literature suggesting higher susceptibility among females to candida yeast infections [21], particularly during childbearing age [22]. Hormonal changes during pregnancy or from obesity, as well as the use of broad-spectrum antibiotics and high-dose estrogen birth control pills, contribute to this susceptibility [23]. While candida infections are common in sexually active women, data on sexually transmitted candida infections remain insufficient [21]. The dataset that we analyzed did not provide details about the sexual activity of this population. However, persons aged 16–35 years, who account for the highest proportion of infections, are typically sexually active. This disparity underscores the need for targeted education and preventive measures against candidiasis for women, especially those in high-risk groups.
Fungal pathogens were isolated from both localized superficial clinical samples and invasive deep samples. Candida spp. were isolated from all superficial clinical samples, which represent the most common sample type associated with candidiasis in both healthy and immunocompromised individuals [24]. The high proportion of isolates from high vaginal swabs correlates with the high number of female patient cases in the study dataset. Urine samples accounted for 14% of the pathogenic fungal isolates, suggesting vaginal and urinary tract yeast colonization. While yeast urinary tract infections are rare in healthy individuals, they are commonly detected in hospitalized patients and those with underlying medical conditions [25]. Candidemia caused by both albicans and non*-albicans Candida* was reported in 1% of the samples. The mortality rate from candidemia remains high, ranging from approximately 46% to 70% [26,27]. In addition, candidemia is associated with longer hospital stays and increased physical complications, which can be averted with early diagnosis and treatment [28]. While the overall burden of candidemia remains unknown in Uganda, our findings indicate that C. albicans is the most frequently isolated fungal species from bloodstream infections [29]. Other sample types, including CSF, sputum, and stool, and various swabs (ear, cervix, pus, wound, and urethra) each contributed less than 5% of the total isolates, highlighting the different clinical sources from which fungal pathogens were isolated. Most of these were among persons from Kampala and Mbarara districts, suggesting not only a regional hotspot but also the presence of access to healthcare facilities in these urban centers for fungal infections that warrants further investigation. In addition, Kampala and Mbarara have the most healthcare facilities in the country, thus improving access to healthcare [30]. This, together with more health-seeking behavior, could have contributed to the high proportion of samples from Kampala and Mbarara districts.
The number of confirmed pathogenic fungal isolates decreased from 40% in 2020 to 5% in 2024. While part of this decline can be attributed to the limited data collection period in 2024 only up to May, the COVID-19 pandemic played a significant role in disrupting routine diagnostics and laboratory services. During this time, resources were reallocated to address SARS-CoV-2 testing, leading to reduced surveillance for other infections, increased misdiagnosis, and reliance on over-the-counter medications [14,31,32]. This disruption highlights the fragility of diagnostic systems in low- and middle-income countries, and emphasizes the need to build resilient national healthcare infrastructure capable of maintaining routine surveillance during public health emergencies [33].
Study limitations
Our findings were limited to fungi genera (Candida and Cryptococcus) due to the diagnostic capacity of the National Microbiology Reference Laboratory. The laboratory lacked the resources and infrastructure to specifically identify non-albicans Candida spp. and other fungal pathogens, such as Aspergillus spp*., Histoplasma* spp., which may also contribute to morbidity. Cutaneous samples were not present in the dataset, showing a diagnostic focus on systemic infections rather than cutaneous and dermatological fungal isolates. This absence may contribute to a lower estimate of the overall fungal infection burden. In addition, the laboratory lacks capacity to perform antifungal susceptibility testing, creating a gap in understanding the true burden of these fungal infections [34]. This highlights the need to expand fungal diagnostic capacity in Uganda to improve the detection and comprehensive management of clinical fungal pathogens.
Conclusions
This study highlights a high proportion of Candida spp. isolates among females, persons aged 16–35 years, and those in Kampala and Mbarara districts. There is need to improve diagnostic capacity and establish surveillance systems for pathogenic fungal isolates in Uganda.
We recommend establishing a dedicated and equipped national mycology program to enhance diagnostic capacity and surveillance. The Ministry of Health Uganda would benefit from prioritizing resource allocation, staff training, and the provision of necessary equipment to build this capacity. This will enable comprehensive data collection to assess the true burden of fungal infections in the country and facilitate effective public health interventions. Additionally, it will align with global efforts to combat the rising threat of fungal pathogens.
Supporting information
S1 DatasetDataset used for analysis of pathogenic fungal isolates from clinical samples in Uganda (January 2020 - May 2024).(XLS)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Walsh TJDD. Spectrum of mycoses. In: Baron S, editor. Medical microbiology, Vol. 4. Galveston (TX): University of Texas Medical Branch at Galveston; 1996.21413276 · pubmed ↗
- 2Rayens E, Norris KA. Prevalence and healthcare burden of fungal infections in the United States, 2018. Open Forum Infect Dis. 2022;9(1):ofab 593. doi: 10.1093/ofid/ofab 593 35036461 PMC 8754384 · doi ↗ · pubmed ↗
- 3Bongomin F, Kwizera R, Namusobya M, van Rhijn N, Andia-Biraro I, Kirenga BJ, et al. Re-estimation of the burden of serious fungal diseases in Uganda. Ther Adv Infect Dis. 2024;11:20499361241228345. doi: 10.1177/20499361241228345 38328511 PMC 10848809 · doi ↗ · pubmed ↗
- 4Bongomin F, Gago S, Oladele RO, Denning DW. Global and multi-national prevalence of fungal diseases—estimate precision. Jo F. 2017;3.10.3390/jof 3040057 PMC 575315929371573 · doi ↗ · pubmed ↗
- 5Mei-Sheng Riley M. Invasive fungal infections among immunocompromised patients in critical care settings: infection prevention risk mitigation. Crit Care Nurs Clin North Am. 2021;33(4):395–405. doi: 10.1016/j.cnc.2021.07.002 34742496 · doi ↗ · pubmed ↗
- 6Fisher JF, Valencia-Rey PA, Davis WB. Pulmonary cryptococcosis in the immunocompetent patient-Many questions, some answers. Open Forum Infect Dis. 2016.10.1093/ofid/ofw 167PMC 504741227704021 · doi ↗ · pubmed ↗
- 7Rudramurthy SM, Singh S. Candida infections in immunocompetent hosts: pathogenesis and diagnosis. Curr Fungal Infect Rep. 2020;14(3):233–45. doi: 10.1007/s 12281-020-00392-5 · doi ↗
- 8Di Mango AL, Zanetti G, Penha D, Menna Barreto M, Marchiori E. Endemic pulmonary fungal diseases in immunocompetent patients: an emphasis on thoracic imaging. Expert Rev Respir Med. 2019;13(3):263–77. doi: 10.1080/17476348.2019.1571914 30668231 · doi ↗ · pubmed ↗