Bronchial Dieulafoy: Diagnostic Utility of Endobronchial Ultrasound
Chee Kiang Phua, Chee Kiang Tay, Carrie Kah Lai Leong

TL;DR
This paper discusses how endobronchial ultrasound helps diagnose bronchial Dieulafoy, a condition that can look like a tumor and cause dangerous bleeding if biopsied.
Contribution
The paper demonstrates the novel use of EBUS in safely diagnosing bronchial Dieulafoy and avoiding risky procedures.
Findings
EBUS confirmed the vascular nature of a bronchial Dieulafoy lesion.
EBUS can prevent life-threatening complications from unnecessary biopsies.
Bronchial Dieulafoy can mimic endobronchial tumors on bronchoscopy.
Abstract
We report a case of bronchial Dieulafoy presenting with haemoptysis, initially resembling an endobronchial tumour on bronchoscopy. This case highlights the critical role of EBUS in the assessment of suspicious endobronchial lesions and in preventing potentially life‐threatening complications from inadvertent biopsy. Bronchial Dieulafoy can mimic an endobronchial tumour and pose a risk of life‐threatening bleeding if biopsied. Endobronchial ultrasound (EBUS) confirmed the vascular nature of the lesion, guiding safe and effective management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
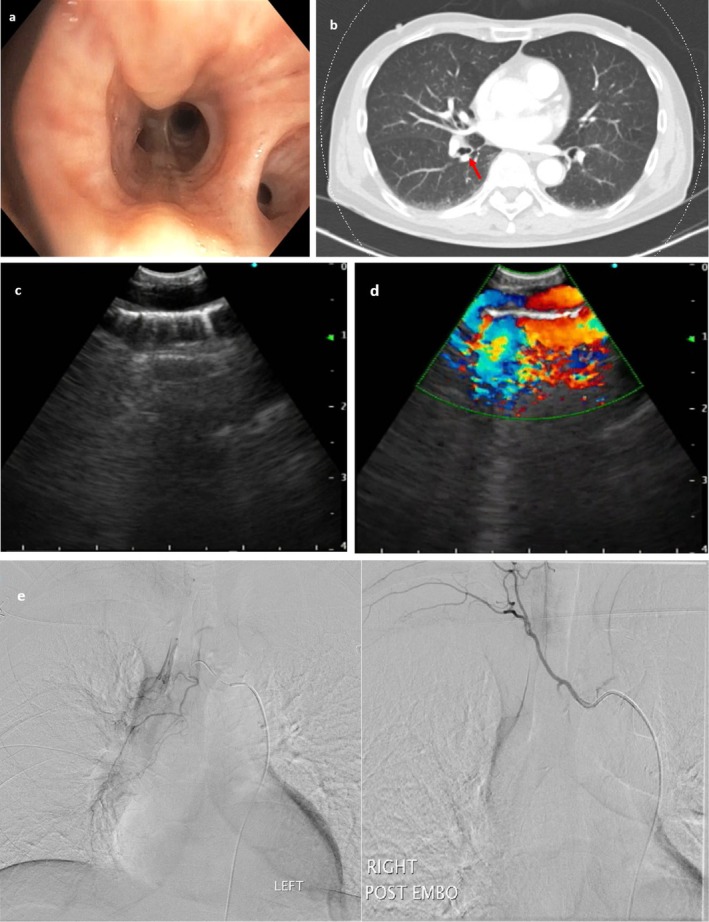 Figure 1
Figure 1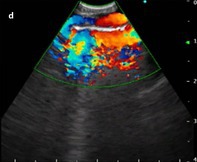 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Vascular Anomalies and Treatments · Dysphagia Assessment and Management
A 63‐year‐old male, chronic smoker, presented with intermittent episodes of haemoptysis for several days. Six months prior, he had similar episodes evaluated with chest computed tomography (CT) and nasoendoscopy, which were unremarkable. Flexible bronchoscopy performed 2 days after the haemoptysis episodes revealed a non‐pulsatile tubular endobronchial lesion at the right lower lobe anterior segment with no visible stigmata of recent bleeding (Figure 1a). Differentials included an endobronchial tumour versus bronchial Dieulafoy. A CT thoracic angiogram was not able to detect any abnormalities (Figure 1b). Due to concerns of airway bleeding, endobronchial ultrasound (EBUS) examination was performed via rigid bronchoscopy with view of sampling. Convex EBUS revealed a linear anechoic lesion (Figure 1c; Video 1) with arterial pulsation on colour doppler (Figure 1d). Radial EBUS also confirmed an anechoic lesion (Video 2). Based on these findings, a diagnosis of bronchial Dieulafoy was made and he successfully underwent bronchial angioembolization with resolution of haemoptysis (Figure 1e). Bronchial Dieulafoy is a rare cause of haemoptysis, and it can be easily misdiagnosed as an endobronchial tumour during bronchoscopy [1]. Convex EBUS uses a specialised bronchoscope equipped with an ultrasound transducer, whilst radial EBUS employs a flexible catheter with a rotating transducer, both allowing immediate confirmation of the diagnosis and averting a biopsy which can lead to catastrophic airway bleeding [1, 2].
Author Contributions
C.K.P. initiated the idea for manuscript submission and prepared the final draft. C.K.T. and C.K.L.L. acquired the clinical data. All authors have read and approved the final manuscript.
Consent
The authors declare that written informed consent was obtained for the publication of this manuscript and accompanying images and attest that the form used to obtain consent from the patient complies with the Journal requirements as outlined in the author guidelines.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1X. Qian , Q. Du , N. Wei , M. Wang , H. Wang , and Y. Tang , “Bronchial Dieulafoy's Disease: A Retrospective Analysis of 73 Cases,” BMC Pulmonary Medicine 19, no. 1 (2019): 104, 10.1186/s 12890-019-0863-1.31170962 PMC 6555732 · doi ↗ · pubmed ↗
- 2O. Ganganah , S. Guo , M. Chiniah , S. K. Sah , and J. Wu , “Endobronchial Ultrasound and Bronchial Artery Embolization for Dieulafoy's Disease of the Bronchus in a Teenager: A Case Report,” Respiratory Medicine Case Reports 27, no. 16 (2015): 20–23, 10.1016/j.rmcr.2015.04.007.PMC 468190026744645 · doi ↗ · pubmed ↗