Unraveling the Yellow Mystery: Severe Jaundice and Multisystem Collapse in a Returning Traveler
Bharadwaj Adithya Sateesh, Natalie Shammas, Ahmed Abdelfattah, Jarmil Alyssa Peters, Kristin Dishongh, Ashley Jenkins, John Mark P Pabona

TL;DR
A 43-year-old man with a travel history and possible toxic exposure died from severe jaundice and multiorgan failure, highlighting the dangers of undiagnosed liver and pancreatic diseases.
Contribution
This case highlights the diagnostic challenges and fatal outcomes of overlapping hepatic and pancreatic pathologies due to unclear toxic exposure.
Findings
The patient exhibited multiorgan dysfunction including acute renal failure, rhabdomyolysis, and disseminated intravascular coagulation.
Liver biopsy showed cirrhosis with cholestasis, ballooning degeneration, and bridging fibrosis.
Hemorrhagic pancreatitis with retroperitoneal gas was observed, suggesting pancreatic gas gangrene.
Abstract
We present the case of a 43-year-old male with recent travel history and possible toxic exposure abroad who was admitted with altered mental status following a seizure. His course was complicated by multiorgan dysfunction, including acute renal failure, rhabdomyolysis, acute pancreatitis, disseminated intravascular coagulation, and severe jaundice. Extensive infectious and autoimmune workup was unrevealing. Imaging revealed hepatosplenomegaly, hemorrhagic ascites, and progressive pancreatic inflammation. Liver biopsy demonstrated cirrhosis with cholestasis, ballooning degeneration, Mallory hyaline, and bridging fibrosis. Despite supportive care, the patient developed hemorrhagic pancreatitis with retroperitoneal gas, concerning for pancreatic gas gangrene. Surgical intervention was not feasible, and the patient ultimately succumbed to his illness. This case underscores the diagnostic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
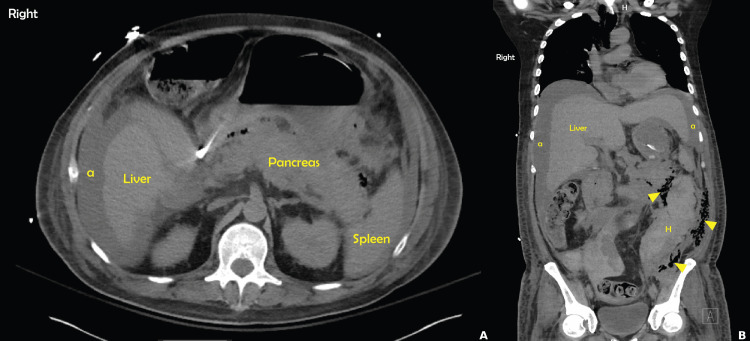 Figure 1
Figure 1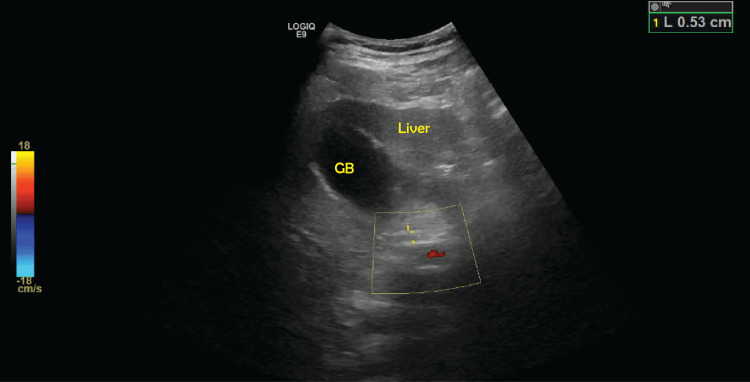 Figure 2
Figure 2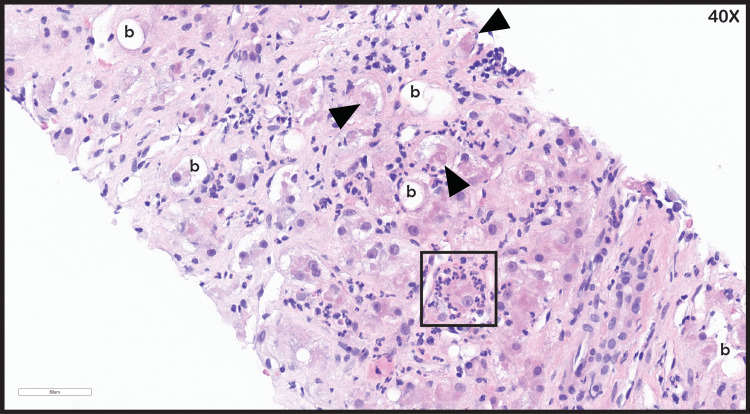 Figure 3
Figure 3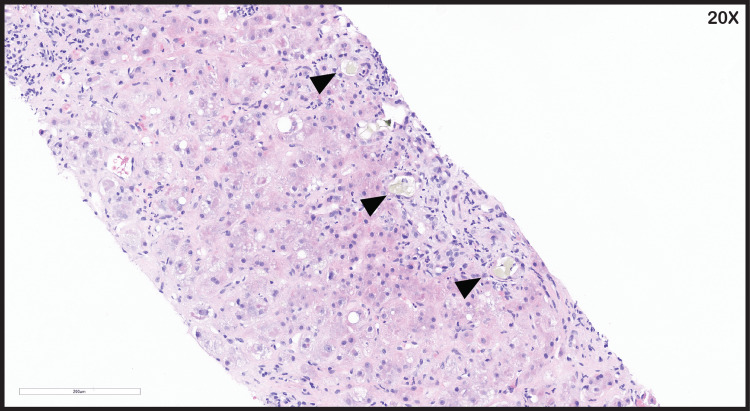 Figure 4
Figure 4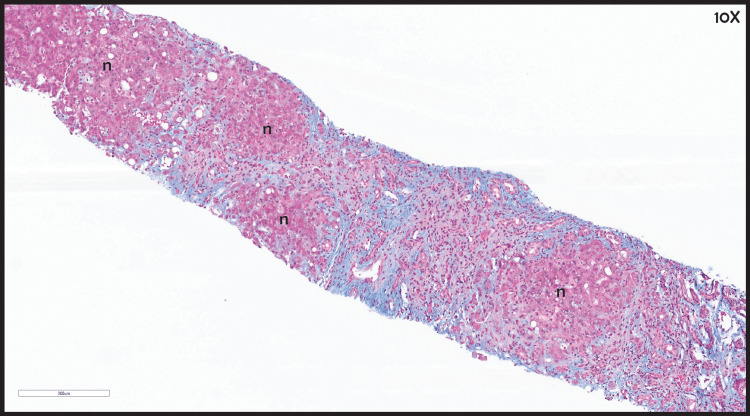 Figure 5
Figure 5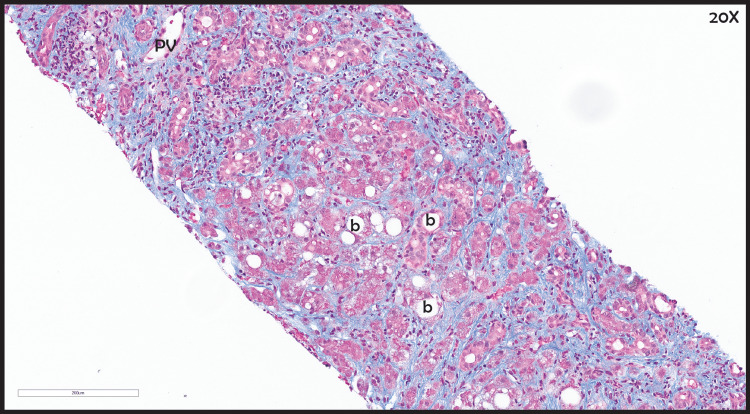 Figure 6
Figure 6| Day of admission | WBC (4.5-11.0 K/uL) | RBC (4.50-5.90 M/uL) | Hemoglobin (13.5-17.5 g/dL) | Hematocrit (41.0-53.0 %) | Platelets (150-400 K/uL) | MPV (7.4-10.4 fL) |
| Day 1 | 11.9 (H) | 4.43 (L) | 11.6 (L) | 34 (L) | 136 (L) | 10.9 (H) |
| Day 2 | 5.2 | 3.60 (L) | 8.8 (L) | 25.9 (L) | 61 (L) | 11.6 (H) |
| Day 3 | 14.6 (H) | 2.80 (L) | 7.4 (L) | 22.8 (L) | 72 (L) | 11.8 (H) |
| Day 4 | 14.2 (H) | 2.47 (L) | 7.9 (L) | 23.9 (L) | 60 (L) | 12.7 (H) |
| Day 5 | 11.2 (H) | 2.56 (L) | 8.0 (L) | 23.4 (L) | 70 (L) | 11.8 (H) |
| Day 6 | 8.8 | 2.44 (L) | 7.7 (L) | 22.3 (L) | 59 (L) | 13.2 (H) |
| Day 7 | 6.9 | 2.37 (L) | 8.8 (L) | 26 (L) | 37 (LL) | 10.4 |
| Day 8 | 7.5 | 2.63 (L) | 8.1 (L) | 23.5 (L) | 110 (L) | 11.3 (H) |
| Day 9 | 7.8 | 2.83 (L) | 8.6 (L) | 25.0 (L) | 101 (L) | 12.0 (H) |
| Day 10 | 12.3 (H) | 2.84 (L) | 8.8 (L) | 26.4 (L) | 110 (L) | 12.3 (H) |
| Day 11 | 15.7 (H) | 2.80 (L) | 8.7 (L) | 26.7 (L) | 141 (L) | 12.7 (H) |
| Day 12 | 15.1 (H) | 2.37 (L) | 7.5 (L) | 23.2 (L) | 169 | 12.5 (H) |
| Day 13 | 20.8 (H) | 2.68 (L) | 8.3 (L) | 25.7 (L) | 235 | 12.0 (H) |
| Day 14 | 18.3 (H) | 2.57 (L) | 8.1 (L) | 25.2 (L) | 229 | 12.2 (H) |
| Day 15 | 15.2 (H) | 2.27 (L) | 7.0 (L) | 22.4 (L) | 257 | 11.3 (H) |
| Day 16 | 13.2 (H) | 2.20 (L) | 7.9 (L) | 23.9 (L) | 268 | 11.2 (H) |
| Day 17 | 12.1 (H) | 2.60 (L) | 8.1 (L) | 24.2 (L) | 242 | 11.1 (H) |
| Day 18 | 10.8 | 2.47 (L) | 7.6 (L) | 23.2 (L) | 211 | 10.9 (H) |
| Day 19 | 9.5 | 2.29 (L) | 7.1 (L) | 21.4 (L) | 193 | 11.2 (H) |
| Day 20 | 10.0 | 2.27 (L) | 7.1 (L) | 21.5 (L) | 180 | 11.1 (H) |
| Day 21 | 13.5 (H) | 2.50 (L) | 8.0 (L) | 23.3 (L) | 268 | 11.6 (H) |
| Day 22 | 14.1 (H) | 2.31 (L) | 7.5 (L) | 22.1 (L) | 394 | 10.5 (H) |
| Day 23 | 17.7 (H) | 3.00 (L) | 9.3 (L) | 27.8 (L) | 488 (H) | 10.5 (H) |
| Day 24 | 23.2 (H) | 2.78 (L) | 8.7 (L) | 26.0 (L) | 525 (H) | 9.9 |
| Day 25 | 18.0 (H) | 2.76 (L) | 8.7 (L) | 25.4 (L) | 505 (H) | 9.5 |
| Day 26 | 22.0 (H) | 2.83 (L) | 8.8 (L) | 25.8 (L) | 490 (H) | 9.3 |
| Day 27 | 16.7 (H) | 2.30 (L) | 5.9 (LL) | 18.1 (LL) | 308 | 9.8 |
| Day 28 | 30.4 (HH) | 2.11 (L) | 7.6 (L) | 23.0 (L) | 359 | 10.2 |
| Day 29 | 24.0 (H) | 2.13 (L) | 7.3 (L) | 21.5 (L) | 309 | 9.9 |
| Day of admission | Sodium (136-145 mmol/L) | Potassium (3.5-5.1 mmol/L) | Creatinine (0.72-1.25 mg/dL) | Chloride (98-107 mmol/L) | CO2 (22-29 mmol/L) | Calcium (8.4-10.2 mg/dL) | BUN (7-26 mg/dL) | Glucose (74-99 mg/dL) | GFR (≥60 mL/min/1.73m²) | Anion gap (8-16 mmol/L) | Osmolality (275-295 mOsm/kg) | Total protein (6.4-8.3 g/dL) | Albumin (3.5-5.0 g/dL) | Bilirubin total (0.2-1.2 mg/dL) | Direct bilirubin (0.1-0.5 mg/dL) | ALP (40-150 U/L) | AST (5-34 U/L) | ALT (<55 U/L) |
| Day 1 | 141 | 4.4 | 3.00 (H) | 104 | 12 (LL) | 10.5 (H) | 25 (H) | 246 (H) | 23 (L) | 40 (H) | 298 (H) | 9.6 (H) | 4.5 | 8.8 (H) | - | 153 (H) | 132 (H) | 75 (H) |
| Day 2 | 141 | 2.8 (LL) | 4.13 (H) | 99 | 13 (LL) | 6.2 (L) | 25 | 325 (H) | 17 (L) | 29 (H) | 293 | 6.3 (L) | 3.0 (L) | 7.9 (H) | - | 109 | 142 (H) | 53 |
| Day 3 | 138 | 4.1 | 3.91 (H) | 94 (L) | 15 (LL) | 5.0 (LL) | 31 (H) | 293 (H) | 19 (L) | 29 (H) | 293 | 5.0 (L) | 2.3 (L) | 6.6 (H) | - | 62 | 144 (H) | 55 (H) |
| Day 4 | 138 | 4.2 | 4.28 (H) | 93 (L) | 14 (LL) | 5.0 (LL) | 34 (H) | 279 (H) | 17 (L) | 31 (H) | 296 (H) | 5.5 (L) | 2.8 (L) | 6.7 (H) | - | 52 | 145 (H) | 49 |
| Day 5 | 138 | 3.9 | 3.07 (H) | 91 (L) | 28 | 4.8 (LL) | 40 (H) | 150 (H) | 25 (L) | 19 (H) | 288 | 5.6 (L) | 2.5 (L) | 7.6 (H) | - | 69 | 122 (H) | 39 |
| Day 6 | 141 | 3.6 | 3.00 (H) | 92 (L) | 30 (H) | 6.0 (LL) | 46 (H) | 131 (H) | 26 (L) | 19 (H) | 295 | 6.0 (L) | 2.9 (L) | 10.0 (H) | - | 163 (H) | 142 (H) | 53 |
| Day 7 | 147 (H) | 2.6 (LL) | 2.54 (H) | 98 | 30 (H) | 6.0 (LL) | 82 (H) | 145 (H) | 31 (L) | 19 (H) | 320 (H) | 6.0 (L) | 2.9 (L) | 11.3 (H) | - | 302 (H) | 144 (H) | 55 (H) |
| Day 8 | 150 (H) | 2.9 (LL) | 1.69 (H) | 99 | 33 (H) | 6.0 (LL) | 93 (H) | 208 (H) | 51 (L) | 18 (H) | 333 (H) | 6.2 (L) | 2.6 (L) | 6.9 (H) | - | 63 | 151 (H) | 51 |
| Day 9 | 154 (H) | 3.3 (L) | 1.26 (H) | 101 | 36 (H) | 6.2 (L) | 94 (H) | 208 (H) | >60 | 17 (H) | 341 (H) | 6.2 (L) | 2.4 (L) | 16.5 (H) | - | 391 (H) | 81 (H) | 81 (H) |
| Day 10 | 151 (H) | 3.5 | 0.89 | 106 | 31 (H) | 6.3 (L) | 87 (H) | 145 (H) | >60 | 14 | 329 (H) | 5.6 (L) | 2.0 (L) | 21.3 (HH) | - | 314 (H) | 41 (H) | 62 (H) |
| Day 11 | 151 (H) | 4.1 | 0.80 | 115 (H) | 25 | 7.7 (L) | 54 (H) | 136 (H) | >60 | 11 | 317 (H) | 5.4 (L) | 2.0 (L) | 23.6 (HH) | - | 263 (H) | 53 (H) | 53 |
| Day 12 | 146 (H) | 5.0 | 0.91 | 115 (H) | 22 | 8.0 (L) | 47 (H) | 197 (H) | >60 | 9 | 308 (H) | 5.7 (L) | 1.8 (L) | 23.2 (HH) | - | 212 (H) | 45 (H) | 46 |
| Day 13 | 148 (H) | 4.0 | 0.99 | 114 (H) | 20 (L) | 8.3 (L) | 44 (H) | 93 | >60 | 14 | 305 (H) | 5.8 (L) | 2.2 (L) | 22.5 (HH) | - | 217 (H) | 44 (H) | 47 |
| Day 14 | 149 (H) | 4.0 | 0.89 | 116 (H) | 21 (L) | 8.3 (L) | 42 (H) | 82 | >60 | 12 | 306 (H) | 5.9 (L) | 2.2 (L) | 20.2 (HH) | - | 240 (H) | 52 (H) | 51 |
| Day 15 | 149 (H) | 3.8 | 0.78 | 119 (H) | 20 (L) | 8.1 (L) | 37 (H) | 116 (H) | >60 | 10 | 306 (H) | 5.8 (L) | 2.3 (L) | 25.1 (HH) | 13.1 | 288 (H) | 51 (H) | 48 |
| Day 16 | 153 (H) | 3.7 | 0.70 (L) | 122 (HH) | 19 (L) | 8.1 (L) | 30 (H) | 138 (H) | >60 | 12 | 312 (H) | 5.6 (L) | 2.3 (L) | 26.0 (HH) | 11.2 | 329 (H) | 52 (H) | 52 |
| Day 17 | 148 (H) | 3.1 (L) | 0.70 (L) | 118 (H) | 19 (L) | 7.7 (L) | 28 (H) | 146 (H) | >60 | 11 | 302 (H) | 5.4 (L) | 2.3 (L) | 26.1 (HH) | 10.5 | 357 (H) | 61 (H) | 50 |
| Day 18 | 144 | 3.4 (L) | 0.68 (L) | 115 (H) | 23 | 8.0 (L) | 27 (H) | 124 (H) | >60 | 6 (L) | 293 | 5.7 (L) | 2.3 (L) | 25.0 (HH) | 10.4 | 366 (H) | 57 (H) | 48 |
| Day 19 | 138 | 3.9 | 0.63 (L) | 109 (H) | 21 (L) | 8.2 (L) | 24 | 127 (H) | >60 | 8 | 281 | 5.8 (L) | 2.2 (L) | 24.1 (HH) | 11.7 | 371 (H) | 56 (H) | 44 |
| Day 20 | 137 | 3.8 | 0.66 (L) | 106 | 21 (L) | 8.1 (L) | 25 | 125 (H) | >60 | 10 | 280 | 5.9 (L) | 2.3 (L) | 25.4 (HH) | 13.8 | 422 (H) | 63 (H) | 51 |
| Day 21 | 133 (L) | 3.5 | 0.64 (L) | 103 | 20 (L) | 8.0 (L) | 25 | 126 (H) | >60 | 10 | 272 (L) | 6.0 (L) | 2.3 (L) | 30.4 (HH) | >15 | 415 (H) | 148 (H) | 108 (H) |
| Day 22 | 131 (L) | 4.4 | 0.61 (L) | 100 | 19 (L) | 8.0 (L) | 27 (H) | 250 (H) | >60 | 12 | 276 | 6.2 (L) | 2.3 (L) | 33.1 (HH) | >15 | 588 (H) | 178 (H) | 172 (H) |
| Day 23 | 134 (L) | 3.7 | 0.72 | 103 | 22 | 8.4 | 44 (H) | 161 (H) | >60 | 9 | 283 | 6.2 (L) | 2.8 (L) | 23.7 (HH) | >15 | 618 (H) | 113 (H) | 151 (H) |
| Day 24 | 137 | 3.8 | 0.69 (L) | 108 (H) | 21 (L) | 8.5 | 31 (H) | 113 (H) | >60 | 8 | 281 | 5.5 (L) | 2.2 (L) | 15.0 (H) | >15 | 609 (H) | 129 (H) | 174 (H) |
| Day 25 | 135 (L) | 4.3 | 0.27 (L) | 106 | 19 (L) | 8.6 | 7 | 186 (H) | >60 | 10 | 273 (L) | 5.9 (L) | 2.6 (L) | 13.6 (H) | >15 | 525 (H) | 111 (H) | 184 (H) |
| Day 26 | 134 (L) | 4.1 | 0.62 (L) | 107 | 20 (L) | 8.8 | 24 | 163 (H) | >60 | 7 (L) | 276 | 5.6 (L) | 2.4 (L) | 13.3 (H) | >15 | 516 (H) | 107 (H) | 200 (H) |
| Day 27 | 137 | 3.7 | 0.60 (L) | 106 | 20 (L) | 8.4 | 28 (H) | 167 (H) | >60 | 11 | 283 | 5.6 (L) | 2.3 (L) | 15.3 (H) | >15 | 572 (H) | 174 (H) | 166 (H) |
| Day 28 | 132 (L) | 4.0 | 0.60 (L) | 104 | 18 (L) | 8.4 | 26 | 163 (H) | >60 | 10 | 273 (L) | 5.3 (L) | 2.2 (L) | 18.5 (HH) | >15 | 657 (H) | 204 (H) | 309 (H) |
| Day 29 | 131 (L) | 3.9 | 0.56 (L) | 103 | 18 (L) | 8.3 (L) | 28 (H) | 196 (H) | >60 | 10 | 274 (L) | 5.3 (L) | 2.2 (L) | 24.7 (HH) | >15 | 575 (H) | 170 (H) | 318 (H) |
| Day 30 | 130 (L) | 3.5 | 0.63 (L) | 103 | 18 (L) | 8.6 | 22 | 150 (H) | >60 | 9 | 267 (L) | 5.4 (L) | 2.2 (L) | 25.1 (HH) | > 15 | 539 (H) | 1112 (H) | 993 (H) |
| Day 31 | 131 (L) | 4.8 | 0.91 | 104 | 8 (LL) | 9.1 | 38 (H) | 200 (H) | >60 | 19 (H) | 277 | 4.8 (L) | 2.3 (L) | 30.4 (HH) | > 15 | 669 (H) | 191 (H) | 316 (H) |
| Day 32 | 132 (L) | 5.2 (H) | 1.47 (H) | 98 | 7 (LL) | 8.9 | 51 (H) | 218 (H) | 60 | 27 (H) | 285 | 4.7 (L) | 2.3 (L) | 33.1 (HH) | > 15 | 669 (H) | 191 (H) | 316 (H) |
| Day of admission | Prothrombin time (9.5-12.1 sec) | INR (0.9-1.1) | PTT (24.0-32.0 sec) | Fibrinogen (200-400 mg/dL) | D-dimer (0.00-0.50 ug/mL FEU) |
| Day 1 | 12.3 (H) | 1.2 (H) | 35.5 (H) | - | - |
| Day 2 | >90.0 (HH) | - | 29.1 | 110 (L) | 4.14 (H) |
| Day 3 | 15.9 (H) | 1.5 (H) | 45.6 (H) | 145 (L) | 14.23 (H) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Hepatobiliary Diseases and Treatments · Liver Disease and Transplantation · Amoebic Infections and Treatments
Introduction
Jaundice is a medical condition characterized by the development of yellow pigmentation of the sclera, mucous membranes, and skin due to hyperbilirubinemia [1]. Determining the underlying cause of hyperbilirubinemia can be challenging because of its wide range of etiologies, the most notable being intrahepatic and extrahepatic factors. In practice, differentiating the causes of jaundice requires a comprehensive history, physical examination, relevant laboratory tests, and diagnostic imaging. When incorporated altogether, these aid the physician in classifying jaundice into obstructive or nonobstructive subtypes [2]. Obstructive jaundice results from blocked bile ducts, preventing bile from flowing correctly from the liver to the gallbladder and digestive tract. An appropriate preoperative evaluation can significantly improve outcomes. However, in most cases, surgery for obstructive jaundice is associated with a higher incidence of complications and increased mortality rates [3]. Acute hepatic failure is an important cause of rapid-onset jaundice and altered mental status, which warrants urgent evaluation and supportive care [1]. Additionally, acute pancreatitis can contribute to extrahepatic biliary obstruction through inflammatory swelling or complications such as pseudocyst formation, highlighting the importance of appropriate cross-sectional imaging to evaluate for such obstructive etiologies [2]. We present a patient with jaundice who developed several unique complications, ultimately leading to a poor prognosis and mortality.
Case presentation
A 43-year-old male with a history of treated malaria, with military work as a private contractor in Southeast Asia, and possible exposure to unknown toxins abroad, presented with altered mental status following a seizure. He was subsequently intubated for airway protection with concerns of septic shock upon admission. He was found to be in acute renal failure, with rhabdomyolysis, acute pancreatitis, and disseminated intravascular coagulation (Tables 1-3). On physical examination, he was noted to have severe jaundice with scleral icterus. He was placed on broad-spectrum antibiotics (vancomycin and cefepime) as he underwent further testing. Computed tomography (CT) scan of the head was negative for any acute abnormalities. CT of abdomen and pelvis (A/P) did show hepatosplenomegaly, hemorrhagic ascites within the pelvis, and small hemorrhages within the bladder (Figures 1A, 1B). Lumbar puncture was conducted, which ruled out concern for meningitis. An extensive workup was completed, which included leptospirosis, tuberculosis, cryptococcal disease, tick-borne disease, hepatitis (A, B, and C), autoimmune hepatitis, ehrlichiosis, eastern equine encephalitis, Western equine encephalitis, California encephalitis, tuberculosis, malaria, dengue, HSV, John Cunningham virus, West Nile virus, CSF testing for multiple bacteria, viruses, and yeast, and a parasite panel, which were all negative. His labs continued to worsen (notably worsening leukocytosis, transaminitis, and hyperbilirubinemia) with consideration of possible initiation of continuous renal replacement therapy (CRRT); however, this was challenging as he remained on vasopressor support for treatment of shock, which was attributed to hypovolemic versus septic etiologies. His pancreatitis continued to worsen with no identifiable cause; repeat ultrasound of the abdomen did not reveal a concern for bile duct dilation (Figure 2). MRCP was suggestive of a possible hyperdense foci within the pancreas, possibly representing parenchymal hemorrhage, with a moderately distended gallbladder with sludge.
Abdomen and pelvis CT scanA: Axial section demonstrating diffuse interstitial pancreatic edema. There is also the presence of peri-hepatic ascites (a). B: Coronal section showing hemorrhage (H) in the retroperitoneum. There are also large amounts of gas surrounding the hemoperitoneum, which can be suspicious for gas gangrene (arrows). There is also a presence of abdominal ascites (a).
Ultrasound of the abdomen showing normal common bile duct (5.3 mm)
A liver biopsy by interventional radiology was completed, showing liver cirrhosis with cholestasis. Hematoxylin and eosin staining revealed ballooning degeneration of hepatocytes, with Mallory hyaline and neutrophilic steatosis (Figure 3). There were also areas of cholestasis in the liver parenchyma (Figure 4). Upon trichrome staining, the liver demonstrated bridging fibrosis (Figure 5), and on 20× magnification, the liver parenchyma showed diffuse fibrosis with ballooning degeneration (Figure 6).
Liver biopsy H&E stainingHepatic steatosis with ballooning degeneration (b), Mallory hyaline (black arrowheads), and neutrophilic satellitosis (box).
Liver parenchyma replaced with areas of canalicular cholestasis (black arrowheads)
Liver biopsy with trichrome stainingCirrhotic liver demonstrating bridging fibrosis between regenerative nodules (n).
Diffuse fibrosis within liver parenchyma with areas of ballooning degeneration (b)Portal tracts and fibrous bands contain a mixed inflammatory infiltrate.PV, portal vein
It was discovered that the patient did in fact have a history of alcohol use in the past; however, the extent of use could not be determined. Within the next several days, he became hypotensive. A repeat CT abdomen and pelvis showed acute interstitial edematous pancreatitis complicated by hemorrhage in the retroperitoneum and hemoperitoneum with large amounts of gas suspicious for gas gangrene. Surgery was consulted; however, he was deemed not a surgical candidate. Due to his poor prognosis, the family decided to proceed with withdrawal of care, and he subsequently passed.
Discussion
Acute pancreatitis is an inflammatory condition of the pancreas that can range from mild to severe, with severe cases often leading to multiorgan dysfunction syndrome (MODS) [4]. Systemic inflammatory response syndrome (SIRS) triggered by acute pancreatitis can result in widespread inflammation, leading to organ failure [5]. A study by Mofidi et al. demonstrated a strong association between early systemic inflammatory response, severity of multiorgan dysfunction, and mortality in acute pancreatitis [4]. Respiratory failure is one of the most common organ dysfunctions observed in severe acute pancreatitis, occurring in approximately 23% of cases and significantly increasing mortality risk [5]. Renal failure is another critical complication, often resulting from hypovolemia, systemic inflammation, and direct effects of pancreatic enzymes [6]. Both respiratory and renal failures significantly impact patient outcomes, with cardiovascular failure leading to the worst prognosis [6]. In this patient, the intense inflammatory cascade and cytokine-mediated microcirculatory impairment likely contributed to hepatic decompensation by worsening hepatocellular injury, cholestasis, and synthetic dysfunction [4-6].
A particularly rare and fatal complication of acute pancreatitis is gas gangrene of the pancreas, often caused by Clostridium perfringens infection. This condition is characterized by the presence of gas within the pancreatic parenchyma and surrounding retroperitoneal tissues, leading to rapid tissue necrosis and systemic toxicity [7]. A case reported by Stockinger and Corsetti described a patient with acute pancreatitis complicated by pancreatic gas gangrene, resulting in pneumoperitoneum without visceral perforation [7]. A case reported by Deręgowska-Cylke et al. highlighted the development of emphysematous pancreatitis associated with retroperitoneal gas gangrene, emphasizing the severity and rapid progression of this infection [8].
Gas gangrene is commonly associated with Clostridium species, which are known for their ability to produce gas and extensive tissue necrosis. A retrospective epidemiological study by Leal et al. demonstrated that Clostridium bacteremia, particularly involving C. perfringens, carries a high mortality rate due to its rapid progression and limited treatment options [9]. While other possible causes of gas in the retroperitoneum, such as emphysematous pancreatitis, enteric perforation, or fistulous connections, should be considered, in this case, no visceral perforation was identified on imaging, and the rapid clinical deterioration supported a diagnosis of gas gangrene [7,8]. Blood cultures in our patient did not yield Clostridium or other pathogens, and ascitic fluid was not tapped due to hemodynamic instability and coagulopathy. Therefore, based on the extensive retroperitoneal gas and hemorrhagic necrosis on imaging, gas gangrene was presumed to be secondary to a spontaneous Clostridium infection.
The management of severe acute pancreatitis complicated by infections like gas gangrene requires prompt recognition and aggressive intervention. Early fluid resuscitation, broad-spectrum antibiotics, and supportive care in an intensive care setting are critical [10]. However, the presence of gas-forming infections often necessitates surgical intervention.
Liver cirrhosis affected approximately 2.2 million adults in the United States from 2010 to 2021, with a 10% increase in mortality rate [11]. Most common causes are alcohol abuse, nonalcoholic fatty liver disease, and hepatitis C, none of which matched the history provided by our patient, except prior consumption of alcohol. Usually, patients with cirrhosis present with encephalopathy and ascites and are often diagnosed with cirrhosis through these presenting complications [11]. Further complications include spontaneous bacterial peritonitis, hepatorenal syndrome (median survival of two weeks), and hepatocellular carcinoma. Although our patient was found to have cirrhosis likely secondary to alcohol use, there were no findings of hepatocellular carcinoma on biopsy. The injury to the liver could likely have been multifactorial in the above patient, given his line of work, leading to potential toxins abroad, alcohol use, and subsequent systemic inflammatory response, further emphasizing the diagnostic complexity in the patient’s case. Potential hepatotoxin exposure in Southeast Asia includes traditional herbal remedies, aflatoxin-contaminated foods, and environmental or occupational chemicals, such as organic solvents (e.g., carbon tetrachloride and trichloroethylene), pesticides, and heavy metals like arsenic [12]. While liver biopsy can provide valuable histopathological insights, its diagnostic specificity in differentiating alcoholic hepatitis from toxin-induced liver injury remains limited. Both conditions can share overlapping features such as ballooning degeneration, Mallory-Denk bodies, neutrophilic infiltration, and varying degrees of fibrosis and cholestasis [13]. In this case, the diagnostic sensitivity of abdominal ultrasound may have been limited by factors such as operator dependency, patient body habitus, and suboptimal acoustic windows, which can reduce its ability to detect subtle biliary obstruction or small mass lesions. This is why repeat imaging with CT was performed to provide improved anatomic detail. Consequently, distinguishing between these etiologies purely on histological grounds can be challenging without a clear clinical context and corroborating history of alcohol consumption or toxin exposure, making it complex for the clinician. Management is largely targeted at the above-mentioned complications of cirrhosis with nonselective beta-blockers, spironolactone, lactulose, and paracentesis.
In the case presented, the patient’s poor surgical candidacy due to multiorgan failure limited treatment options, leading to a fatal outcome. The importance of early detection and management of complications in severe acute pancreatitis with associated multiorgan dysfunction is vital.
Conclusions
This case report highlights the complexities and challenges of diagnosing and managing severe obstructive jaundice complicated by multiple organ system failures and a rare but fatal gas gangrene of the pancreas. The patient’s history of travel, possible toxin exposure, and underlying liver cirrhosis further complicated the clinical picture. Despite extensive testing and supportive care, the patient’s condition deteriorated, leading to a poor prognosis. This case underscores the critical importance of early detection, aggressive intervention, and multidisciplinary management in patients with severe acute pancreatitis and associated multiorgan dysfunction to improve outcomes. This case also highlights the diagnostic uncertainty clinicians face in patients with overlapping hepatic and pancreatic findings, particularly when toxin exposure is unclear and lab data are nonspecific. Furthermore, it emphasizes the need for a thorough investigation of jaundice etiologies, particularly in patients with complex medical histories and risk factors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jaundice in the adult patient Am Fam Physician Roche SP Kobos R 299304692004 https://pubmed.ncbi.nlm.nih.gov/14765767/14765767 · pubmed ↗
- 2ACR Appropriateness Criteria(®) jaundice J Am Coll Radiol Hindman NM Arif-Tiwari H Kamel IR 040162019 https://pubmed.ncbi.nlm.nih.gov/31054739/10.1016/j.jacr.2019.02.01231054739 · doi ↗ · pubmed ↗
- 3Obstructive jaundice and perioperative management Acta Anaesthesiol Taiwan Wang L Yu WF 22295220142499921510.1016/j.aat.2014.03.002 · doi ↗ · pubmed ↗
- 4Association between early systemic inflammatory response, severity of multiorgan dysfunction and death in acute pancreatitis Br J Surg Mofidi R Duff MD Wigmore SJ Madhavan KK Garden OJ Parks RW 7387449320061667106210.1002/bjs.5290 · doi ↗ · pubmed ↗
- 5Organ failure associated with severe acute pancreatitis World J Gastroenterol Zhu AJ Shi JS Sun XJ 25702573920031460609910.3748/wjg.v 9.i 11.2570 PMC 4656543 · doi ↗ · pubmed ↗
- 6Early systemic inflammatory response syndrome is associated with severe acute pancreatitis Clin Gastroenterol Hepatol Singh VK Wu BU Bollen TL Repas K Maurer R Mortele KJ Banks PA 12471251720091968686910.1016/j.cgh.2009.08.012 · doi ↗ · pubmed ↗
- 7Pneumoperitoneum from gas gangrene of the pancreas: three unusual findings in a single case J Gastrointest Surg Stockinger ZT Corsetti RL 489492820041512037510.1016/j.gassur.2003.11.002 · doi ↗ · pubmed ↗
- 8A deceptive case of emphysematous cholecystitis complicated with retroperitoneal gangrene and emphysematous pancreatitis: clinical and computed tomography features Pol J Radiol Deręgowska-Cylke M Palczewski P Pacholczyk M Jonas M Cylke R Kosieradzki M Gołębiowski M 0584201910.5114/pjr.2019.82858 PMC 647914631019593 · doi ↗ · pubmed ↗