Diagnosis and Treatment of Hypermobile Cecum Mimicking Acute Appendicitis
Malak Maaz Hassan

TL;DR
A rare case of hypermobile cecum mistaken for appendicitis is reported, highlighting the importance of CT imaging and timely surgery for accurate diagnosis and treatment.
Contribution
This case report adds to the clinical understanding of hypermobile cecum and its diagnostic challenges in acute surgical settings.
Findings
A hypermobile cecum with volvulus was diagnosed via CT scan in a patient presenting with appendicitis-like symptoms.
Emergency laparoscopy with cecopexy and appendectomy resolved the condition successfully.
CT imaging is emphasized as critical for diagnosing hypermobile cecum and avoiding misdiagnosis.
Abstract
A hypermobile cecum is a rare anomaly where incomplete fixation to the body wall causes increased mobility of the cecum and ascending colon. This condition can be asymptomatic or present with vague symptoms that can mimic other acute surgical conditions. This is a case report of a 34-year-old female patient, who presented to the emergency department with clinical symptoms suggestive of acute appendicitis like right iliac fossa pain, vomiting and nausea. After an inconclusive ultrasound, a CT scan was performed, which revealed a hypermobile cecum with volvulus. An emergency laparoscopy was performed, during which both a successful cecopexy and appendectomy were carried out. The patient recovered well post-operatively and was discharged on the fourth post-operative day. This case highlights the need for radiological imaging and the diagnostic difficulty caused by a hypermobile cecum,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
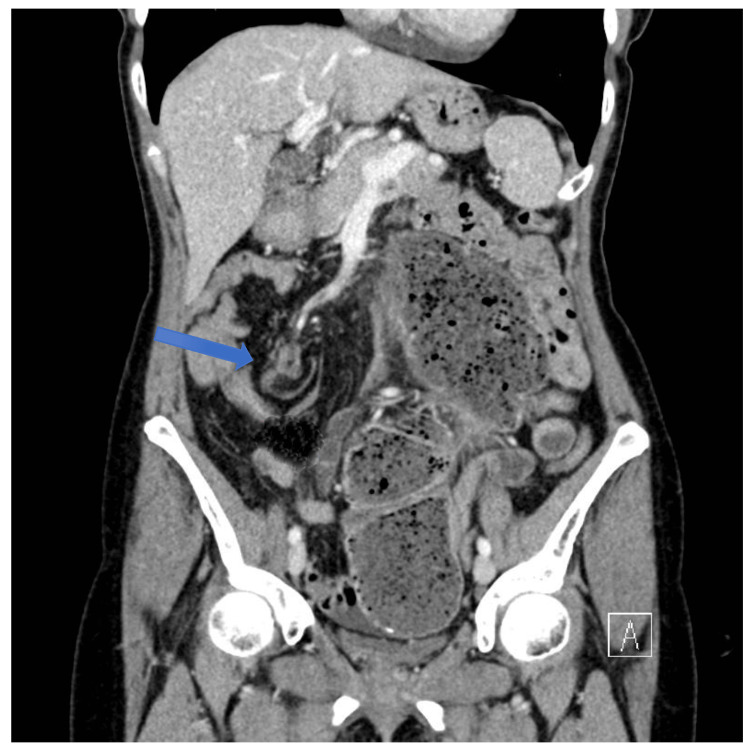 Figure 1
Figure 1| Test | Result | Normal Range |
| White Cell Count | 9.2×109/L | 3.5-11×109/L |
| Hemoglobin | 13.7 g/dL | 11.5-15 g/dL |
| Platelets | 293×109/L | 150-400×109/L |
| Red Cell Count | 4.53×1012/L | 3.8-4.8×1012/L |
| Hematocrit | 0.386 L/L | 0.37-0.47 L/L |
| Mean Cell Volume | 85 fL | 80-100 fL |
| Mean Cell Hemoglobin | 30.2 pg | 27-32 pg |
| RDW | 12% | 11-15% |
| Neutrophils | 6×109/L | 2-8×109/L |
| Lymphocytes | 2.6×109/L | 1-4×109/L |
| Monocytes | 0.4×109/L | 0.2-1.0×109/L |
| Eosinophils | 0.1×109/L | 0.0-0.5×109/L |
| Basophils | 0.0×109/L | 0.0-0.2×109/L |
| Nucleated RBCs | 0.0×109/L | 0.0-0.01×109/L |
| Test | Result | Normal Range |
| Sodium | 141 mmol/L | 133-146 mmol/L |
| Potassium | 4.6 mmol/L | 3.5-5.3 mmol/L |
| Chloride | 105 mmol/L | 95-108 mmol/L |
| Total CO2 | 26 mmol/L | 22-29 mmol/L |
| Urea | 3.4 mmol/L | 2.5-7.8 mmol/L |
| Creatinine (Enzymatic) | 67 umol/L | 45-84 umol/L |
| Estimated GFR | ≥90 mL/min/1.73sq.m | |
| Total Protein | 76 g/L | 60-80 g/L |
| Calculated Globulin | 33 g/L | 25-40 g/L |
| ALB | 43 g/L | 35-50 g/L |
| Total Bilirubin | 5 umol/L | 0-21 umol/L |
| Alkaline Phosphate | 65 IU/L | 30-130 IU/L |
| GGT | 22 IU/L | 6-42 IU/L |
| ALT | 19 IU/L | 8-41 IU/L |
| Amylase | 70 IU/L | 28-100 IU/L |
| CRP | 3.3 mg/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal Malrotation and Obstruction Disorders · Esophageal and GI Pathology · Intestinal and Peritoneal Adhesions
Introduction
A hypermobile cecum is a rare developmental anomaly that occurs due to failure of attachment of the cecum and ascending colon to the posterior body wall [1]. Bowel development starts in the fifth week of gestation and involves three main stages: herniation outside the abdominal cavity, return to the abdomen, and fixation to the body wall [2,3]. Anomalies in rotation and fixation of the developing bowel may lead to failure of fixation of the cecum and ascending colon to the posterior abdominal wall, resulting in increased mobility of the cecum and the ascending colon.
This condition can be asymptomatic but can present with vague symptoms such as recurrent right lower quadrant pain, abdominal distension, pseudo-obstruction, and, in some cases, volvulus, a serious condition requiring emergency surgery [4,5].
Owing to its atypical clinical presentation and rarity, it is usually confused with other acute surgical presentations. Radiological investigation plays an important role in diagnosis because of the non specificity of the clinical findings and laboratory tests for both mobile cecum and acute presentations. Diagnosis is often missed or delayed, posing a challenge to both clinicians and radiologists [1].
Simply fixation and suturing the cecum to the lateral peritoneum and interposition with a sponge have become outdated, and laparoscopic cecopexy is the treatment of choice now a days [4].
This case report highlights a patient with a symptomatic hypermobile cecum, emphasizing the importance of considering the differential diagnosis of this entity in recurrent or unexplained abdominal pain. A review of the diagnostic modalities and surgical management is also discussed.
Case presentation
A 34-year-old female patient with a known history of gastroesophageal reflux disease (GERD) and depression presented to the emergency department with a 12-hour history of progressively worsening right lower quadrant abdominal pain. The pain was sharp, severe, and non-radiating, and was accompanied by nausea and one episode of non-bilious vomiting. She denied any changes in bowel habits, urinary symptoms, or recent travel. There was no history of fever, anorexia, or vaginal discharge.
On examination, she was tachycardic and afebrile, with stable vital signs. Abdominal examination revealed severe tenderness in the right lower quadrant with positive guarding and Rovsing’s sign. She underwent routine blood investigations, which showed an elevated white blood cell count. C-reactive rotein (CRP), electrolytes, and renal function were normal (Tables 1, 2).
An abdominopelvic ultrasound was performed, which was inconclusive because of overlying bowel gas, and she was booked for a CT scan of the abdomen and pelvis to evaluate her symptoms. Given the typical symptoms of abdominal pain, rebound tenderness and Rovsing’s sign, a clinical diagnosis of acute appendicitis was established.
When the CT scan was done, it showed cecal volvulus, hypermobile caecum, with the caecal pole lying just to the left of midline at the level of the umbilicus and no evidence of acute appendicitis (Figure 1). She was immediately booked for an emergency laparoscopy.
CT scan of abdomen and pelvis, showing cecal volvulusThe blue arrow points to whirls, indicating twisting of cecal mesentery.
Laparoscopy revealed distension of the cecum, ileum, and jejunal loop. The colon beyond the point of rotation was collapsed. The cecum was twisted along its mesentery and located in the umbilical region. A microbiological culture was taken from the abdominal fluid, which was reported as negative. After untwisting of the cecum, the bowel showed complete recovery; therefore, an appendectomy and cecopexy were carried out. The patient recovered well post-operatively and was observed in the surgical ward. The patient was discharged on the fourth post-operative day.
Discussion
The hypermobile cecum remains asymptomatic; however patients may present with intermittent or chronic right lower quadrant abdominal pain, often mimicking appendicitis or other gastrointestinal disorders. Volvulus of the mobile cecum requires urgent surgical intervention. If not treated promptly, it can lead to serious complications such as bowel ischemia, gangrene, and perforation. Therefore, early and accurate diagnosis is crucial.
As clinical examination and laboratory tests are often non-specific, radiological investigations play a central role in diagnosis. Ultrasound is the first investigation that’s usually carried out because of its cost-effectiveness, easy availability, and the ability to exclude various surgical conditions like appendicitis or macroscopic lesions of the intestine. However, its findings are generally non-specific [6]. A CT scan is highly specific for the mobile cecum and reveals suspicion of cecum malposition [7].
Laparoscopy remains a valuable tool not only for diagnosis but also for therapeutic management. Surgical intervention depends on the patient's clinical presentation and bowel viability. Cecopexy is only suitable for volvulus if the bowel is viable, but in case of gangrenous and a grossly distended, thin-walled cecum, resection become mandatory [8]. Given the absence of ischemia in our patient, cecopexy was performed. Some surgeons advocate performing cecopexy to prevent future complications; however, there is limited consensus due to the rarity of the condition.
Conclusions
A hypermobile cecum is a rare condition that can mimic other acute surgical pathologies, making diagnosis challenging. It should be considered in the differential diagnosis of right lower quadrant abdominal pain. Clinical identification of a mobile cecum is often difficult; therefore, a CT scan is the preferred imaging modality for accurate diagnosis. The recommended treatment is cecopexy using a peritoneal flap along with an appendectomy, which helps resolve cecal volvulus and prevent recurrence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mobile cecum in a young woman with Ehlers-Danlos syndrome hypermobility type: a case report and review of the literature Intern Med Fukuda Y Higuchi Y Shinozaki K 279127965620172892412410.2169/internalmedicine.8758-16PMC 5675945 · doi ↗ · pubmed ↗
- 2Surgical diseases of the alimentary tract in infants N Engl J Med Ladd WE 7057082151936 https://doi.org/10.1056/NEJM 193610152151604
- 3Development of the human intestine and its position in the adult Johns Hopkins Hosp Bull Mall FT 19720891898 https://embryology.med.unsw.edu.au/embryology/index.php/Paper_-_Development_of_the_human_intestine_and_its_position_in_the_adult_(1898)
- 4Laparoscopic cecopexy for mobile cecum syndrome manifesting as cecal volvulus: report of a case Surg Today Tsushimi T Kurazumi H Takemoto Y Oka K Inokuchi T Seyama A Morita T 3593623820081836832910.1007/s 00595-007-3620-7 · doi ↗ · pubmed ↗
- 5Abdominal pain - a common presentation with unusual diagnosis: a case report J Community Hosp Intern Med Perspect Reddy YP Senthil Kumaran S Vanka V Rab A Patel V 604608102020 https://pubmed.ncbi.nlm.nih.gov/33194140/3319414010.1080/20009666.2020.1821469 PMC 7599011 · doi ↗ · pubmed ↗
- 6Preoperative sonographic diagnosis of midgut malrotation with volvulus in adults: the "whirlpool" sign J Clin Ultrasound Yeh WC Wang HP Chen C Wang HH Wu MS Lin JT 2792832719991035589210.1002/(sici)1097-0096(199906)27:5<279::aid-jcu 8>3.0.co;2-g · doi ↗ · pubmed ↗
- 7Cecal volvulus Dis Colon Rectum Rabinovici R Simansky DA Kaplan O Mavor E Manny J 765769331990220256610.1007/BF 02052323 · doi ↗ · pubmed ↗
- 8Twists and turns: a case report of cecal volvulus Clin Case Rep Sapkota A Batajoo A Lamichhane S Shrestha A Bhatt N 011202310.1002/ccr 3.7936 PMC 1050934037736477 · doi ↗ · pubmed ↗