Surgical management and postoperative outcomes of orbital cavernous malformations: A systematic literature review by the EANS skull base section
Edoardo Agosti, Vittorio Ricciuti, Giorgio Mantovani, Giorgia De Rosa, Pier Paolo Panciani, Marco Maria Fontanella, Cesare Zoia, Moncef Berhouma, Moncef Berhouma, Michaël Bruneau, Luigi Maria Cavallo, Jan Frederick Cornelius, Sebastien Froelich, Emmanuel Jouanneau

TL;DR
This study reviews surgical approaches for treating orbital cavernous malformations and finds that minimally invasive techniques like EEAs and ETOAs offer high success rates and fewer complications.
Contribution
The paper provides a systematic comparison of surgical approaches for OCMs, highlighting the effectiveness of endoscopic techniques.
Findings
EEAs are the most commonly used approach with high resection rates and minimal complications.
ETOAs are a promising option for laterally located lesions.
Functional outcomes like visual acuity and proptosis improved significantly post-surgery.
Abstract
Orbital cavernous malformations (OCMs) are benign vascular lesions frequently associated with progressive proptosis and visual disturbances due to their slow growth and compression of adjacent structures. Multiple surgical approaches have been developed for their treatment, including microsurgical transfacial-transorbital approaches (MTTAs), cranio-orbital approaches (MCOAs), orbitotomies (MOs), endoscopic endonasal approaches (EEAs), and endoscopic transorbital approaches (ETOAs). However, the optimal approach remains a topic of debate. This systematic review aims to compare the resection rates, postoperative complications, and clinical outcomes across various surgical approaches for OCM management. A comprehensive literature search was performed in PubMed, Embase, and the Cochrane Library according to PRISMA guidelines. Studies reporting surgical treatment of OCMs with clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
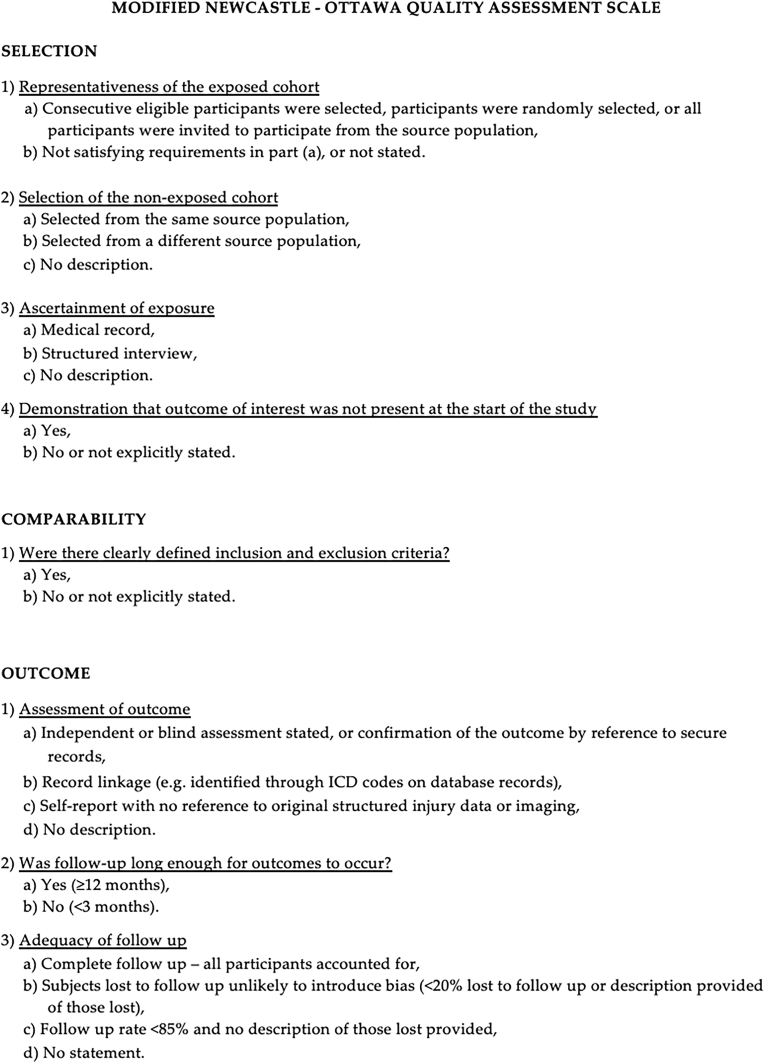 Figure 1
Figure 1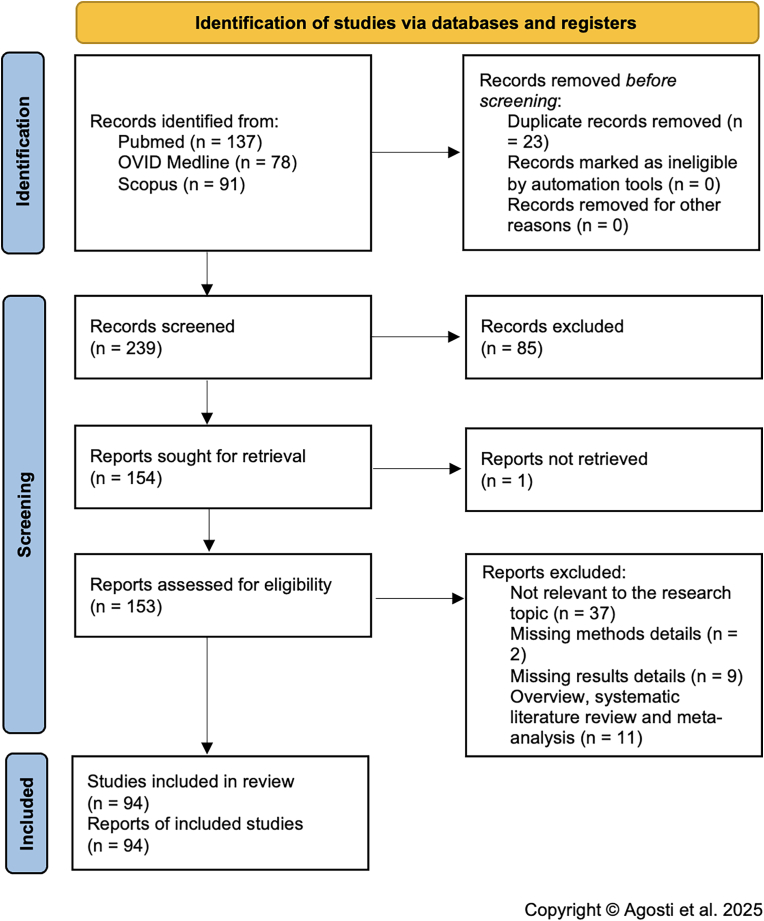 Figure 2
Figure 2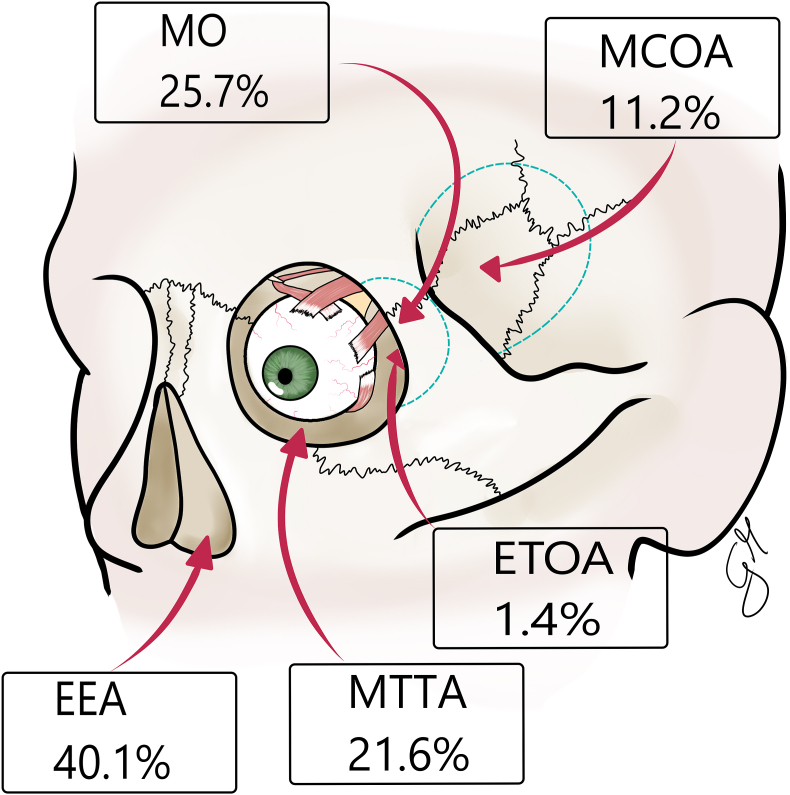 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations Diagnosis and Treatment · Meningioma and schwannoma management · Head and Neck Surgical Oncology
Introduction
1
Cavernous malformations (CMs) are vascular anomalies characterized histopathologically by dilated vascular channels containing blood products at different stages of degradation. The walls of these caverns are composed of a delicate fibrous adventitia and a single layer of endothelial cells with incomplete or dysfunctional tight junctions, leading to increased vascular permeability and potential hemorrhage into the surrounding parenchyma (Agosti et al., 2019; Fontanella et al., 2021).
Among CMs, orbital cavernous malformations (OCMs) represent a distinct subset and are the most common benign intraconal, intraorbital vascular tumors in adults (Ansari and Mafee, 2005; Bleier et al., 2016a; Castelnuovo et al., 2015). Orbital cavernous malformations account for approximately 4.3 % of orbital neoplasms and 9–13 % of all intracranial CMs. These lesions typically present between the third and fifth decades of life and are usually unilateral (Ansari and Mafee, 2005; Agosti et al., 2021a; Boari et al., 2011). Their slow growth and location within the orbit commonly lead to progressive, painless axial proptosis, which is the most frequent clinical sign. Other symptoms include visual disturbances such as reduced visual acuity, visual field defects, and dyschromatopsia due to optic nerve compression. Additionally, diplopia and extraocular motility restrictions may arise from the involvement of adjacent orbital structures (Bleier et al., 2016a; Alexander et al., 2022; Clarós et al., 2019).
Although OCMs are the most common benign vascular tumors of the orbit in adults, they remain a rare clinical entity overall. Precise incidence data are scarce, but available literature suggests an estimated occurrence of approximately 0.1–0.6 cases per 100,000 individuals annually, a figure that likely includes both symptomatic and asymptomatic lesions discovered incidentally during imaging for unrelated conditions (Fontanella et al., 2021; Castelnuovo et al., 2015; Clarós et al., 2019). This low incidence has contributed to the limited availability of large-scale, prospective studies, resulting in a fragmented evidence base for management strategies. Despite their rarity, OCMs frequently prompt surgical intervention due to progressive symptoms and their management presents significant anatomical and technical challenges. The growing number of surgical approaches and evolving minimally invasive techniques further underscores the need for a systematic synthesis of the literature to inform best practices and optimize patient outcomes (Agosti et al., 2019; Ansari and Mafee, 2005).
Surgical removal of symptomatic OCMs poses a significant challenge due to the tendency of these lesions to adhere to surrounding tissues, the risk of intraoperative bleeding, the limited working space within the orbital apex, and the potential for nerve injury (Millesi et al., 2021; Schick et al., 2003a). The choice of surgical approach depends on several factors, including lesion size, location, and relationship to the optic nerve, but also surgeon's preference and familiarity with approach. Traditionally, microsurgical transfacial-transorbital approaches (MTTAs), microsurgical cranio-orbital approaches (MCOAs) and microsurgical orbitotomies (MOs) have been the standard techniques for OCM removal. However, these approaches may be associated with significant morbidity, including cosmetic concerns and post-operative complications related to extensive tissue dissection and reconstruction (Millesi et al., 2021; Alexander et al., 2022).
In recent years, endoscopic techniques have gained increasing attention for the management of orbital pathologies (Locatelli et al., 2024; Agosti et al., 2024; Roccuzzo et al., 2024). Endoscopic endonasal approaches (EEAs) and endoscopic transorbital approaches (ETOAs) offer minimally invasive alternatives to traditional open approaches, potentially reducing surgical morbidity while maintaining efficacy (Chen et al., 2010; Bleier et al., 2016a; Clarós et al., 2019). EEAs provide a direct route to medially and inferiorly located OCMs, allowing access to the orbital apex without external incisions, brain retraction, or extensive bony removal. Initially employed for optic nerve decompression and drainage of orbital abscesses, the indications for EEAs have expanded to include tumor biopsy, debulking, and radical resection (Limawararut et al., 2006; Harris, 2010; Bleier et al., 2016a). Conversely, ETOAs, which access the orbit through small lateral or superior incisions, have emerged as a complementary technique, particularly for laterally positioned lesions. Some studies suggest that a combined endonasal and transorbital endoscopic approach may optimize surgical exposure and outcomes in select cases (Agosti et al., 2021b; Dallan et al., 2015a; Di Somma et al., 2018).
The relevance of OCMs extends beyond their rarity. These lesions, while benign, are often located in anatomically complex and functionally critical areas of the orbit, where even slow growth can lead to debilitating symptoms such as vision loss or disfigurement. As the use of high-resolution imaging has increased, incidental detection of these lesions has become more common, prompting the need for clear clinical guidelines on whether to observe or operate. Furthermore, the emergence of less invasive surgical techniques has generated ongoing debate regarding the optimal approach for different lesion locations. Despite these advances, comparative data across treatment modalities remain limited. A systematic review of the literature is warranted to assess the efficacy and safety of these different surgical strategies in the management of OCMs. Thus, this systematic review aims to compare MTTAs, MCOAs, MOs, EEAs, and ETOAs for OCM treatment, to clarify surgical outcomes and complications, inform clinical decision-making, and identify areas requiring further research in the management of OCMs.
Materials and methods
2
Literature search
2.1
A comprehensive and systematic literature search was conducted using PubMed, Embase, and the Cochrane Library, covering studies published up to December 2024. The search strategy was developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). Medical Subject Headings (MeSH) terms and free-text keywords related to OCMs and to surgical interventions were employed, including “orbital cavernous malformation," “orbital cavernous hemangioma," “surgical treatment," “microsurgical cranio-orbital approach," “microsurgical orbitotomy," “endoscopic endonasal approach," and “endoscopic transorbital approach." Boolean operators (AND, OR) were used to refine the search strategy and maximize the inclusion of relevant studies. The following search string was used: (("orbit cavernous malformation" OR “orbit cavernous hemangioma" OR “orbit vascular tumor") AND ("surgical treatment")). Additional records were identified through backward and forward citation tracking of selected articles. Only studies published in English and appearing in peer-reviewed journals were considered. Grey literature, including conference abstracts and unpublished manuscripts, was excluded to maintain a high standard of evidence reliability.
Study selection
2.2
After retrieving the initial pool of studies, duplicate records were removed. The remaining articles underwent a two-step screening process. In the first phase, four independent reviewers screened the titles and abstracts to exclude irrelevant studies. The second phase involved a full-text review of the remaining articles to determine their eligibility based on predefined inclusion and exclusion criteria. Studies were included if they reported on patients diagnosed with OCMs who underwent surgical treatment and provided clinical or surgical outcome data. Eligible studies included retrospective and prospective cohort studies, case reports and case series, and comparative studies analyzing different surgical approaches.
Exclusion criteria comprised studies focused exclusively on non-surgical management, those lacking sufficient outcome data, review articles, expert opinions, and studies involving pediatric populations if results were not analyzed separately. Disagreements between reviewers were resolved by discussion or consultation with a fifth independent investigator to ensure objectivity and consistency in study selection.
Data extraction
2.3
Data extraction was carried out independently by two authors using a standardized extraction form. Extracted data encompassed study characteristics (author, year, journal, country, study design, study period), patient demographics (sample size, mean age, sex distribution), clinical presentation (visual impairment, proptosis, diplopia, enophthalmos, extraocular muscle dysfunction, cranial nerve (CN) deficits), details on surgical approach (MTTAs, MCOAs, MOs, EEAs, and ETOAs), follow up period, details on postoperative surgical – including amount of resection (i.e. subtotal resection (STR), gross total resection (GTR), biopsy, optic canal (OC) decompression) and post-operative complications – and postoperative clinical outcomes.
Outcomes
2.4
Primary clinical outcomes included detailed ophthalmological assessments following surgery. These comprised changes in visual acuity (categorized as improved, unchanged, or worsened), presence or resolution of visual field deficits and color vision disturbances, evaluation of diplopia (new onset, persistent, or resolved), assessment of extraocular muscle function, and documentation of any new or worsening CN deficits affecting ocular motility or sensation. Primary surgical outcomes included the extent of tumor resection, classified as GTR, STR, biopsy only, or optic canal decompression. In addition, we evaluated the rate and type of postoperative complications, such as worsening visual function, diplopia, enophthalmos, CSF leak, infection, or hematoma formation.
Risk of bias assessment
2.5
The quality of the included observational studies was assessed using the Newcastle-Ottawa Scale (NOS), which evaluates studies based on selection, comparability, and outcome assessment domains (Fig. 1). (Stang, 2010) Each study was scored out of a maximum of 9 points. Studies scoring fewer than 7 points were considered low quality and excluded from the analysis. The remaining studies were included regardless of their score but were considered in subgroup analyses and narrative synthesis to interpret potential bias due to study quality. Detailed NOS scores for each study are provided in Supplementary material 1.Fig. 1. New Castel-Ottawa Scale flow chart.Fig. 1
Statistical analysis
2.6
A descriptive statistical analysis of proportions was conducted to summarize the distribution of variables. Subsequently, the Chi-square goodness-of-fit test was performed to evaluate whether the observed frequencies significantly deviated from the expected distribution, with statistical significance defined as p < 0.05.
Results
3
Literature review
3.1
A total of 239 papers were found after duplicates were eliminated. After titles and abstracts were examined, 154 papers were chosen for full-text evaluation. A total of 94 of the 153 papers that had their eligibility evaluated were included in the final assessment. The following standards were used to weed out the remaining 59 articles: 2 and 9 publications for the lack of methodological or results-related information respectively, 11 systematic literature reviews and meta-analyses, and 37 publications were not pertinent to the research topic. The PRISMA flowchart is summarized in Fig. 2. Prisma checklist is reported in Supplementary material 2. Table 1 includes details of anamnestic and clinical data of the studies included in the systematic review. Details of the radiological and surgical data from the studies that were part of the systematic review are included in Table 2. Details of clinical and surgical postoperative outcome data and follow-up duration of the studies that were part of the systematic review are detailed in Table 3.Fig. 2PRISMA flow chart.Fig. 2. Table 1Anamnestic and clinical data of the included studies.Table 1. Author, yearPeriodSample sizeAnamnestic dataClinical presentationOphthalmological signsMean Age at InterventionFemalesVisual ImpairmentProptosisPainDiplopiaOcular movement deficitRetinopathyOptic NeuropathyCorneal exposure Ocular movement deficitHobbs et al., 19611953148011011000Silva and Symon, 1984/235.5222002020Dyer et al., 19851977-1984344033000///Lyness et al., 19861984123101010000Shields et al., 1987/142111000000Ohbayashi et al., 198819802 lesions, 1 patient45111011000McNab et al., 19891968-19888547.8505077860000Leatherbarrow et al., 19891980-1988350123010000Leib et al. British., 19931982132111000000Missori et al.,1994199425460.68200400000Hassler et al., 1994/159011000000Herman et al., 1999/156111000000Hejazi et al., 19991988-19971546.281311002000Maus et al.,1999/135101000000D'hermies et al., 20002000142111001011Christensen et al., 20021999131111001011Kim et al., 2002/145111000000Schick et al.,20031988-20023751.2251927806000Papalkar et al., 2005/155111100000Monin et al., 2005/128010000000Karaki et al.,2006/150100000000Hejazi et al., 20071988-20051949.1111717077///Chaddad Neto et al., 2007/139101000000Maheshwari et al., 2007200214111000100Cheng et al., 20082001-20053945.4219321850000Yan et al., 20082005154001000000Stamm et al.,2009/133011001000Tang Cho et al., 201020101050640002200Yoshimura et al.,20102010148011000010Cho et al., 20101998-2006940.9826004100Gazioglu et al., 2011/150010000000Campbell et al., 2011/157111000000Boari et al., 20111999-2009204514512650000Locatelli et al., 20112012159111000000Arora et al., 2011/140111001000Muscatello et al., 20122011354202000000Yamamoto et al.,2012/161001111000Meena et al., 2012/129001000000Netuka et al., 20132010-2011257.5220000000Wu et al., 20132008-20121242.6812/000000Aymard et al.,2013201343/25131023/9//Murray et al.,2013/143000000000Healy et al.,2014/139111000000Chhabra et al.,20142007-2011554.4255030000Yang et al., 20142002-20107441.1474353123340150Dallan et al.,2015/1/111000010Koch et al.,20152014151111000000Ikonomidis et al.,2015/157011000000Kang et al., 20162016159111000010Chen et al.,20162009-2016943.521100000110Bleier et al.,2016/2350.913158650000Xue et al., 2016/347.3320000000Wang et al.,20172014949.1659000030Louisraj et al.,20172017126101111000Bagheri et al.,20182001-201660403695461/24//Bagheri et al.,2018/128011000000Golden et al.,201820181041/0100000/Dallan et al.,20192008-20172346.113148031000Marcellino et al.,2019/152110000000Castelnuovo et al., 2019/234/12000000Claros et al.,20191997-20177637.842327614101031179Hegde et al.,2019/165101110000Kim et al., 20192006-20171844.814516106000Zoli et al., 20192019147001111111An et al., 20202018147100000000Quin et al., 2020/153111000000Rimmer et al.,2020201-20187//30010000May et al., 2020/162001000000Strianese et al.,20212005-201616444.4955013213213523//Fong Ng et al., 2021/164110000000De Feudis et al., 2021/142101100000Li et al., 20212016-20201849.91110853////Almeida et al.,202120191401/1000000Millesi et al.,20212002-20193550221115040000Lao et al.,2021/137011000010Zoli et al., 20212002-2018458320010000Austria et al.,2021/166101000000Li et al., 2021/168110000000de Melo Junior et al.,20212021162000001000Park et al., 2022/143011000010Zhou et al.,20222018-20211945.119140000060Essayed et al., 2022/147101100000Yang et al., 20222003-20203543.325350000000Ayoub et al.,20222022149100000000Almatrudi et al.,2023/11001001001Lai et al., 2023/114100001000Leocata et al.,2023/145110000000Jaxa-Kwiatkowski et al., 2023/135/11000000Finisanti et al., 2023/120101100000Das et al., 2023/326.7233003000Dalfino et al.,20232023155111000000Gulsuna et al.,20242018-20231335.1872251000Kushwaha et al.,2024/148111011000Abdulla et al.,2024202411010000000Table 2Radiological and surgical data of the included studies.Table 2. Author, yearLocationPositionSize (cm)Surgical TreatmentIntraconalExtraconalOptic CanalMedialLateralSuperiorInferiorEEAMTTAMCOAMOETOAHobbs et al., 1961NANANA10002.8x2.3x1.401000Costa e Silva et al., 198400200000.45x0.3500200Dyer et al., 1985NANA002003 × 3 × 200300Lyness et al., 198610001005x4x400010Shields et al., 19871000100/00010Ohbayashi et al., 198802002002.8x1.80011McNab et al., 1989NANA216652926/0104710Leatherbarrow et al., 19893003000/03000Leib et al. British., 199310010002.3x1.7x1.400010Missori et al.,19940000000/00000Hassler et al., 199410000014x201000Herman et al., 199910010011.1x0.8x1.210000Hejazi et al., 199913207330/04830Maus et al.,19991000100/00100D'hermies et al., 200010011105x4x300100Christensen et al., 200210011105x4x300100Kim et al., 200210000012.3x3x3x700010Schick et al.,200331511315713/1917100Papalkar et al., 200510000102x1.5x100100Monin et al., 200500100001.4x0.510000Karaki et al.,20061001000/10000Hejazi et al., 200719004357/07930Chaddad Neto et al., 2007///1010/00100Maheshwari et al., 200701010002.7x1.4x1.801000Cheng et al., 20083900435930/039000Yan et al., 200801000011.7x2.201000Stamm et al.,20091001000/10000Tang Cho et al., 2010/0000///000010Yoshimura et al.,20101001001/10000Cho et al., 20105403//12.3x1.809000Gazioglu et al., 20111001000/10000Campbell et al., 2011//000012.5x1.9x1x711000Boari et al., 201120007605/001280Locatelli et al., 201110010011.1x0.8x1.210000Arora et al., 201110001001.6x100010Muscatello et al., 20122102001/21000Yamamoto et al.,20121000101/00100Meena et al., 201210001012x1.5x1.500010Netuka et al., 20131112000/20000Wu et al., 2013//290012x1.2120000Aymard et al.,2013158/00///0/0/0Murray et al.,201310010001.6x1.8x1.510000Healy et al.,201410010011.3x1.3x1.310000Chhabra et al.,2014///50001.6850000Yang et al., 201474007401413/069050Dallan et al.,20151001010/00100Koch et al.,20151001010/00100Ikonomidis et al.,201510000011.7x2.110000Kang et al., 20161001001/10000Chen et al.,2016001100000-5x0.4x0.3110000Bleier et al.,20161435////1.57x1.15x1.09230000Xue et al., 20163001101/01200Wang et al.,201763090271.9x1.6x1.390000Louisraj et al.,20171000101/00100Bagheri et al.,2018582/949///0100500Bagheri et al.,201801000013.5x2.5x200010Golden et al.,2018//0000//001000Dallan et al.,20191670230//1.9x1.5x1.4230000Marcellino et al.,20190101000/10000Castelnuovo et al., 201922020001.8x1.1420000Claros et al.,2019724066600/040720Hegde et al.,201910001002.7x1.4x1.400010Kim et al., 20191800711612/00080Zoli et al., 20191111111111111An et al., 20201001001/10000Quin et al., 20200110111/00100Rimmer et al.,2020420////1.9x1.4x1.777000May et al., 20201001000/01000Strianese et al.,20211303440491005852/0013000Fong Ng et al., 202110101001x1x100001De Feudis et al., 20211001010/01000Li et al., 2021126/1614122x1.6x1x6162000Almeida et al.,20211001001/01000Millesi et al.,20213140613792.10131480Lao et al.,202110010012.6x1.6x1.910000Zoli et al., 20214003122/30001Austria et al.,20210100001/00010Li et al., 20210101000/10000de Melo Junior et al.,202101000102.3x1.3x201000Park et al., 202210010002x1.5x1.710000Zhou et al.,2022190//////190000Essayed et al., 20221001000/00100Yang et al., 2022350026009/2201300Ayoub et al.,20221001001/10000Almatrudi et al.,20231000110/01000Lai et al., 202301000102.3x1.3x201000Leocata et al.,20231001000/10000Jaxa-Kwiatkowski et al., 202310010004.3x3.5x3.400100Finisanti et al., 20230100100/10000Das et al., 20233002100/00120Dalfino et al.,20231001010/00100Gulsuna et al.,2024121313023/130000Kushwaha et al.,202410010002x201000Abdulla et al.,20240110111/00100Table 3Postoperative clinical and surgical outcome data of the included studies.Table 3. Postoperative Clinical OutcomesPostoperative Surgical OutcomesFU (months)ResectionComplicationsAuthor, yearVisual Acuity ImprovementOcular Movement ImprovementProptosis ImprovementDiplopia ImprovementGTRSTRBiopsyOC decompressionInfectionsVisual Acuity deficit appearance/worseningDiplopia Appearance/WorseningEnophthalmosOcular Movement deficit appearance/WorseningRecurrenceHobbs, 19611111100000000060Costa e Silva et al., 198412202000000000/Dyer and Atkinson, 1985100030000111006Lyness and Williams, 1986001100100000006Shields et al., 19871010100000000024Ohbayashi et al., 198811112000/0000//McNab and Wright, 198931///80500/75030/Leatherbarrow et al., 19891021102000001117Leib et al. British., 199310101000000000/Missori et al.,1994//8/0403000000/Hassler et al., 1994001010000000008Herman et al., 1999100000000000006Hejazi et al., 19998//////////////Maus et al.,199900101000000000/D'hermies et al., 200000101000000000/Christensen et al., 20020010100000000024Kim et al., 2002101010100000006Schick et al., 2003b1442103700002000/12.65Papalkar et al., 200510101000000000/Monin et al., 20051000001100000//Karaki et al., 200600001000000000/Hejazi et al., 200714//7/////0000/37Chaddad Neto et al., 200700/0100000000036Maheshwari and Thool, 20070010100000000111Cheng et al., 2008603253720002000018Yan et al., 200800101000000000/Stamm and Nogueira, 20091///1000000000/Tang Cho et al., 20104////0000/000012Yoshimura et al., 20101010101/1000008Cho et al., 20102490900000000029Gazioglu et al., 2011100010000000003Campbell et al., 2011100010000000003Boari et al., 2011401222000001000047.15Locatelli et al., 2011101010000000005Arora et al., 2011////1000///////Muscatello et al., 201310003000000000/Yamamoto et al., 201201010100000000/Meena et al., 2012001010000000019Netuka et al., 20132000200000000021Wu et al., 2013120001200000000011.8Aymard et al.,2013NANANANA32000003020/Murray et al., 20130000100000000012Healy et al., 2014101010000000003Chhabra et al., 20145053410000020024Yang and Yan, 201424/74/7400006/012/Dallan et al.,20151010100000000012Koch et al., 20151010100000000015Ikonomidis et al., 2015100010000001003Kang et al., 20161010100000000012Chen et al.,2016110001100110000009.9Bleier et al., 2016b12/8317222/065///Xue et al., 2016300030000000006Wang et al.,2017309090000206004.5Louisraj et al., 20170101010000000011Bagheri et al.,2018////6000000404061.4Bagheri et al.,2018101010000000003Golden et al., 201800000///0000///Dallan et al., 201810/8/1640300000052.9Marcellino et al., 201910001000000000/Castelnuovo et al., 2019102020000000008Claros et al.,201924///7600000000/6Hegde et al., 20191011100000000012Kim et al., 20194/16/////00001011.2Zoli et al., 2019111111111111111An et al., 2020000010000000003Quin et al., 202010101000000000/Rimmer et al., 2020////301000000//May et al., 202100101000000000/Strianese et al.,202142251301616400002500077Fong Ng et al., 202210001001000000/De Feudis et al., 2021001010000000003Li et al., 2021////141030400006Almeida et al.,2021000010000000016Millesi et al.,2021601523500000100//Lao et al.,2021////10000//////Zoli et al., 202110014000000000/Austria et al.,2021001010000000008Li et al., 2021100010000000003de Melo Junior et al.,2021000010000100001Park et al., 20221010100000010012Zhou et al., 202214000190000000006.71Essayed and Al-Mefty, 202210101000000000/Yang et al., 2022170003500009000064.5Ayoub et al., 2022000010000000003Almatrudi et al., 20230110///0000000/Lai et al., 20230000100000000036Leocata et al., 2023100010000000006Jaxa-Kwiatkowski et al., 2023111010000000003Finisanti et al., 2023001010000000003Das et al., 20232030300000000016Dalfino et al.,202310101000000000/Gulsuna et al., 202441241300001000021Kushwaha et al.,202411111000000000/Abdulla et al., 202410101000000000/
All included studies were assessed for methodological quality using the Newcastle-Ottawa Scale (NOS). A total of 94 studies underwent quality evaluation, and all were found to have a score equal to or greater than 7, reflecting an acceptable to high level of methodological rigor. Specifically, 41 studies (43.6 %) scored 7, 40 studies (42.6 %) scored 8, and 13 studies (13.8 %) scored 9. This distribution indicates a strong overall quality among the included studies. Although detailed NOS scoring is provided in Supplementary Material 1.
Data analysis
3.1.1
Anamnestic and clinical data
3.1.1.1
The study analyzed 1007 patients with a mean age of 43.9 years (range: 1–85). Females accounted for 58.5 % of the cohort, a significantly higher proportion compared to males (p = 0.04). Among clinical presentations, proptosis was the most frequent symptom (63.2 %), followed by visual impairment (48.1 %). Less common manifestations included ocular movement deficit, pain, and diplopia (p = 0.006). Regarding ophthalmological signs, retinopathy was the most prevalent finding (9.1 %), followed by optic neuropathy and corneal exposure due to ocular movement deficit (p < 0.0001) (Table 4).Table 4. Summary of anamnestic and clinical data of the included studies.Table 4Total Patients N1007Anamnestic dataAge means (range)43.9 (1-85)Females %58.5 (589/1007)Clinical dataClinical presentation %Visual impairment48.1 (485/1007)Proptosis63.2 (637/1007)Pain11.3 (114/1007)Diplopia9.4 (95/1007)Ocular movement Deficit12.5 (126/1007)Ophthalmological signs %Retinopathy9.1 (92/1007)Optic neuropathy6.1 (62/1007)Corneal exposure ocular movement deficit1.2 (13/1007)
Radiological and surgical data
3.1.1.2
Radiological analysis revealed a predominant intraconal localization (80 %), with significantly fewer cases in the extraconal space or optic canal (p < 0.001). Lesions were more frequently found in the lateral position (39 %), while medial, inferior, and superior locations were less common (p = 0.01). The selection of technique could vary significantly based on lesion location, underlying the importance of tailored surgical planning (Table 5). The EEAs were the most used approaches (40.1 %), followed by MOs and MTTAs (25.7 % and 21.6 % respectively) (Fig. 3).Table 5. Summary of radiological and surgical data of the included studies.Table 5Radiological dataMean maximum diameter (cm) N (range)3 (0.45–5)Location % (N/tot)Intraconal80 (701/876)Extraconal11.8 (103/876)Optic canal8.2 (72/876)Position % (N/tot)Medial25.8 (285/1104)Lateral39 (431/1104)Superior14.7 (162/1104)Inferior20.5 (226/1104)**Surgical approach % (N/tot)**EEA40.1 (393/979)MTTA21.6 (211/979)MCOA11.2 (110/979)MO25.7 (251/979)ETOA1.4 (14/979)Fig. 3. Schematic representation of the surgical approaches. MO: Microsurgical Orbitotomy, MCOA: Microsurgical Cranio-Orbital Approaches, MTTA: Microsurgical Transfacial-Transorbital approaches, EEA: Endoscopic Endonasal Approaches, ETOA: Endoscopic Transorbital Approaches.Fig. 3
Post-operative surgical and clinical outcomes
3.1.1.3
Postoperative outcomes varied significantly depending on the surgical approach (p < 0.001). Gross total resection was achieved in 93.7 % of cases, while STR, biopsy, and optic canal decompression were performed in a minority of patients (p < 0.001). Postoperative complications occurred at low rates, with visual acuity worsening (3.9 %), diplopia (2.4 %), enophthalmos (1.7 %), and ocular movement deficits (1.1 %) (p = 0.002). Clinical outcomes demonstrated significant improvements, with visual acuity improving in 65.1 %, ocular movement in 34.9 %, proptosis in 61.6 %, and diplopia in 56.8 % of cases (p = 0.03) (Table 6).Table 6. Summary of postoperative clinical and surgical outcome data of the included studies.Table 6**Postoperative surgical outcome % (N/tot)**ResectionGTR93.7 (821/876)STR2.5 (22/876)Biopsy0.9 (8/876)OC decompression2.9 (25/876)ComplicationsInfection0.1 (1/979)Visual acuity deficit appearance/worsening3.9 (38/979)Diplopia appearance/worsening2.4 (23/979)Enophthalmos1.7 (17/979)Ocular movement deficit appearance/worsening1.1 (11/979)Recurrence0.7 (6/821)**Postoperative clinical outcome % (N/tot)**Visual acuity improvement65.1 (316/485)Ocular movement improvement34.9 (44/126)Proptosis improvement61.6 (393/637)Diplopia improvement56.8 (54/95)
Discussion
4
Our systematic review highlights the predominance of the EEAs over traditional techniques, with an emerging role in the last years of ETOAs. Gross total resection was achieved in majority of cases, with significant improvements in visual acuity, proptosis, and diplopia. The low complication rates reinforce the safety and efficacy of modern surgical strategies for orbital cavernous malformations.
Clinical presentations
4.1
The propensity for OCMs to cause visual disturbances is well-documented (Almeida et al., 2022; Lao et al., 2021; Austria et al., 2023). In our systematic review, nearly half of the patients reported visual impairment. The insidious growth pattern of OCMs often leads to delayed diagnoses. Clinical symptoms are frequently attributed to more common orbital pathologies, resulting in misdiagnoses. Our findings reveal that a significant proportion of patients experienced delayed recognition of their condition, emphasizing the need for heightened clinical suspicion, especially in cases presenting with unexplained proptosis or visual decline. A study by Yang et al. (2021) analyzed 35 patients with OCMs located under the optic nerve sheath in the orbital apex or common tendon ring. They reported a high rate of misdiagnosis (57.1 %), with many cases initially mistaken for optic neuritis. Additionally, 65.7 % of patients experienced acute or subacute visual acuity deterioration, primarily due to hemorrhagic events within the lesion. These acute presentations contrast with the more gradual symptom progression observed in our review, suggesting that lesion location, particularly in proximity to critical structures like the optic nerve, may precipitate more rapid clinical declines. A case reported by Lao et al. (2021) described a patient with an OCM in the infraorbital canal presenting with intense headaches and visual disturbances, initially misdiagnosed as an infraorbital nerve neurofibroma. This case highlights the diagnostic challenges posed by atypical clinical presentations.
The anatomical positioning of OCMs significantly influences their clinical manifestations (Zoia et al., 2024a; Fontanella et al., 2021; Castelnuovo et al., 2019). Our review indicates that 80 % of lesions are intraconal. This intraconal predominance often results in symptoms, such as proptosis and visual disturbances, due to mass effect on adjacent ocular structures. Conversely, extraconal lesions may present with less pronounced proptosis but can still cause significant visual impairment if they exert pressure on the optic apparatus.
While our systematic review focuses on surgical outcomes, it is important to acknowledge that not all OCMs require immediate intervention. The decision to pursue surgery versus conservative management is influenced by lesion size, growth rate, anatomical location, presence of symptoms (particularly visual impairment), and patient preference. Surveillance with periodic imaging is often recommended for small, asymptomatic, or incidentally discovered lesions. Surgical resection, which is indicated in the presence of progressive symptoms or radiological growth, remains the most frequently employed treatment modality, reported in 40–60 % of cases. Radiotherapy, while rarely used, may be considered in select situations involving unresectable lesions or high surgical risk.
Surgical treatment
4.2
Our systematic review highlights the predominance of the EEAs, followed by MOs, MCOAs, and ETOAs. This distribution underscores the evolving preference for less invasive techniques in the treatment of OCMs, aligning with recent literature emphasizing the benefits of minimally invasive approaches in reducing morbidity and improving patient outcomes.
Microsurgical cranio-orbital approaches, once considered the gold standard for deeply located OCMs, provide extensive exposure and direct visualization of the lesion but come with considerable drawbacks. Studies such as those by Yang et al. (2021) have reported increased operative times, risk of neurovascular injury, and prolonged recovery periods associated with these approaches. We reported a decreasing trend of MCOAs (10.9 %). Our data reflect this shift away from MTTAs and MCOAs, with their relatively low utilization suggesting that surgeons increasingly prioritize approaches that minimize surgical trauma while maintaining efficacy.
Microsurgical orbitotomies remain a widely used technique, particularly for lateral and extraconal lesions. They offer a balance between adequate exposure and minimized invasiveness compared to MTTAs and MCOAs, as confirmed by several studies (Aymard et al., 2013). However, complications such as ocular muscle damage, nerve injury, and postoperative diplopia remain concerns. The external incisions required for MOs also pose cosmetic considerations, leading to a preference for less invasive options when feasible.
Endoscopic endonasal approaches (EEAs) have emerged as the most frequently employed surgical technique, accounting for the largest proportion of cases in our review (Zoia et al., 2024b; Bleier et al., 2016a; An et al., 2020; Park et al., 2022). This approach offers a direct route to medial and inferomedial orbital lesions via the nasal corridor, avoiding external incisions and reducing the risk of cosmetic deformities. The literature supports this trend, with Lao et al. (2021) demonstrating that EEAs facilitate effective resection of deep-seated orbital lesions with minimal complications. Moreover, advances in endoscopic technology and surgical expertise have broadened the applicability of EEAs, contributing to their growing preference among surgeons. While often labeled as “minimally invasive,” this characterization of EEA has been debated. The creation of a nasoseptal flap, wide bilateral sphenoidotomies, and extensive manipulation of sinonasal structures can result in non-negligible soft tissue trauma. This includes risks of postoperative nasal crusting, olfactory dysfunction, and septal perforation, which may not occur with the same frequency in some transcranial approaches. Thus, when weighing the advantages of EEA, it is crucial to also consider these potential morbidities (Chen et al., 2017). Despite these considerations, EEAs remain attractive for orbital cavernous malformation management due to their ability to provide direct access to medial orbital lesions, minimize brain retraction, and offer favorable cosmetic outcomes (Dallan et al., 2015a). When selected appropriately, they can still achieve high rates of gross total resection with fewer neurological complications compared to traditional open approaches.
Endoscopic transorbital approaches, despite their potential, remain underutilized, representing only a small fraction of cases in our review. While these approaches provide access to lateral and superior orbital lesions through eyebrow, eyelid, or conjunctival routes, their limited exposure and steep learning curve contribute to their restricted adoption (Agosti et al., 2021b, 2023; De Simone et al., 2024; Zoia et al., 2024c). Dallan et al. (2015b) highlighted the successful use of ETOAs in specific cases, yet their widespread application remains constrained. Nonetheless, with further refinement and increasing surgical expertise, ETOAs may become a more viable alternative in select cases (Zoia et al., 2019, 2023).
While it is conceptually accepted that surgical approach selection should be dictated by the anatomical location of the OCM, our analysis of the literature reveals a more complex and variable reality. Despite the theoretical alignment between lesion site and surgical corridor, several studies deviated from this paradigm. For instance, Boari et al. (2011) and Yang et al.(Kushwaha et al., 2024) reported resecting predominantly lateral lesions via midline transcranial approaches, such as the frontotemporal or pterional routes, rather than employing more direct lateral orbitotomies or transorbital techniques. Similarly, our review identified multiple cases where inferomedial lesions were accessed through extended transcranial exposures, despite the availability of endoscopic endonasal or transconjunctival options. This pattern suggests that, in many instances, surgical decision-making is influenced less by anatomical logic than by factors such as surgeon expertise, institutional familiarity with specific techniques, and access to specialized equipment (Missori et al., 1994; Maus and Goldman, 1999; Aymard et al., 2013; Kim et al., 2019). Moreover, we observed that centers contributing larger case series often adhered to a consistent approach across varied lesion locations, reinforcing the idea that personal or institutional preference can supersede lesion-specific tailoring. These findings emphasize a key limitation in the assumption that current practice reflects true anatomic customization.
Regardless of the surgical approach selected, the incorporation of image-guided navigation systems has become an essential adjunct in OCM surgery. While navigation offers value in both microsurgical and endoscopic procedures, its relevance is particularly pronounced in the context of endoscopic techniques, where conventional anatomical landmarks may be distorted, obscured, or absent due to prior interventions or lesion-related anatomical changes. In such scenarios, real-time navigation enables accurate localization and delineation of lesion boundaries relative to adjacent critical structures such as the optic nerve, medial rectus muscle, ophthalmic artery, and internal carotid artery (Kim et al., 2019). This facilitates safe dissection, minimizes the risk of iatrogenic injury, and improves the extent of resection. In endoscopic endonasal and transorbital procedures, where the field of view is limited and the working corridor is narrow, navigation compensates for these constraints by providing three-dimensional orientation and enhancing the surgeon's spatial awareness (Zoli et al., 2021). Moreover, navigation-guided surgery reduces reliance on extensive exposure, thereby preserving surrounding soft tissues and further supporting the minimally invasive paradigm. Studies have demonstrated that the use of intraoperative navigation can lead to decreased operative times, reduced complication rates, and improved surgical confidence, particularly during complex skull base or medial orbital interventions (Agosti et al., 2023).
Postoperative clinical and surgical outcomes
4.3
Resection rates remain a critical factor in evaluating surgical effectiveness. Several studies, including Aymard et al. (2013) and Calandriello et al. (2017), report high GTR rates using lateral orbitotomy and transcranial approaches, ranging between 85 % and 95 %. However, these techniques often require significant manipulation of the orbital contents, increasing the risk of optic nerve injury and prolonged recovery. In contrast, our systematic review aligns with the findings of Bleier et al. (2016a) and Castelnuovo et al. (2019), demonstrating that EEAs achieve comparable GTR rates (80 %–90 %) with minimal orbital disruption. This approach facilitates direct access to the medial orbital compartment via the skull base, avoiding unnecessary retraction and reducing surgical morbidity. Although EEAs may be less effective for laterally located OCMs, their success in medial lesions makes them a superior choice in many cases.
Postoperative complications further differentiate these approaches. Transcranial and lateral orbitotomy techniques, as reported by Dalfino et al. (2023) and de Melo Junior et al.(de et al., 2021), are associated with higher rates of periorbital hematoma (up to 20 %), optic nerve edema (10 %–15 %), and persistent diplopia (25 %–40 %). Our systematic review corroborates the findings of An et al. (2020) and Park et al. (2022), indicating that EEAs significantly reduce the risk of optic nerve injury and external scarring. However, EEAs have an inherent risk of cerebrospinal fluid (CSF) leaks (reported between 5 % and 15 %), necessitating meticulous skull base reconstruction techniques, such as nasoseptal flap coverage, to mitigate this complication. Notably, with advancements in endoscopic skull base reconstruction, CSF leak rates have substantially declined, reinforcing the safety profile of EEAs (Zoia et al., 2018).
Clinical outcomes and functional preservation are paramount in surgical decision-making (Fontanella et al., 2022; Clarós et al., 2019). Traditional transcranial and lateral orbitotomy techniques, despite achieving high resection rates, often lead to prolonged hospital stays and delayed recovery due to extensive tissue disruption. Additionally, patients undergoing EEAs report lower rates of postoperative diplopia and periorbital swelling, likely due to the minimally invasive nature of the procedure. Despite these benefits, EEAs may be limited in addressing laterally located lesions or those encasing major vascular structures, necessitating a tailored, case-specific approach.
Limitations
4.4
The primary limitation of this systematic review is the heterogeneity of the included studies, which complicates direct comparison due to variations in patient selection, lesion characteristics, surgical indications, and operative techniques. A significant proportion of the included literature (i.e., 56 out of 94 studies) consisted of case reports, which inherently limits the robustness of aggregated data. While these reports provide valuable anecdotal insights, they are subject to reporting bias and do not offer consistent or comprehensive data on complications or long-term outcomes. This aggregation of isolated experiences may therefore skew interpretation and dilute the reliability of conclusions regarding the comparative safety and efficacy of surgical approaches. Additionally, the expertise appears to be concentrated within a limited number of high-volume centers, with only 23 groups reporting more than 10 cases, highlighting a potential imbalance in experience distribution that may influence outcome generalizability.
The predominance of retrospective single-center studies and case series further reduces the overall level of evidence. Inconsistencies in reporting, particularly in relation to postoperative complications and long-term follow-up, limit the ability to assess recurrence rates or functional outcomes across surgical modalities. Moreover, data variability precluded meaningful statistical synthesis or meta-analysis. The lack of standardized outcome measures and reporting criteria across studies also increases the risk of publication bias, as favorable results are more likely to be published than studies with negative or inconclusive findings. Collectively, these limitations underscore the need for multicenter prospective studies with uniform outcome reporting to better define the optimal surgical strategy for orbital cavernous malformations.
Additionally, the analysis of postoperative complications was limited by inconsistent reporting across studies, particularly in distinguishing transient from permanent deficits. In many cases, complication details were sparsely described or variably categorized, limiting the ability to conduct a granular analysis. Importantly, complications are multifactorial events influenced by patient-specific factors, lesion size and location, surgical approach, and surgeon experience. Given these complex interdependencies, and the absence of individual patient data across studies, we were unable to perform a multivariate analysis to control for confounding variables. As such, while our findings suggest trends in complication rates associated with different approaches, these associations should be interpreted cautiously and not assumed to reflect direct causality.
Moreover, while a GTR rate of 94 % was reported across studies, the definition of resection completeness was often unclear or inconsistently applied. In many cases, it was not specified whether GTR was determined by intraoperative assessment or confirmed through postoperative imaging, limiting the objectivity and reproducibility of this outcome metric. Additionally, follow-up durations were generally short and heterogeneously reported. Only three studies included a follow-up period exceeding five years, which restricts our ability to assess the long-term behavior, recurrence potential, or delayed complications of orbital cavernous malformations. This limitation significantly impacts the interpretation of disease control and surgical durability over time.
Conclusions
5
Our systematic review highlights the predominancy of EEAs in the surgical management of OCMs, with an emerging role in the last years of ETOAs. Endoscopic techniques could offer a less invasive, direct route for both medially and laterally located lesions, reducing complications while preserving orbital function.
Ethical approval
Not applicable.
Funding
No funding was received for this research.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abdulla E.Abdulla Z.Alalawi W.Fathalla S.Asad F.Successful management of a large orbital hemangioma in an infant: a case report Cureus 1642024 e 5806210.7759/cureus.58062 PMC 1108844938738043 · doi ↗ · pubmed ↗
- 2Agosti E.Flemming K.D.Lanzino G.Symptomatic cavernous malformation presenting with seizure without hemorrhage: analysis of factors influencing clinical presentation World Neurosurg.1292019 e 387e 39210.1016/j.wneu.2019.05.15731132505 · doi ↗ · pubmed ↗
- 3Agosti E.Doglietto F.Fontanella M.M.Letter to the Editor. Bleeding risk after cavernous malformation surgery: remnant or recurrence?J. Neurosurg.1353202197897910.3171/2020.12.JNS 20419233711810 · doi ↗ · pubmed ↗
- 4Agosti E.Turri-Zanoni M.Saraceno G.Quantitative anatomic comparison of microsurgical transcranial, endoscopic endonasal, and transorbital approaches to the spheno-orbital region Oper. Neurosurg.2162021 E 494E 50510.1093/ons/opab 31034467999 · doi ↗ · pubmed ↗
- 5Agosti E.Zeppieri M.De Maria L.Surgical treatment of spheno-orbital meningiomas: a systematic review and meta-analysis of surgical techniques and outcomes J. Clin. Med.12182023584010.3390/jcm 1218584037762781 PMC 10531637 · doi ↗ · pubmed ↗
- 6Agosti E.Alexander A.Y.Plou P.360° around the orbit: key surgical anatomy of the microsurgical and endoscopic cranio-orbital and orbitocranial approaches Neurosurg. Focus 5642024 E 210.3171/2024.1.FOCUS 2386638560949 · doi ↗ · pubmed ↗
- 7Alexander A.Y.Agosti E.Leonel L.C.P.C.Kerezoudis P.Peris-Celda M.Lanzino G.Interhemispheric Precuneal Transtentorial approach to a dorsal pontine cavernous malformation: 2-dimensional operative video Oper. Neurosurg.2332022 e 17310.1227/ons.000000000000030135972100 · doi ↗ · pubmed ↗
- 8Almatrudi M.Alnowaishiri K.Babiker S.Alsufyani D.Abdelaziz A.Surgical intervention in pediatric orbital hemangioma: a case report Cureus 15122023 e 5015610.7759/cureus.50156 PMC 1077163038186409 · doi ↗ · pubmed ↗