Association of Aortic Root and Valve Morphology With De Novo Aortic Valve Regurgitation After Implantation of Left Ventricular Assist Device
Takashi Murakami, Yusuke Misumi, Daisuke Yoshioka, Takuji Kawamura, Ai Kawamura, Shin Yajima, Shunsuke Saito, Takashi Yamauchi, Shigeru Miyagawa

TL;DR
This study finds that a specific aortic root measurement before LVAD implantation is linked to new aortic valve regurgitation after surgery.
Contribution
Identifies a novel preoperative morphological risk factor for post-LVAD aortic valve regurgitation.
Findings
Patients with higher VBD/GH ratios had significantly more postoperative aortic regurgitation.
A VBD/GH ratio above 1.6 may indicate higher risk for new aortic valve insufficiency after LVAD implantation.
Abstract
The development of aortic valve regurgitation (AR) negatively affects the survival of patients with continuous‐flow left ventricular assist device (LVAD) support. Although several risk factors have been identified, little is known about the effect of preoperative aortic root and valve morphology on the development of de novo AR after LVAD implantation. Between April 2018 and September 2023, 87 patients underwent durable LVAD implantation at our department. Of these, the 15 eligible patients who underwent preoperative electrocardiography‐synchronized cardiac contrast‐enhanced computed tomography were included in this study. Baseline aortic root and valve morphology and its relationship with the postoperative development of AR were retrospectively reviewed. The mean duration of LVAD support was 1208 ± 618 days. At 60 months postsurgery, 10 patients had mild or greater AR (Group I) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
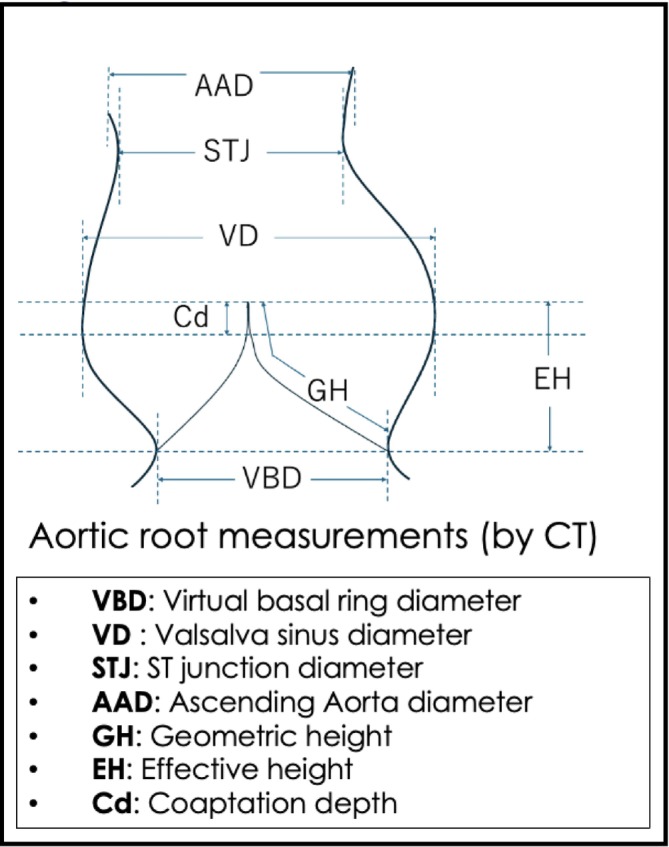 FIGURE 1
FIGURE 1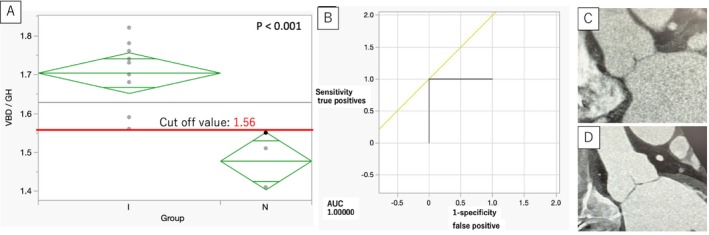 FIGURE 2
FIGURE 2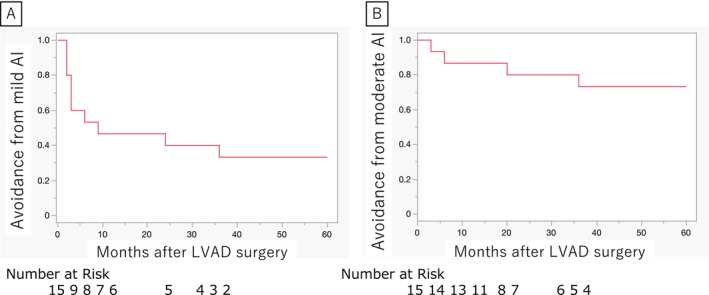 FIGURE 3
FIGURE 3| Preoperative | All ( | Group I ( | Group N ( |
|
|---|---|---|---|---|
| Patient characteristic | ||||
| Age | 51.8 ± 13.3 | 51.9 ± 4.4 | 51.6 ± 6.2 | 0,97 |
| Sex | 11 (73.3%) | 8 (80%) | 3 (60%) | 0,56 |
| BSA (m2) | 1.65 ± 0.19 | 1.64 ± 0.06 | 1.66 ± 0.09 | 0,86 |
| Nonischemic cardiomyopathy | 13 (86.7%) | 8 (80%) | 5 (100%) | 0,52 |
| Previous cardiovascular surgery | 7 (46.7%) | 5 (50%) | 2 (40%) | 1 |
| Hypertension | 2 (13.3%) | 1 (10%) | 1 (20%) | 1 |
| Dyslipidemia | 3 (20%) | 1 (10%) | 2 (40%) | 0,24 |
| Diabates mellites | 3 (20%) | 2 (20%) | 1 (20%) | 1 |
| COPD | 0 (0%) | 0 (0%) | 0 (0%) | ー |
| Peripheral vascular disease | 1 (6.7%) | 1 (10%) | 0 (0%) | 1 |
| CVA | 1 (6.7%) | 1 (10%) | 0 (0%) | 1 |
| Hemoglobin (g/dl) | 13.3 ± 2.27 | 12.8 ± 0.70 | 14.4 ± 0.99 | 0,21 |
| White blood cell (/dl) | 6203 ± 1800 | 6769 ± 524 | 5072 ± 742 | 0,084 |
| LDH | 211.6 ± 57.2 | 222.5 ± 18.0 | 189.8 ± 25.5 | 0,31 |
| AST | 24.3 ± 6.85 | 22.4 ± 2.0 | 28.2 ± 2.9 | 0,13 |
| ALT | 25.5 ± 14.7 | 22.6 ± 4.6 | 31.2 ± 6.5 | 0,3 |
| T‐Bil | 0.77 ± 0.32 | 0.88 ± 0.09 | 0.56 ± 0.13 | 0,069 |
| Albumin | 3.93 ± 0.41 | 3.78 ± 0.12 | 4.22 ± 0.16 | 0,046 |
| Creatinine | 1.01 ± 0.24 | 1.06 ± 0.074 | 0.898 ± 0.106 | 0,23 |
| BNP | 473.2 ± 332.7 | 485.0 ± 109.0 | 449.8 ± 154.2 | 0,86 |
| TTE | ||||
| LVDd (mm) | 67.5 ± 9.05 | 68.6 ± 2.93 | 65.4 ± 4.14 | 0,5388 |
| LVDs (mm) | 62.1 ± 9.40 | 63.4 ± 3.02 | 59.6 ± 4.27 | 0,4808 |
| LVEF (%) | 20.5 ± 7.88 | 20.1 ± 2.58 | 21.4 ± 3.65 | 0,7756 |
| Trivial AI | 6 (40%) | 5 (50%) | 1 (20%) | 0,5804 |
| MR | 2.47 ± 1.41 | 2.70 ± 0.45 | 2.00 ± 0.63 | 0,3835 |
| TR | 2.00 ± 0.85 | 2.20 ± 0.26 | 1.60 ± 0.37 | 0,2059 |
| INTERMACS level | 2.53 ± 0.74 | 2.50 ± 0.24 | 2.60 ± 0.34 | 0,8162 |
| RHC | ||||
| Heart rate | 76.7 ± 13.1 | 78.6 ± 4.21 | 72.8 ± 5.95 | 0,4402 |
| CVP (mmHg) | 7.2 ± 4.72 | 7.40 ± 1.55 | 6.80 ± 2.19 | 0,8263 |
| mPAP (mmHg) | 27.5 ± 9.11 | 29.7 ± 2.79 | 23.0 ± 3.95 | 0,1894 |
| PAWP (mmHg) | 18.9 ± 8.35 | 20.8 ± 2.58 | 15.0 ± 3.65 | 0,2164 |
| CI by Fick (L/min/㎡) | 1.94 ± 0.76 | 1.91 ± 0.25 | 2.01 ± 0.35 | 0,819 |
| CI by Thermo (L/min/㎡) | 2.18 ± 0.66 | 2.27 ± 0.21 | 2.03 ± 0.30 | 0,5261 |
| PVR (dyn・sec・cm‐5) | 226.3 ± 113.8 | 226.4 ± 37.3 | 226.3 ± 52.8 | 0,9992 |
| Preoperative therapy | ||||
| IMPELLA (pVAD) | 0 | 0 | 0 | ー |
| IABP | 3 (20%) | 1 (10%) | 2 (40%) | 0,2418 |
| V‐A ECMO | 0 | 0 | 0 | ー |
| Ventilator | 1 (6.7%) | 0 (0%) | 1 (20%) | 0,3333 |
| Catecholamines | 13 (86.7%) | 8 (80%) | 5 (100%) | 0,5238 |
| HD | 0 | 0 | 0 | ー |
| Preoperative aortic root and valve | All ( | Group I ( | Group N ( |
|
|---|---|---|---|---|
| Virtual basal ring diameter (mm) | 25.5 ± 3.08 | 25.7 ± 1.00 | 25.1 ± 1.42 | 0,7577 |
| Virtual basal ring diameter/BSA (mm/m2) | 15.5 ± 2.01 | 15.8 ± 0.65 | 15.1 ± 0.92 | 0,5456 |
| Valsalva diameter (mm) | 31.4 ± 4.84 | 30.8 ± 1.56 | 32.7 ± 2.20 | 0,4833 |
| Valsalva diameter/BSA (mm/m2) | 19.2 ± 2.70 | 18.9 ± 0.86 | 20.0 ± 1.22 | 0,4662 |
| ST junction diameter (mm) | 26.1 ± 4.03 | 25.9 ± 1.32 | 26.3 ± 1.86 | 0,8605 |
| ST junction diameter/BSA (mm/m2) | 16.0 ± 2.24 | 15.9 ± 0.73 | 16.1 ± 1.03 | 0,829 |
| Ascending aorta diameter (mm) | 26.8 ± 4.74 | 26.3 ± 1.53 | 27.7 ± 2.17 | 0,6008 |
| Ascending aorta diameter/BSA (mm/m2) | 16.4 ± 2.45 | 16.1 ± 0.79 | 17.0 ± 1.12 | 0,5186 |
| Geometric height (N) (mm) | 16.5 ± 1.88 | 16.1 ± 0.59 | 17.1 ± 0.84 | 0,3608 |
| Geometric height (L) (mm) | 15.1 ± 2.29 | 14.3 ± 0.63 | 16.8 ± 0.89 | 0,0391 |
| Geometric height (R) (mm) | 15.0 ± 2.78 | 14.3 ± 0.84 | 16.4 ± 1.20 | 0,1767 |
| Geometric height average (mm) | 15.5 ± 1.92 | 14.9 ± 0.55 | 16.8 ± 0.79 | 0,0797 |
| Geometric height average/BSA (mm/m2) | 9.50 ± 1.07 | 9.15 ± 0.30 | 10.2 ± 0.43 | 0,0619 |
| Effective height (N) (mm) | 9.2 ± 1.37 | 9.2 ± 0.45 | 9.2 ± 0.63 | 1 |
| Effective height (L) (mm) | 8.5 ± 1.24 | 8.3 ± 0.77 | 8.9 ± 0.56 | 0,4378 |
| Effective height (R) (mm) | 9.3 ± 1.70 | 9.0 ± 0.53 | 10.0 ± 075 | 0,2915 |
| Effective height average (mm) | 9.0 ± 1.27 | 8.8 ± 0.41 | 9.3 ± 0.58 | 0,4783 |
| Effective height average/BSA (mm/m2) | 5.5 ± 0.57 | 5.4 ± 0.18 | 5.7 ± 0.25 | 0,328 |
| Coaptation depth (N) (mm) | 3.6 ± 0.65 | 3.5 ± 0.21 | 3.6 ± 0.30 | 0,7717 |
| Coaptation depth (L) (mm) | 3.4 ± 0.52 | 3.3 ± 0.16 | 3.6 ± 0.23 | 0,2944 |
| Coaptation depth (R) (mm) | 3.6 ± 0.65 | 3.6 ± 0.21 | 3.5 ± 0.30 | 0,7703 |
| Minimum coaptation depth average (mm) | 3.1 ± 0.51 | 3.1 ± 0.16 | 3.2 ± 0.23 | 0,6878 |
| Maximum coaptation depth average (mm) | 3.9 ± 0.45 | 3.9 ± 0.15 | 4.0 ± 0.21 | 0,91 |
| Virtual basal ring/Geometric height | 1.63 ± 0.13 | 1.70 ± 0.024 | 1.48 ± 0.034 | 0,0001 |
| All ( | Group I ( | Group N ( |
| |
|---|---|---|---|---|
| Operative data | ||||
| Operation time (min) | 300.5 ± 74.9 | 321.6 ± 22.4 | 258.2 ± 31.6 | 0,1258 |
| CPB time (min) | 135.3 ± 44.4 | 148.2 ± 13.2 | 109 ± 18.7 | 0,1149 |
| Cross clamp time | ー | ー | ー | ー |
| HeartMate 3 | 11 (73.3%) | 6 (60%) | 5 (100%) | 0,2308 |
| HeartMate 2 | 1 (6.7%) | 1 (10%) | 0 (0%) | 1 |
| HeartWare | 2 (13.3%) | 2 (20%) | 0 (0%) | 0,5238 |
| Jarvik 2000 | 1 (6.67%) | 1 (10%) | 0 (0%) | 1 |
| Mitral procedure | 0 (0%) | 0 (0%) | 0 (0%) | ー |
| Tricuspid procedure | 2 (13.3%) | 1 (10%) | 1 (20%) | 1 |
| Early outcomes | ||||
| RVAD | 2 (13.3%) | 1 (10%) | 1 (20%) | 1 |
| ECMO | 1 (6.7%) | 0 (0%) | 1 (20%) | 0,3333 |
| Reexploration for bleeding | 2 (13.3%) | 2 (20%) | 0 (0%) | 0,5238 |
| In hospital death | 0 (0%) | 0 (0%) | 0 (0%) | ー |
| Latest TTE | ||||
| MR | 1.47 ± 1.36 | 1.40 ± 0.44 | 1.60 ± 0.63 | 0,7988 |
| TR | 1.73 ± 0.70 | 2.00 ± 0.19 | 1.20 ± 0.27 | 0,0319 |
| AR | 1.73 ± 0.88 | 2.10 ± 0.23 | 1.00 ± 0.33 | 0,0163 |
| Opening aortic valve | 5 (33.3%) | 2 (20%) | 3 (60%) | 0,2507 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Cardiac Structural Anomalies and Repair · Aortic Disease and Treatment Approaches
Introduction
1
De novo aortic regurgitation (AR) after left ventricular assist device (LVAD) implantation is one of the most serious complications associated with morbidity and mortality [1, 2]. De novo AR develops after LVAD implantation in many patients, even without preoperative AR or only with trivial AR [1]. Several investigators have reported the risk factors for de novo AR under LVAD support, but few studies have examined the relationship between aortic root morphology and de novo AR [3]. This study aimed to determine the relationship between the occurrence of de novo AR and the detailed preoperative morphology of the aortic root and valve.
Materials and Methods
2
As shown in the Figure S1, 15 patients who underwent preoperative electrocardiography‐synchronized contrast‐enhanced cardiac computed tomography (CT) were included in the cohort. The patients were divided into two groups: those who developed significant AR during the follow‐up period after LVAD implantation (Group I, n = 10) and those whose AR was less than trivial (Group N, n = 5). Significant AR was defined as mild or greater AR. The morphology of the aortic root and valve (Figure 1) was measured using contrast‐enhanced cardiac CT, and avoidance rates of mild or greater AR were calculated. All data were retrospectively obtained from electronic medical records. The mean follow‐up period was 1208 ± 618 days after LVAD implantation for all patients.
Aortic root morphology and definition of terms. [Color figure can be viewed at wileyonlinelibrary.com]
Echocardiographic Evaluation and Measurements of Aortic Root and Valve Morphology
2.1
Comprehensive TTE was performed according to the American Society of Echocardiography [4]. The morphology of the aortic root and valve (Figure 2) was measured using a contrast‐enhanced cardiac CT scan, as previously described by Izawa et al. [5].
(A) One‐way ANOVA and t‐test for VBD/GH with the two groups and cutoff values shown using a box plot diagram, with diamonds indicating 95% confidence intervals. (B) ROC curve and the typical aortic root morphologies of (C) Group I and (D) Group N. [Color figure can be viewed at wileyonlinelibrary.com]
Statistical Analysis
2.2
All data analyses were performed using the JMP software (version 17.0; SAS Institute Inc., Cary, NC, USA). Data are expressed as mean ± standard deviation or median and range for continuous variables, as well as numerical values (percentages) for categorical variables. Continuous variables were compared using the unpaired t‐test.
The same analysis was performed using covariates considered to be associated with the development of de novo AI as represented in Table 2. The avoidance rate of AI was analyzed using the Kaplan–Meier method.
Results
3
Baseline Characteristics
3.1
We included 15 patients with a mean age of 52 years at the time of LVAD implantation. Among these, 73% were male, and 87% had nonischemic etiology. Cardiac functions and comorbidities before LVAD implantation were comparable between Group I and Group N (Table 1).
Preoperative Aortic Root and Valve Geometry
3.2
To define anatomical predictors of de novo AR, aortic valve and aortic root morphology were assessed (Table 2) using preoperative cardiac CT following previous literature [5]. The geometric height (GH) is measured for all left, right, and noncoronary cusps, respectively, and their average is calculated. The virtual basal ring diameter (VBD) measures the diameter at the level of the most left ventricular side of the cusps at end diastole. The VBD/GH in Group I (1.70 ± 0.024) was significantly greater than that in Group N (1.48 ± 0.034) (p = 0.0001) (Figure 2A). All other measurements were not significantly different between the two groups. The ROC curve was drawn for VBD/GH with a cutoff value of 1.56 to predict mild or greater de novo AR, with a sensitivity of 1.0000 and a specificity of 1.0000 (Figure 2B).
Surgical Data and Initial Clinical Outcomes
3.3
No significant differences were found between the two groups for all items (Table 3).
Postoperative Echocardiographic Data
3.4
According to the latest echocardiographic findings, there were no significant differences between Groups I and N in the degree of mitral regurgitation (Group I: 1.40 ± 0.44, Group N: 1.60 ± 0.63, p = 0.7988) and tricuspid regurgitation (Group I: 2.00 ± 0.19, Group N: 1.20 ± 0.27, p = 0.0319).
During the follow‐up period after LVAD implantation, an aortic valve was never opened in eight (80%) patients in Group I and two (40%) patients in Group N (p = 0.2507).
De Novo AR Avoidance Rate
3.5
The long‐term de novo AR avoidance rates of the 15 patients were analyzed (Figure 3). The avoidance rates for mild or greater AR were 50%, 42%, 40%, and 37% at 6, 12, 24, and 36 months, respectively. The avoidance rates for moderate or severe AR were 80% and 73% at 24 and 36 months, respectively.
(A) Kaplan–Meier analysis showed avoidance rates for mild or greater aortic regurgitation (AR) of 50%, 42%, 40%, and 37% at 6, 12, 24, and 36 months, respectively, after left ventricular assist device (LVAD) implantation. (B) Kaplan–Meier analysis showed that the avoidance rates for moderate or greater AR were 80% and 73% at 24 and 36 months, respectively. [Color figure can be viewed at wileyonlinelibrary.com]
Discussion
4
Changes in aortic hemodynamics after LVAD implantation, older age, no aortic valve opening, smaller Valsalva sinus size, as well as lower left ventricular and aortic volumes have been reported as independent predictors of developing AR after LVAD implantation [6, 7, 8, 9, 10]. However, the relationship between the detailed morphology of the aortic root and de novo AR after LVAD implantation has scarcely been described. In the present study, a large VBD/GH was significantly associated with the occurrence of de novo AR, and although further studies on a larger number of cases are needed to confirm the present findings, the cutoff value of VBD/GH of 1.56 may be one indicator of whether or not to perform surgical intervention on the aortic valve when performing LVAD implantation surgery. Several studies have suggested that dilatation of the proximal ascending aorta [3] or a combination of the ST junction and proximal ascending aortic dilatation may be associated with the development of significant AR [11, 12]. Nishida et al. reported that dilatation of the proximal ascending aorta was a risk factor for de novo AR [3]. In their study, patients with de novo AR were significantly older than those without, and multivariable analysis failed to show an association between age and the development of de novo AR, although age‐related changes in aortic morphology can be taken into account. In the present study, there was no significant difference in age between the AR and non‐AR groups, which allowed us to compare aortic morphology without age‐related considerations. Prior literature has also shown that Cd and EH are the key factors for preventing AR; shorter Cd or shorter EH has been associated with the development of AR [11, 12, 13, 14]. The VBD/GH ratio, representing the length of aortic valve leaflet relative to aortic annulus, potentially relates to coaptation depth after increased downward pressure with continuous‐flow LVAD. Although further studies are needed, the ratio of VBD/GH can be a valuable parameter to predict de novo AR, simultaneously considering the anatomy of both the aortic root and valve leaflet.
Limitations
4.1
There are some limitations that should be addressed in this study. First, this was a single‐center, retrospective study. Selection bias and confounding factors cannot be completely excluded. Second, the sample size of this cohort study was small.
Conclusions
5
In conclusion, a greater aortic VBD/GH before LVAD surgery was associated with the occurrence of significant de novo AR after LVAD implantation.
Author Contributions
Takashi Murakami, Yusuke Misumi, and Daisuke Yoshioka contributed to the study's conception and design. Takuji Kawamura contributed to the critical revision of the article. Ai Kawamura, Shin Yajima, Shunsuke Saito, and Takashi Yamauchi contributed to data acquisition. Shigeru Miyagawa contributed to the approval of the article. Takashi Murakami drafted, and all authors revised the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Figure S1. Consecutive patients (n = 87) who underwent LVAD implantation at our institution between 2018 and 2023 were reviewed. Twenty‐three patients who underwent concurrent aortic valve surgery were excluded. Among the remaining 64 patients, 55 had no or trivial AI on preoperative transthoracic echocardiography (TTE). Of these, 15 patients who underwent preoperative electrocardiography‐synchronized contrast‐enhanced cardiac computed tomography (CT) were included in the cohort (HeartMate 3: n = 11, HeartMate II: n = 2, and HeartWare: n = 2). The patients were divided into two groups: those who developed significant AR during the follow‐up period after LVAD implantation (Group I, n = 10) and those whose AR was less than trivial (Group N, n = 5). Significant AR was defined as mild or greater AR.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1L. K. Truby , A. R. Garan , R. C. Givens , et al., “Aortic Insufficiency During Contemporary Left Ventricular Assist Device Support,” Journal of the American College of Cardiology: Heart Failure 6, no. 11 (2018): 951–960, 10.1016/j.jchf.2018.07.012.PMC 621785930384913 · doi ↗ · pubmed ↗
- 2T. Imamura , N. Narang , G. Kim , et al., “Aortic Insufficiency During Heart Mate 3 Left Ventricular Assist Device Support,” Journal of Cardiac Failure 26, no. 10 (2020): 863–869, 10.1016/j.cardfail.2020.05.013.32473380 · doi ↗ · pubmed ↗
- 3H. Nishida , T. Song , D. Onsager , et al., “Proximal Ascending Aorta Size Is Associated With the Incidence of de Novo Aortic Insufficiency With Left Ventricular Assist Device,” Heart and Vessels 37, no. 4 (2022): 647–653, 10.1007/s 00380-021-01946-4.34585275 · doi ↗ · pubmed ↗
- 4S. A. Goldstein , A. Evangelista , S. Abbara , et al., “Multimodality Imaging of Diseases of the Thoracic Aorta in Adults: From the American Society of Echocardiography and the European Association of Cardiovascular Imaging: Endorsed by the Society of Cardiovascular Computed Tomography and Society for Cardiovascular Magnetic Resonance,” Journal of the American Society of Echocardiography 28, no. 2 (2015): 119–182, 10.1016/j.echo.2014.11.015.25623219 · doi ↗ · pubmed ↗
- 5Y. Izawa , S. Mori , J. Tretter , et al., “Normative Aortic Valvar Measurements in Adults Using Cardiac Computed Tomography―A Potential Guide to Further Sophisticate Aortic Valve‐Sparing Surgery,” Circulation Journal 85, no. 7 (2021): 1059–1067, 10.1253/circj.CJ-20-0938.33408304 · doi ↗ · pubmed ↗
- 6A. Aggarwal , R. Raghuvir , P. Eryazici , et al., “The Development of Aortic Insufficiency in Continuous‐Flow Left Ventricular Assist Device‐Supported Patients,” Annals of Thoracic Surgery 95, no. 2 (2013): 493–498, 10.1016/j.athoracsur.2012.09.020.23245444 · doi ↗ · pubmed ↗
- 7J. Cowger , F. D. Pagani , J. W. Haft , M. A. Romano , K. D. Aaronson , and T. J. Kolias , “The Development of Aortic Insufficiency in Left Ventricular Assist Device‐Supported Patients,” Circulation: Heart Failure 3, no. 6 (2010): 668–674, 10.1161/CIRCHEARTFAILURE.109.917765.20739615 PMC 3089421 · doi ↗ · pubmed ↗
- 8S. W. Pak , N. Uriel , H. Takayama , et al., “Prevalence of de Novo Aortic Insufficiency During Long‐Term Support With Left Ventricular Assist Devices,” Journal of Heart and Lung Transplantation 29, no. 10 (2010): 1172–1176, 10.1016/j.healun.2010.05.018.20619680 · doi ↗ · pubmed ↗