An Incidental Embolism
Emma Alley, Eric Melnychuk

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
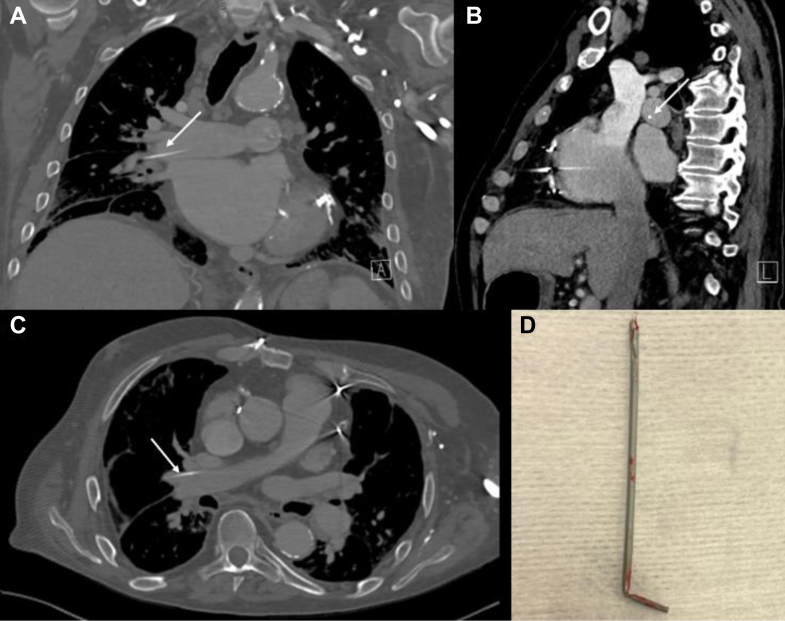 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutopsy Techniques and Outcomes · Traumatic Ocular and Foreign Body Injuries · Organ Donation and Transplantation
Case Presentation
1
A 70-year-old man presented to the emergency department for increased falls and generalized weakness at home. He had a medical history of myocardial infarction, coronary artery bypass grafting, end-stage renal disease on hemodialysis, and a ruptured aneurysm of his left arteriovenous dialysis fistula. He also had a history of multiple tunneled dialysis catheters placed, the most recent being 7 months prior. Computed tomography of the chest was obtained as part of the workup.
Diagnosis
2
Computed tomography of the chest revealed an incidental intravascular retained catheter fragment located in his right pulmonary artery (Fig). Interventional radiology was consulted for the evaluation and removal of the foreign body. Retained catheter fragments from venous access can result in complications including arrythmias, infection, and death.1 In our case, a chest x-ray from 1 month prior did not show evidence of a retained foreign body despite his most recent intravascular procedure occurring 7 months prior. Up to 11.6% of patients living with retained foreign bodies are asymptomatic and have been identified incidentally.1 Percutaneous approaches to intravascular foreign bodies appear to be the primary method of removal.2^,^3 This case highlights the importance of examining guidewires and catheters placed intravascularly to ensure that they are intact before placement and after removal, as this can reduce delayed adverse procedural outcomes.FigureThe image shows multiple views of a retained catheter in the right pulmonary artery extending into the right middle lobar artery. Arrows point to the retained catheter. (A) Coronal view. (B) Sagittal view. (C) Transverse view. (D) Image of the catheter after retrieval by Interventional Radiology.
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Surov A.Wienke A.Carter J.M.Intravascular embolization of venous catheter--causes, clinical signs, and management: a systematic review JPEN J Parenter Enteral Nutr 33620096776851967530110.1177/0148607109335121 · doi ↗ · pubmed ↗
- 2Gabelmann A.Kramer S.Gorich J.Percutaneous retrieval of lost or misplaced intravascular objects AJR Am J Roentgenol 17662001150915131137322110.2214/ajr.176.6.1761509 · doi ↗ · pubmed ↗
- 3Yen H.J.Hwang B.Lee P.C.Meng C.C.Transcatheter retrieval of different types of central venous catheter fragment: experience in 13 cases Angiology 57320063473531670319510.1177/000331970605700311 · doi ↗ · pubmed ↗