A late presentation of benign cephalic histiocytosis
Madison A. Hackley, Nicholas D. Brownstone, Shayan Waseh, Simo Huang, Jason B. Lee, Sylvia Hsu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1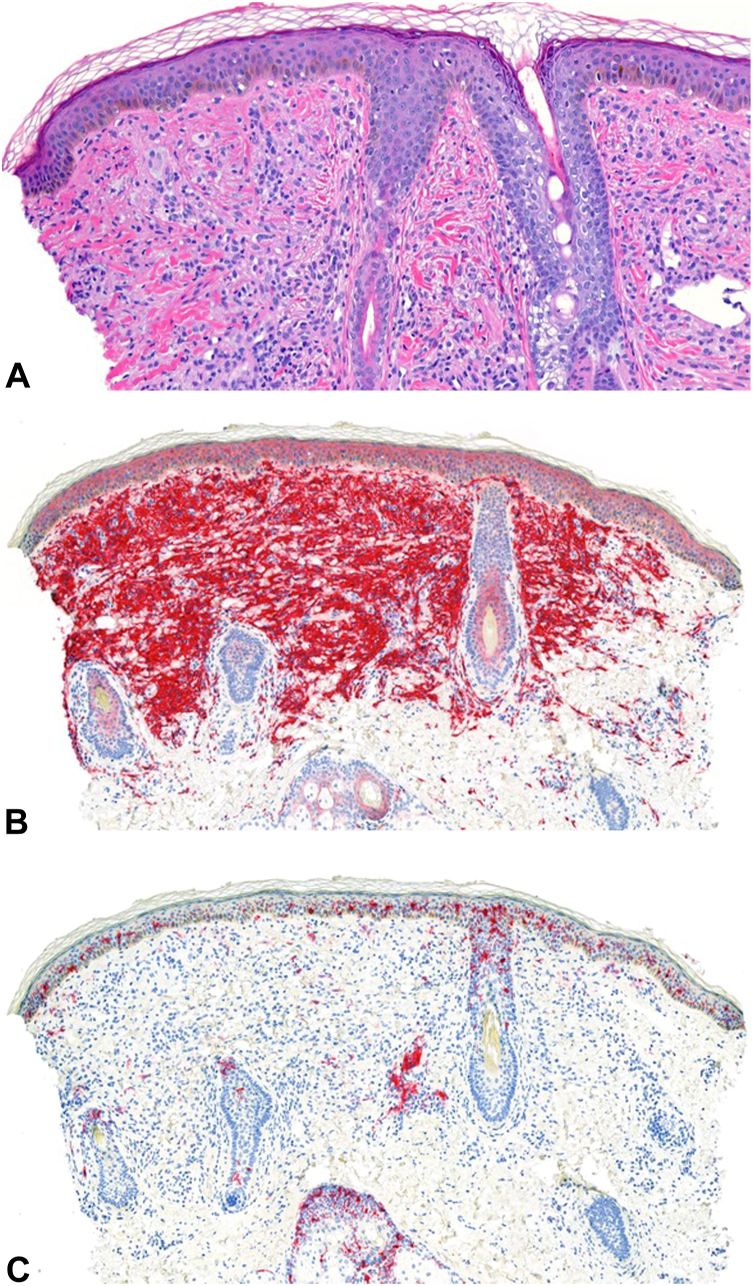 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHistiocytic Disorders and Treatments · Genetic and rare skin diseases. · Tumors and Oncological Cases
Case report
A 5-year-old girl presented to the dermatology clinic with numerous hyperpigmented macules on the bilateral cheeks (Fig 1). According to the patient’s mother, the macules had spontaneously appeared 6 months prior to the patient’s presentation to the clinic. The macules were not painful or pruritic. The patient’s past medical history was noncontributory. On examination, there were multiple 1-mm, round, well-demarcated, light brown macules on the bilateral cheeks. A few lesions exhibited the morphology of papules. A punch biopsy was performed and demonstrated a prominent histiocytic infiltrate with foci of foamy cells in the superficial dermis (Fig 2, A), highlighted by CD163 (Fig 2, B) and CD68 stains. A CD1a stain failed to highlight the cells (Fig 2, C). The combination of these dermatopathology findings with the clinical presentation was consistent with a diagnosis of benign cephalic histiocytosis (BCH).Fig 1. Multiple, light-brown pigmented macules and papules on the left cheek. Similar lesions were present on the right cheek.Fig 2. Benign cephalic histiocytosis. There are oval-to-round pale histiocytes, some of them with foamy cytoplasm, throughout the dermis accompanied by perivascular lymphocytes (A, H&E 200×). CD163 stain highlights a dense infiltrate of histiocytes within the superficial dermis (B, 100×). CD1a stain, a specific marker for Langerhans cells, fails to highlight the lesion (C, 100×).
Introduction
Benign cephalic histiocytosis (BCH) is a subtype of non-Langerhans cell histiocytosis that occurs in young children. BCH has an average age onset of 15 months, although a recently published case series found the average age of presentation to occur before 6 months of age.1^,^2 BCH typically presents as multiple small, asymmetric, and asymptomatic, yellow-brown macules, predominantly on the face and neck.1^,^2 The pathogenesis of BCH is still largely unknown.3 The diagnosis of BCH is usually clinical, although histopathology usually shows a histiocytic infiltrate in the superficial dermis. Immunohistochemical staining of BCH lesions is positive for factor XIIIa, CD163, and CD68, but negative for CD1a, langerin, and S100.1^,^3
Discussion
Without confirmatory biopsy results, BCH may be easily misdiagnosed as other non-Langerhans cell subtypes.3 Both BCH and juvenile xanthogranuloma share similar immunohistologic markers: CD68, CD163, and Factor XIIIa.3 Other forms of non-Langerhans cell histiocytosis are less prone to spontaneous regression in comparison to BCH.3 Differentiating between the subtypes can help guide clinical decision-making about treatment.
The prognosis of BCH is very favorable. BCH is self-limiting, and the lesions spontaneously regress over a period of months to years.1^,^2 Some cases of BCH can be characterized by periods of exacerbation or escalation to generalized eruptive histiocytosis.3 Treatment of the lesions is not necessary. Recent literature has reported the successful treatment of BCH with rapamycin in a handful of pediatric cases.4^,^5 However, regression of lesions resulted in mild scarring in a small portion of reported BCH cases.1^,^4 Cosmetic correction of residual scarring can be considered on an individual basis.
Non-Langerhans cell histiocytosis subtypes, including BCH, have been associated with diseases such as diabetes insipidus and insulin-dependent diabetes mellitus.6^,^7 However, these associations are exceedingly rare, and there are no serious systemic complications or comorbidities linked to BCH.8 Therefore, no further workup was needed for our asymptomatic patient.
BCH is an exceedingly rare diagnosis, with only 60 cases reported in the literature.2 Differentiation between BCH and other non-Langerhans cell manifestations that are less prone to spontaneous regression, such as progressive mucinous familial histiocytosis and xanthoma disseminatum, is important.3 Additionally, it is crucial to recognize that BCH can manifest as late as the fifth or sixth year of life, as in our patient. Accurate diagnosis of BCH in pediatric populations requires the use of both clinical findings and immunohistological markers. This case report highlights an underrepresented, late presentation of this rare and underdiagnosed dermatologic entity.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mathes E.Lalor L.Skin Lesion in the Newborn and Infant. Post TW, ed. Up To Date. Waltham, MA: Up To Date Inchttp://www.uptodate.com
- 2Polat Ekinci A.Buyukbabani N.Baykal C.Novel clinical observations on benign cephalic histiocytosis in a large series Pediatr Dermatol 344201739239710.1111/pde.1315328466548 · doi ↗ · pubmed ↗
- 3Fraitag S.Emile J.F.Cutaneous histiocytoses in children Histopathology 801202219621510.1111/his.1456934958507 · doi ↗ · pubmed ↗
- 4Effendi R.M.R.A.Rizqandaru T.Yuliasari R.Gondokaryono S.P.Diana I.A.Dwiyana R.F.Successful treatment of non-Langerhans cell histiocytosis with topical rapamycin in two pediatric cases Clin Cosmet Investig Dermatol 1520221575158210.2147/CCID.S 375995 PMC 936501335967913 · doi ↗ · pubmed ↗
- 5Habeshian K.Silverman R.A.De Klotz C.M.C.Treatment of benign cephalic histiocytosis with topical 1% rapamycin ointment Pediatr Dermatol 363201941141310.1111/pde.1380030907021 · doi ↗ · pubmed ↗
- 6Saez-De-Ocariz M.Lopez-Corella E.Duran-Mc Kinster C.Orozco-Covarrubias L.Ruiz-Maldonado R.Benign cephalic histiocytosis preceding the development of insulin-dependent diabetes mellitus Pediatr Dermatol 231200610110210.1111/j.1525-1470.2006.00187.x 16445430 · doi ↗ · pubmed ↗
- 7Weston W.L.Travers S.H.Mierau G.W.Heasley D.Fitzpatrick J.Benign cephalic histiocytosis with diabetes insipidus Pediatr Dermatol 174200029629810.1046/j.1525-1470.2000.01779.x 10990580 · doi ↗ · pubmed ↗
- 8Patsatsi A.Kyriakou A.Sotiriadis D.Benign cephalic histiocytosis: case report and review of the literature Pediatr Dermatol 315201454755010.1111/pde.1213523551579 · doi ↗ · pubmed ↗