A Comparative Study of the Effect of Anxiety, Stress and Poor Sleep on Multipara and Nullipara Pregnant Women
Pragati Divedi, Deepti Dwivedi, Nimarpreet Kaur, Pragyashaa Chaudhary, Sunil Chamola

TL;DR
This study compares how sleep deprivation affects stress and anxiety in pregnant women who have had previous pregnancies versus those who are pregnant for the first time.
Contribution
The study provides new insights into the differences in sleep health and psychological outcomes between multipara and nullipara pregnant women.
Findings
Poor sleep was more common in nullipara women compared to multipara women.
Stress and anxiety were strongly correlated with poor sleep quality in pregnant women.
Multipara women showed better coping strategies due to prior pregnancy experience.
Abstract
Introduction: Sleep is an essential component of well-being. It is defined as a reversible behavioral state of perception disengagement from unresponsiveness to the environment. Sleep deprivation leads to stress, leading to mental issues like mood disorders and depression. This study has a prime focus on how the psychological parameters, like anxiety and stress, are affected by sleep deprivation during pregnancy and differentiates these in nullipara and multipara women. Aim and objectives: The aim of this study was to study the effect of sleep health on the psychological health of pregnant women. The objectives were (i) to assess the quality of sleep in pregnant women by using the Pittsburgh Sleep Quality Index (PSQI 21 items), (ii) to compare the quality of sleep in multipara and nullipara pregnant women by using the Pittsburgh Sleep Quality Index (PSQI), (iii) to compare the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
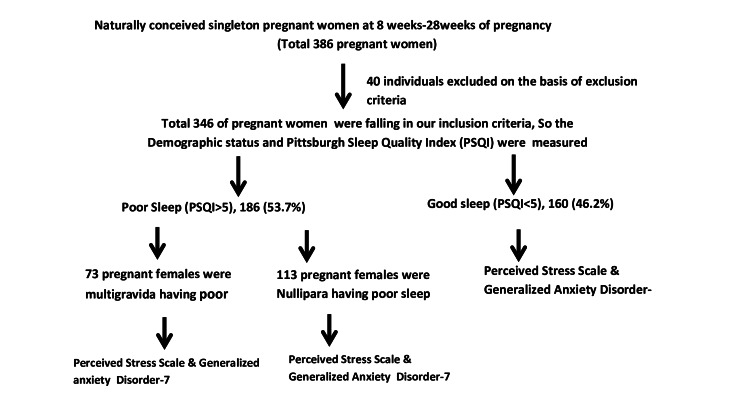 Figure 1
Figure 1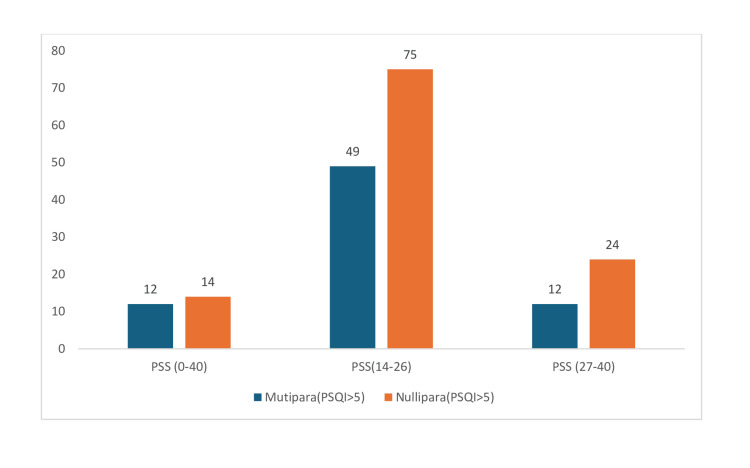 Figure 2
Figure 2| Parameters | N (%) | |
| Age | 25-30 years | 138 |
| >30 years | 208 | |
| Global PSQI score (>5) | <30 years | 117 |
| >30 years | 69 | |
| Global PSQI score (<5) | <30 years | 21 |
| >30 years | 139 | |
| Parity | Nulliparous | 200 |
| Multiparous | 146 | |
| Marital status | Married | 344 |
| Single | 2 | |
| Gestational age | 1st Trimester | 80 |
| 2nd Trimester | 214 | |
| 3rd Trimester | 52 | |
| Socioeconomic status | Lower class | 93 |
| Middle class | 211 | |
| Upper class | 42 |
| Perceived stress score (0-40) | Poor sleep quality (PSQI score>5) 186 (53.75%) | Good sleep quality (PSQI score<5) 160 (46.25%) | ||
| Multipara women (73; 39.24%) | Nullipara women (113; 60.75%) | Multipara women (86; 53.75%) | Nullipara women (74; 46.25%) | |
| Mild stress (Score 0-13) | 12 (16.44%) | 14 (12.38%) | 33 (38.37%) | 43 (58.10%) |
| Moderate stress (Score 14-26) | 49 (67.12%) | 75 (66.38%) | 29 (33.72%) | 23 (31.08%) |
| Severe stress (Score 27-40) | 12 16.44%) | 24 (21.24%) | 24 (27.90%) | 8 (10.81%) |
| Generalized anxiety disorder 7 (0-21) | Poor sleep quality (PSQI score>5) (186 women) | Good sleep quality (PSQI score<5) (160 women) | ||
| Multipara women (73) | Nullipara women (113) | Multipara women (86) | Nullipara women (74) | |
| Minimal anxiety (Score 0- 4) | 5 | 15 | 13 | 6 |
| Mild anxiety (Score 5-9) | 13 | 8 | 29 | 23 |
| Moderate anxiety (Score 10-14) | 38 | 68 | 24 | 36 |
| Severe anxiety (Score >15) | 17 | 22 | 20 | 9 |
| Psychological assessment scale | Poor quality sleep | t-value | p-value | |
| Multipara N1=73 (39.24%) | Nullipara N2=113 (60.75%) | |||
| Perceived stress scale score | 10.73±3.65 | 21.03±4.90 | 15.40 | <0.0001 |
| Generalized Anxiety Disorder scale Score | 7.87± 3.21 | 12.31±1.36 | 13.02 | <0.0001 |
| PSQI and PSS r-value | 0.53 | |||
| PSQI and GAD r-value | 0.57 | |||
| First trimester (80 women; 23.13%) | Second trimester (214 women; 61.84%) | Third trimester (52 women; 15.03%) | ||||
| Poor sleep quality (PSQI>5) 58 | Good sleep quality (PSQI<5) 22 | Poor sleep quality (PSQI>5) 102 | Good sleep quality (PSQI<5) 112 | Poor sleep quality (PSQI>5) 34 | Good sleep quality (PSQI<5) 20 | |
| Stress (PSS ≥ 14) | 31 | 5 | 49 | 27 | 21 | 8 |
| Anxiety (GAD-7 ≥10) | 36 | 9 | 53 | 32 | 24 | 9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Sleep and related disorders · Breastfeeding Practices and Influences
Introduction
Sleep is a key component of health. It has an essential role in various reparative processes of the body, along with the removal of toxins, release of hormones, and memory consolidation [1,2]. Hormonal changes affect the psychological health of women including impaired sleep quality in women. During pregnancy, the hypothalamo-pituitary-adrenal (HPA) axis has reduced stress responsiveness along with the anti-inflammatory profile of the immune system [3]. Maternal stress stimulates the downregulated HPA axis and inflammatory responses during pregnancy, resulting in maternal illness during pregnancy. This increases behavioral changes and disordered sleep [4].
Sleep insufficiency has been linked to the leptin hormone of adipose tissue, responsible for appetite suppression and increased concentration of ghrelin hormone, which stimulates the appetite. Adults with chronic sleep loss report excess mental distress, depressive symptoms, anxiety, and alcohol use [5].
Pregnancy is different for the same woman, and the consequences of various physiological changes even vary within each trimester of the same pregnancy, which has a huge impact on the sleep quality and psychological health of pregnant women.
This study was planned to provide valuable insights into the influence of sleep quality on the psychological state during pregnancy. This study has a primary focus on how the psychological parameters like anxiety and stress are affected by sleep health during pregnancy and differentiates these in nullipara and multipara pregnancies. The mental health of women during pregnancy has been discussed for a long time, but how it is different in women with multipara and nullipara pregnancies affected by sleep deprivation is analyzed in this study.
Materials and methods
This cross-sectional study was done on 386 naturally conceived singleton literate pregnant women at eight weeks to 28 weeks of pregnancy who visited FMHS SGT Hospital Obstetrics & Gynecology Department and gave consent during the study period. Naturally conceived singleton literate pregnant women at 8-28 weeks of pregnancy of age 18-41 years participated in this study. The duration of the study was six months, i.e., July 2024 to December 2024. Forty pregnant women were excluded. They were those with any history of medical and psychiatric illnesses (medical and psychological), history of pregnancy loss, drugs, alcohol, and hormonal therapy, and unpredictable conditions such as travelling to different time zones and night shift workers.
The study was done by using widely used and validated tools shown in Figure 1.
Study design
The study tool was divided into four different sections: (i) Demographic status (eight items), (ii) Perceived stress score (10 items) [6], (iii) Pittsburgh Sleep Quality Index (PSQI 21 items) [7], and (iv) Generalized Anxiety Disorder (seven items) [8]. Descriptive statistics and Pearson correlation test were applied using IBM SPSS Statistics for Windows, Version 26 (Released 2019; IBM Corp., Armonk, New York, United States).
Pittsburgh Sleep Quality Index (PSQI)
The sleep quality was measured by using this scale system. It is a free validated questionnaire categorized into seven components: sleep quality, latency, duration, efficiency, sleep disturbances, use of medications, and daytime dysfunction. It contains 21 questions. The global score of PSQI ranges between 0 and 21. A score less than 5 indicates good sleep quality, ‘0’ indicates no difficulty, and a total score greater than 5 indicates poor sleep quality. The scale has been widely used in various studies with high reliability and validity and the Cronbach’s alpha of this index is 0.811.
Perceived Stress Scale (PSS)
This is the most widely used scale to measure perceived stress. Each question is scored from 0 (never) to 4 (very often), with a total possible score range of 0 to 40. The higher score interprets a higher degree of stress: Scores ranging from 0 to 13 are considered as low stress; scores ranging from 14 to 26 are considered as moderate stress; scores ranging from 27 to 40 are considered as high perceived stress
Generalized Anxiety Disorder-7 (GAD-7)
The GAD-7 is a seven-item self-report scale developed to assess the defining symptoms of anxiety. The various items are graded on a 4-point Likert-type scale (0=not at all to 3=nearly every day). Scores range from 0 to 21, with higher scores indicating more severe GAD symptoms.
Results
The study results show that out of 346 women, 200 were nulliparous, and 146 (42.2%) were multiparous. Among 346 women, 186 (53.76%) had poor sleep with a mean ± SD of 6.28 ± 2.56, out of which 73 were multipara and 113 pregnancies were nullipara.
Table 1 shows that the majority of the population falls in the >30 years age group, comprising 208 individuals, while a smaller portion is in the 25-30 years age group, making up 138. Nulliparous represents the majority, with 200 women, while multiparous makes up a smaller group of 146 women. The majority of women were married (344 women), while a very small proportion (two women) were single. Most participants were in the second trimester, accounting for 214 women. The first-trimester group had 80 pregnant women, while the third-trimester group had 52 pregnant women. The majority of the sample belongs to the middle class, comprising 211 women. Lower-class women were 93, while a smaller group was in the upper class (42 women).
Table 2 and Figure 2 show that pregnant women with poor sleep quality were 186 while 160 women had good sleep quality. A small proportion of women with poor sleep quality reported mild stress. This is observed in both multipara (12; 16.44%) and nullipara (14; 12.38%) women, while a significantly higher proportion of women with good sleep quality experienced mild stress, particularly nullipara women (43; 58.10%), followed by multipara women (33; 38.37%).
Comparison of the perceived stress level and PSQI score of multipara and nullipara women with poor sleep qualityPSQI: Pittsburgh Sleep Quality Index; PSS: Perceived Stress Scale
A significant majority of women with poor sleep quality experienced moderate stress. Among multipara women, 49 (67.12%) reported moderate stress, while 75 (66.38%) nullipara women also reported moderate stress. Moderate stress is less common among those with good sleep quality compared to poor sleep quality. Only 29 (33.72%) multipara women and 23 (31.08%) nullipara women with good sleep quality reported moderate stress. A smaller proportion of women with poor sleep quality experienced severe stress. Twelve (16.44%) multipara women and 24 (21.24%) nullipara women with poor sleep quality reported severe stress. A higher proportion of multipara women with good sleep quality experienced severe stress 24 (27.90%) compared to nullipara women with good sleep quality 8(10.81%). The chi-square value is 75.32 with a p-value less than 0.001, which explains that there is an association between sleep pattern and stress.
Table 3 shows that among women with poor sleep quality, minimal anxiety (Score 0-4) was reported by a small percentage (five (2.69%) multipara women and 15 (8.06%) nullipara women). Mild anxiety (score 5-9) was reported by 13 (6.98%) multipara women and eight (4.30%) nullipara women. Moderate anxiety (score 10-14) was significantly higher among women with poor sleep quality, with 38 (20.43%) multipara women and 68 (36.56%) nullipara women reporting moderate anxiety. Severe anxiety (Score >15) was reported by 17 (9.14%) multipara women and 22 (11.83%) nullipara women. Among women with good sleep quality, minimal anxiety (Score 0-4) was reported by 13 (8.13%) multipara women and six (3.75%) nullipara women, mild anxiety (Score 5-9) was reported by 29 (18.12%) multipara women and 23 (14.37%) nullipara women, moderate anxiety (Score 10-14) was reported by 24 (15.00%) multipara women and 36 (22.50%) nullipara women, and severe anxiety (Score >15) was reported by 20 (12.5%) multipara women and nine (5.63%) nullipara women.
Table 4 shows that the Mean±SD perceived stress score for multipara women with poor sleep quality is 10.73 ± 3.65, while in nullipara women, the Mean±SD perceived stress score with poor sleep quality was 21.03 ± 4.90. This indicates a statistically significant difference between the two groups. The Mean±SD generalized anxiety disorder scale score for multipara women with poor sleep quality is 7.87 ± 3.21, and the Mean±SD generalized anxiety disorder scale score for nullipara women with poor sleep quality is 12.31 ± 1.36. The p-value is <0.0001, which shows a highly statistically significant difference between the two groups.
Table 5 shows that out of 80 pregnant women in the first trimester, 58 (23.13%) had poor sleep quality among which 31 (53.45%) were in moderate to high level of stress (PSS≥14), and 36 (62.07%) had moderate to high anxiety with (GAD-7 ≥ 10). Similarly, out of 214 pregnant women in the second trimester, 102 (47.67%) had poor sleep quality among which 31 (53.45%) were in moderate to high level of stress (PSS≥14), and 49 (48.04%) had moderate to high anxiety with (GAD-7≥ 10). Among 52 pregnant women in the third trimester, 34 (65.38%) had poor sleep quality, among which 21 (61.76%) were in a moderate to high level of stress (PSS≥14), and 24 (70.59%) had moderate to high anxiety with (GAD-7≥ 10).
Discussion
The study conducted by Kiper et al. showed that sleep quality is better in younger pregnant women. This finding differed from the present study, where 117(62.98%) women aged less than 30 years had poor quality sleep [9]. The 214 (60.98%) women were from the middle socioeconomic status, out of which 98 (45.80%) had poor sleep. The previous conducted study explains our results by the fact that, as previously suggested in the literature, normally, education and socioeconomic status are likely to result in good mental health [10-12]. Our study results show that women during pregnancy have poor quality of sleep. The percentage of poor quality sleep was further more in nulliparous (186; 53.76%) women than in multiparous women (73; 39.24%). This finding is in concordance with the study conducted in Taiwan & Iran [13,14]. Although a Vietnamese study conducted on 119 healthy pregnancies reported contradictory results [15].
The findings of the present study suggested that there was a statistically highly significant difference in stress level between multipara (10.73±3.65) and nullipara women (21.03±4.90). The possible reason could be that multipara women have better coping strategies as they have previous pregnancy experience. Further, the stress levels of the moderate to severe category with poor sleep quality were positively associated with perceived stress score, and a correlation of 0.53 was present between them. This finding is concordant with the previously done study on the Chinese population by Gao [16].
The FinnBrain birth cohort study conducted on 78 healthy pregnant women shows deterioration in sleep quality across the pregnancy, along with depressive & anxiety-related symptoms. These results were similar to the present study, where out of 186 poor sleep quality, 145 (77.96%) had moderate to severe levels of generalized anxiety score. Among these, 55 (29.57%) were multipara and 90 (48.39%) were nullipara [17,18].
Further, we can elaborate on the linkage between anxiety and obstetric history on the basis of our results, as the generalized anxiety disorder score was statistically highly significant for multipara (7.87±3.21) and nullipara (12.31±1.36). The possible reason for this could be that nullipara women have less fear of the outcome of pregnancy in comparison to multipara women in the Indian population. These results correspond with the findings of a study done on pregnant women in the Netherlands who reported more episodes of anxiety symptoms in multiparity, with severe nausea and extreme fatigue [19,20].
The study conducted on 148 pregnant women determined that the stress level of pregnant women was high in all three trimesters, and the worst sleep quality and stress were reported in the third trimester. These findings were in accordance with the present study finding where among the poor sleep quality pregnant women, 31 (53.45%) women in the first trimester, 49 (48.04%) women in the second trimester and 24 (70.59%) women in the third trimester were suffering from moderate to high level of stress and stress worsened in third-trimester women. Thus the sleep quality decreases as the pregnancy stress increases and worsens in the third trimester of pregnancy [21,22].
The pattern of anxiety was also following a similar trend, as in the first trimester, 36(62.07%), second trimester, 53(51.96%), and in the third trimester, 24 (70.59%) pregnant women had poor sleep quality. The anxiety score increases in women in their third trimester, with the deterioration in sleep quality. Further, various previous research studies have documented that maternal anxiety sleep quality, and life stress have a strong association [23,24]. However, this is in contrast to the study published with the 630 pregnant women from Spain by Pascal et al. They had different results stating that anxiety and depressive symptoms do not have a homogeneous trend. They found a low correlation between sleep quality and stress and anxiety [25].
The authors recognize that there were a few areas, like a single-center study, and single point of contact, and a short duration of study were major limitations. Due to the uniformity of the rural population, the analysis was not powered to control for multiple potential confounders. However, we did not control for age, but the maximum responders were in the younger age group.
Conclusions
Increased levels of stress and anxiety had a vicious direct effect related to the poor quality of sleep by acting on HPA axis activity. Poor sleep health is an important indicator of the mental health of women during pregnancy. Multiparous women have better coping strategies than nulliparous women as they have more experience from their previous pregnancies. The future scope of study includes observing the relationship between pregnancy outcome and sleep and psychological health. The psychological screening and sleep health assessment during pregnancy should be an essential component of the antenatal checkups. The antenatal visits of pregnant women with the assessment of psychological health and sleep health could be a very important method to prevent the adverse effects of pregnancy outcomes induced by them. Sleep health education and maintenance of good sleep hygiene will have a positive impact on psychological health during pregnancy. The outcome of this study envisages attention to sleep health and psychological health during pregnancy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Unraveling why we sleep: quantitative analysis reveals abrupt transition from neural reorganization to repair in early development Sci Adv Cao J Herman AB West GB Poe G Savage VM 6202010.1126/sciadv.aba 0398 PMC 750092532948580 · doi ↗ · pubmed ↗
- 2Effects of poor and short sleep on glucose metabolism and obesity risk Nat Rev Endocrinol Spiegel K Tasali E Leproult R Van Cauter E 253261520091944425810.1038/nrendo.2009.23PMC 4457292 · doi ↗ · pubmed ↗
- 3Immunology of pregnancy Proc Nutr Soc Thornton CA 3573656920102057620510.1017/S 0029665110001886 · doi ↗ · pubmed ↗
- 4Effects of prenatal stress on pregnancy and human development: mechanisms and pathways Obstet Med Coussons-Read ME 5257620132775715710.1177/1753495 X 12473751 PMC 5052760 · doi ↗ · pubmed ↗
- 5Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index P Lo S Med Taheri S Lin L Austin D Young T Mignot E 01200410.1371/journal.pmed.0010062 PMC 53570115602591 · doi ↗ · pubmed ↗
- 6A global measure of perceived stress J Health Soc Behav Cohen S Kamarck T Mermelstein R 3853962419836668417 · pubmed ↗
- 7Pittsburgh Sleep Quality Index (PSQI) responses are modulated by total sleep time and wake after sleep onset in healthy older adults P Lo S One Zitser J Allen IE Falgàs N Le MM Neylan TC Kramer JH Walsh CM 017202210.1371/journal.pone.0270095 PMC 923215435749529 · doi ↗ · pubmed ↗
- 8A brief measure for assessing generalized anxiety disorder: the GAD-7Arch Intern Med Spitzer RL Kroenke K Williams JB Löwe B 1092109716620061671717110.1001/archinte.166.10.1092 · doi ↗ · pubmed ↗