A patient with periumbilical hyperpigmentation and keratotic papules
Mallory Hedden, Katelyn Dugan, Emily H. Smith, Alexander B. Aria

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1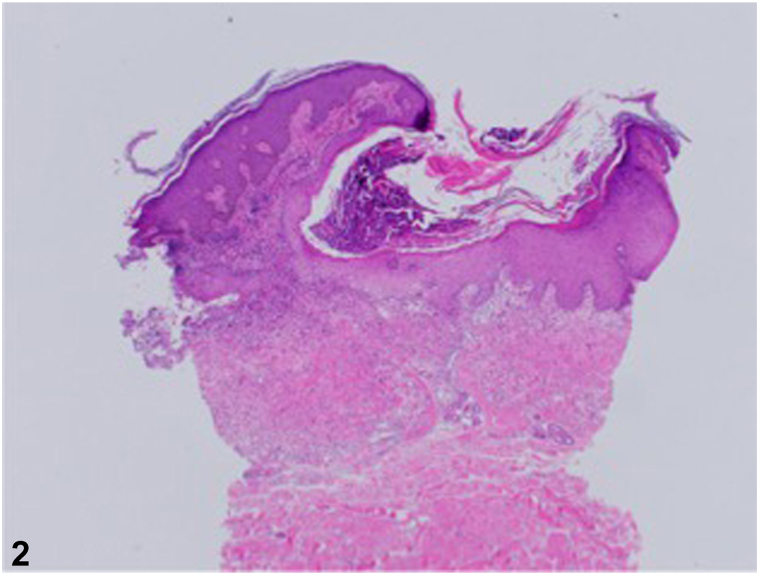 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatological and Skeletal Disorders · Vascular Tumors and Angiosarcomas · Autoimmune and Inflammatory Disorders
Clinical images
History
A 60-year-old multiparous African American female with a past medical history of hypertension, systemic lupus erythematosus, fibromyalgia, and osteoarthritis presented with a 3-year history of an abdominal rash. Associated symptoms included tenderness and worsening of the rash with friction. The patient had previously tried clobetasol 0.05% cream without improvement. She denied a family history of a similar abdominal rash. Examination revealed well-demarcated hyperpigmented plaques with admixed focal keratotic papules and surrounding erythema in a periumbilical distribution (Fig 1). Two punch biopsies were obtained from the right and inferior periumbilical abdomen. Hematoxylin and eosin staining showed short, curled, distorted collections of basophilic elastic fibers throughout the reticular dermis that extrude through a hyperplastic epidermis (Fig 2).Fig 1Perforating calcific elastosis. Well-demarcated hyperpigmented plaques with admixed focal keratotic papules and surrounding erythema in a periumbilical distribution.Fig 2Hematoxylin and eosin stain demonstrating perforating calcific elastosis. Punch biopsy from the patient’s periumbilical region demonstrating short, curled, distorted collections of basophilic elastic fibers throughout the reticular dermis and extruding through a hyperplastic epidermis.
Question: What is the most likely diagnosis?
- **A.**Perforating calcific elastosis
- **B.**Localized hereditary pseudoxanthoma elasticum
- **C.**Elastosis perforans serpiginosa
- **D.**Calcinosis cutis
- **E.**Reactive perforating collagenosis
Answers:
- **A.**Perforating calcific elastosis—Correct. Perforating calcific elastosis, also known as periumbilical perforating pseudoxanthoma elasticum (PPPXE), is the most likely diagnosis in this middle-aged, multiparous patient given the clinical and histopathologic findings. Perforating calcific elastosis is an acquired perforating disorder caused by repetitive trauma that leads to degeneration and calcification of elastic fibers.
- **B.**Localized hereditary pseudoxanthoma elasticum – Incorrect. Hereditary PXE is unlikely given this patient’s age of onset, absence of lesions on the flexural folds, lack of cardiovascular and ophthalmic involvement, and absence of family history of a similar rash.1
- **C.**Elastosis perforans serpiginosa (EPS) – Incorrect. EPS can be differentiated from perforating PXE histologically by the presence of transepidermal elimination of unmineralized elastic fibers. EPS also primarily affects males and typically occurs in patients before age 30.1^,^2
- **D.**Calcinosis cutis – Incorrect. Calcinosis cutis is characterized by dermal and subcutaneous nodules. Additionally, all connective tissue fibers are calcified in calcinosis cutis, while only the elastic fibers are calcified in perforating calcific elastosis.1
- **E.**Reactive perforating collagenosis – Incorrect. Although RPC also presents with hyperkeratotic papules, it is characterized by transepithelial elimination of altered collagen, rather than elastic fibers, and is unlikely in this patient without a history of diabetes or renal disease.3
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lewis K.G.Bercovitch L.Dill S.W.Robinson-Bostom L.Acquired disorders of elastic tissue: Part I. Increased elastic tissue and solar elastotic syndromes J Am Acad Dermatol 511200412110.1016/j.jaad.2004.03.01315243519 · doi ↗ · pubmed ↗
- 2Hosen M.J.Lamoen A.De Paepe A.Vanakker O.M.Histopathology of pseudoxanthoma elasticum and related disorders: histological hallmarks and diagnostic clues Scientifica 2012201211510.6064/2012/598262 PMC 382055324278718 · doi ↗ · pubmed ↗
- 3Faver I.R.Daoud M.S.Su W.P.Acquired reactive perforating collagenosis J Am Acad Dermatol 304199457558010.1016/S 0190-9622(94)70065-68157784 · doi ↗ · pubmed ↗