Prevalence of vaginal laxity in primiparous women six months after birth
Marina Resende Godoy, Gláucia Miranda Varella Pereira, Clara Vale Viegas, Marilene Vale de Castro Monteiro

TL;DR
This study found that 8% of first-time mothers experienced vaginal laxity six months after childbirth, with urinary and sexual symptoms linked to its occurrence.
Contribution
The study provides new insights into the prevalence and risk factors for vaginal laxity in primiparous women postpartum.
Findings
The prevalence of vaginal laxity was 8% in the studied population.
Urgency urinary incontinence and coital incontinence were strongly associated with vaginal laxity.
Higher scores on vaginal symptom and urinary incontinence questionnaires increased the risk of vaginal laxity.
Abstract
To assess the prevalence of VL in primiparous women undergoing vaginal birth or caesarean section; and its association with obstetric, urinary, intestinal and sexual factors for its occurrence. This is a cross-sectional study carried out between July 2021 and January 2023. Primiparous women who underwent vaginal birth or caesarean section without complaints of VL during pregnancy were included. Clinical and obstetric data were collected and participants completed questionnaires on the impact of urinary incontinence (ICIQ-SF), vaginal symptoms (ICIQ-VS) and sexual distress (FSDS-R) at recruitment and six-months postpartum. Univariate and multivariate logistic regression was performed, considering VL as the outcome and p=0.05. One hundred participants were included for data analysis. The prevalence of VL was 8%. In the univariate analysis, SUI, urgency urinary incontinence (UUI), coital…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
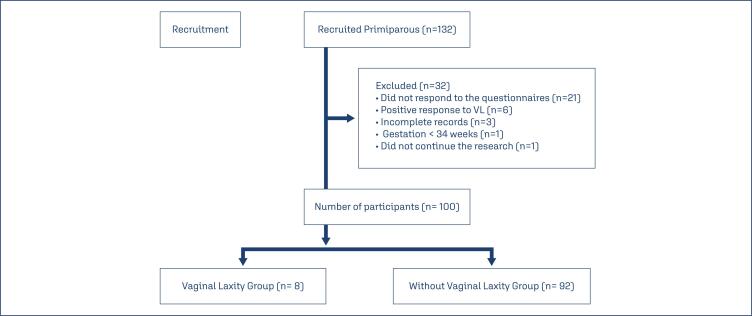 Figure 1
Figure 1| Variables | Vaginal laxity (n=8) | Without vaginal laxity (n=92) | p-value | |
|---|---|---|---|---|
| Age (mean ± SD) | 24.6 ± 6,3 | 26.1 ± 6,0 | 0.437 | |
| Education | 0.296 | |||
| Primary | 1(12.50) | 2(2.17) | ||
| Secondary | 6(75) | 76(82.61) | ||
| Tertiary | 1(12.0) | 14(15.22) | ||
| Body Mass Index | 0.651 | |||
| Normal | 1(12.50) | 23(25) | ||
| Overweight | 3(37.50) | 35(38.04) | ||
| Obesity | 4(55.50) | 34(36.96) | ||
| Gestation | 0.763 | |||
| Single gestation | 8(100) | 89(96.74) | ||
| Twin gestation | 0 | 3 (3.26) | ||
| Type of birth | 0.062 | |||
| Vaginal Delivery | 7(87,50) | 49(53.26) | ||
| C-section | 1(1) | 43(46.74) | ||
| Gestational age / Mean ± SD | 38.5 ± 1.9 | 38.4 ± 1.4 | 0.768 | |
| Newborn weight / Mean ± SD* | 3,020 ± 594.2 | 3,165 ± 459.9 | 0.237 | |
| Newborn weight / Grams* | 0.653 | |||
| < 2500 | 1(12.50) | 12(13.05) | ||
| 2500 – 3499 | 6(75) | 62(67.39) | ||
| 3500 – 4000 | 0 | 16(17.39) | ||
| > 4000 | 0 | 2(2.17) | ||
| Forceps | 0 | 3(3.26) | 0.598 | |
| Vacuum extraction | 0 | 1(1.09) | 0.764 | |
| Position during the second stage of labour* | 0.473 | |||
| Not applied (C-section) | 1(12.50) | 43(46.74) | ||
| Lithotomy | 1(12.50) | 12(13.05) | ||
| Sitting position | 2(25) | 15(16.30) | ||
| Squatting position | 3(37.50) | 20(21.74) | ||
| Hands-and-knees position | - | 2(2.17) | ||
| Duration of the second stage of labour (mean ± SD) | 39.4 ± 40.6 | 60.9 ± 49.4 | 0.343 | |
| Oxytocin * | 3(37.50) | 46(50) | 0.498 | |
| Spinal anaesthesia | 1(12.50) | 42(45.65) | 0.070 | |
| Epidural anaesthesia | 4(50) | 38(41.30) | 0.625 | |
| Episiotomy | 2(25) | 6(6.52) | 0.070 | |
| Perineal laceration | 0.383 | |||
| 0 | 2(25) | 48(52.17) | ||
| 1 | 3(37.50) | 20(21.74) | ||
| 2 | 3(37.50) | 20(21.74) | ||
| 3 | 0 | 4(4.35) | ||
| Shoulder dystocia | 1(12.50) | 1(1.09) | 0.029 | |
| Stress urinary incontinence | 5(62.50) | 42(45.65) | 0.357 | |
| Urge urinary incontinence | 1(12.50) | 15(16.30) | 0.760 | |
| Urgency | 3(37.50) | 42(45.65) | 0.661 | |
| Nocturia | 7(87.50) | 88(95.65) | 0.321 | |
| Constipation | 6(75) | 65(70.65) | 0.675 | |
| Anal incontinence | 1(12.50) | 7(7.61) | 0.640 | |
| Dyspareunia | 2(25) | 17(18.48) | 0.613 | |
| Sexual activity | 8(100) | 60(65.22) | 0.988 | |
| Coital incontinence | 1(12.50) | 2(2.17) | <0.001 | |
| Variables | Initial recruitment (n) | 6 months postpartum (n) | p-value | |
|---|---|---|---|---|
| Urinary symptoms | ||||
| Stress urinary incontinence | 47 | 10 | <0.001 | |
| Use of absorbent pads | 14 | 12 | 0.824 | |
| Urgency | 45 | 10 | <0.001 | |
| Urge urinary incontinence | 16 | 9 | 0.144 | |
| Urinary frequency | <0.001 | |||
| < 8x | 20 | 28 | ||
| > 8x | 80 | 72 | ||
| Nocturia | 95 | 67 | <0.001 | |
| Nocturnal enuresis | 7.1 | 4 | 0.508 | |
| Dysuria | 5 | 5 | 0.999 | |
| Suprapubic pain with repletion | 26 | 9 | 0.002 | |
| Straining to urinate | 10 | 11 | 0.999 | |
| Feeling of incomplete emptying | 49 | 22 | <0.001 | |
| Intermittent stream | 20 | 15 | 0.424 | |
| History of urinary tract infection | 33 | 11 | <0.001 | |
| Bowel symptoms | ||||
| Bowel habit | 0.052 | |||
| Regular | 19 | 30 | ||
| Constipation | 81 | 70 | ||
| Anal incontinence | 8 | 18 | 0.064 | |
| Sexual symptoms | ||||
| Coital incontinence/orgasm | 0 | 3 | 0.500 | |
| Dyspareunia | 19 | 21 | 0.839 | |
| Sexual activity | 0.230 | |||
| No | 38 | 31 | ||
| Yes | 62 | 69 | ||
| Questionnaires | Initial recruitment (mean ± SD) | 6 months postpartum (mean ± SD) | p-value | |
|---|---|---|---|---|
| ICIQ-SF | 3.18 ± 3.89 | 1.41 ± 3.76 | <0.001 | |
| ICIQ-VS | ||||
| Vaginal Symptoms | 6.61 ± 4.87 | 4.99 ± 5.73 | 0.002 | |
| Sexual Matters | 6.03 ±11.22 | 5.02 ± 14.74 | 0.117 | |
| Quality of life | 2.02 ± 2.76 | 1.71 ± 2.94 | 0.204 | |
| FSDS-R | 4.11 ± 6.60 | 5.35 ± 10.77 | 0.722 | |
| Variables | Univariate analysis | p-value | Multivariate analysis | p-value |
|---|---|---|---|---|
| Childbirth | ||||
| Caesarean section | 0.14 (0.02 – 1.16) | 0.069 | ||
| Perineal laceration | ||||
| Grade II | 5.05 (0.85 –29.92) | 0.074 | ||
| Second Stage of labour | ||||
| Sitting position | 9.21 (0.89 –95.86) | 0.063 | ||
| Stress urinary incontinence | 11.33 (2.40 – 53.60) | 0.002 | ||
| Urge urinary incontinence | 7.08 (1.41 – 35.59) | 0.017 | 10.50 (1.90 – 58.10) | 0.007 |
| Coital incontinence | 25.71 (2,07 – 319.80) | 0.012 | 42.00 (3.11 – 566.38) | 0.005 |
| Constipation | 5.58 (1.29 – 24.10) | 0.021 | ||
| ICIQ-VS | ||||
| Vaginal symptoms | 1.31 (1.11 – 1.55) | 0.001 | 1.32 (1.05 – 1.66) | 0.015 |
| Sexual matters | 1.04 (1.00 – 1.09) | 0.031 | ||
| Quality of life | 1.31 (1.08 – 1.60) | 0.007 | ||
| FSDS-R | 1.05 (1.00 – 1.09) | 0.036 | ||
| ICIQ-SF | 1.33 (1.14 – 1.56) | 0.001 | 1.25 (1.02 – 1.54) | 0.028 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic floor disorders treatments · Anorectal Disease Treatments and Outcomes · Urinary Bladder and Prostate Research
Introduction
Vaginal laxity (VL) is a common postpartum complaint,^(1,2)^ and is characterized by excessive vaginal looseness perceived by the patient.^(3)^
According to the literature, its prevalence can vary between 2% and 48%.^(1,4,5)^ VL appears to be associated with changes in the integrity of vaginal and muscular tissue due to pregnancy, childbirth and ageing, resulting in greater distension of the pelvic floor muscles and opening of the vaginal introitus.^(6,7)^ Excessive distension of the pelvic floor muscles contributes to the occurrence of microtraumas and avulsion of the levator ani muscle, leading to an increase in the size of the genital hiatus.^(8)^ Such changes may result in reduced sensation during penetration, orgasmic dysfunction, and reduced sexual satisfaction.^(5,7,9)^ Reduced sensation during sexual intercourse may be related to damage to the perineal body, vaginal introitus, nerves, and connective tissue.^(5)^
VL is common in young women and after vaginal birth.^(1,4)^ Caesarean section appears to be a protective factor for the symptom.^(4)^ The symptom of VL pre-existing during pregnancy does not seem to worsen after birth, but women who had a vaginal birth had a higher prevalence of VL compared to those who had a caesarean section.^(10)^ When compared to nulliparous women, primiparous women were five times more likely to report VL and women who had three or more vaginal births were seven times more likely to report VL.^(5,11)^
Although there is currently a growing interest in treatment options for VL, its pathophysiology is still poorly understood.^(12–14)^ According to 83% of the 416 physicians members of the International Urogynecological Association (IUGA) surveyed, the symptom of VL is underreported and presents itself as an uncomfortable condition that negatively affects the sexual life and affective relationships of their patients.^(14)^
Considering that the mechanism of occurrence of VL is little studied, further studies are needed on its association with the type of delivery and the first delivery. It appears that complaints of VL are more prevalent among women who have experienced vaginal childbirth, with the first delivery being the primary contributing factor. This observation aligns with previous research indicating that the most significant adverse effects on the pelvic floor occur during the first vaginal birth, while subsequent deliveries have a comparatively lesser impact.^(15)^ A study examined the influence of first and second deliveries on levator ani muscle (LAM) avulsion and its association with symptoms of pelvic floor dysfunction. Their findings revealed that the first delivery poses the greatest risk for LAM avulsion, whereas the second may exacerbate existing injuries without causing new avulsions.^(16)^ To date, there are no studies that address VL exclusively in primiparous women. Thus, the objective of this study was to assess the prevalence of VL in primiparous women undergoing vaginal or caesarean birth; and its association with risk factors (clinical, obstetric), in addition to urinary, intestinal and sexual symptoms for its occurrence at six months post-partum.
Methods
This is a cross-sectional observational study, carried out between July 26, 2021, and January 31, 2023, at a tertiary hospital. We followed the STROBE recommendations for observational studies.^(17)^
Primiparous women, aged 18 years or older, who retrospectively reported an absence of symptoms related to vaginal laxity during pregnancy in the immediate postpartum period, and who underwent either vaginal delivery or cesarean section between July 2021 and January 2023, were included in the study. Participant selection was conducted weekly in the maternity ward. The absence of VL was considered when participants responded negatively to a direct question regarding their perception of VL (yes/no) and negative response to question 4a (Do you feel that your vagina is very loose or lose?) from the International Consultation on Incontinence Questionnaire - Vaginal Symptoms (ICIQ-VS) regarding the gestational period.^(18)^ Women were excluded if they reported VL during pregnancy, had a history of vaginal or caesarean birth, underwent vaginal surgery before pregnancy, had a gestational age of less than 34 weeks, had neurological disorders, experienced cognitive impairments or were unable to read or understand Brazilian Portuguese, or failed to respond to the questionnaires six months postpartum.
Participants who met the inclusion criteria were approached in person by a single researcher in the hospital room during the immediate postpartum period until up to 10 days after delivery. The researcher ensured that all participants could answer the questions accurately. Sociodemographic, clinical, and obstetric data were collected from medical records. Urinary, vaginal, and sexual symptoms were assessed using self-administered questionnaires validated for Brazilian Portuguese. These questionnaires were completed in person in the hospital room during the immediate postpartum period, gathering responses about the gestational period as baseline assessment. The six-month assessment was conducted via telephone or email six months after delivery.
The International Consultation on Incontinence Questionnaire - Short Form (ICIQ-SF) is a questionnaire that qualifies urinary loss and the impact of urinary incontinence (UI) on quality of life with a score ranging from 0 to 21. A score of zero means no urinary loss and no impact on quality of life.^(19)^ The ICIQ-VS assesses the severity of vaginal symptoms, the impact on sexual function and quality of life. The higher the score, the worse the severity of the symptoms.^(18)^ The Female Sexual Distress Scale-Revised (FSDS-R) is a questionnaire that aims to assess sexual distress with a maximum score of 53 and the higher the total score, the greater the sexual distress.^(2)^
To calculate the sample size, the proportion estimate was used in a descriptive study^(1)^ with a categorical qualitative variable, setting the alpha significance level or type I error at 5% (alpha = 0.05) (or 95% confidence interval), the sampling error at 10% (d = 0.10) and the sample power (1-beta) at 80%. A sample size of n = 109 participants was obtained for the present study. The sample calculation was performed by the SAS System for Windows (Statistical Analysis System), version 9.4. SAS Institute Inc, 2002-2012, Cary, NC, USA.
Continuous variables were presented as mean, standard deviation, and median, with minimum and maximum values reported. Categorical variables were presented according to their absolute and relative frequency. To estimate the association between the predictor variables and the outcomes of interest, the Chi-Square test was used for categorical variables and the Mann-Whitney test for continuous variables. Univariate and multivariate logistic regression models were used to estimate cofactor-adjusted odds ratios with 95% confidence intervals. In all statistical calculations, the significance level was 0.05. SPSS® 22.0 software was used for the analysis.
The present study was approved by the Research Ethics Committee (4.865.026) and all participants signed the Informed Consent Form.
Results
During the period from July 2021 to January 2023, 132 primiparous participants were recruited for data analysis. Thirty-two participants were excluded (21 did not respond to the questionnaires; six responded positively to VL; three were due to incomplete medical records; one had a gestation of less than 34 weeks and one did not want to continue in the research). Of the 100 participants with complete data included in the final analysis, eight reported VL and 92 denied this symptom (Figure 1).
Flowchart of primiparous women recruited for the study
The prevalence of VL after childbirth in the present study was 8%. The sociodemographic characteristics of the participants are shown in table 1. The average age in participants with and without VL were 24.6 ± 6.3 and 26.1 ± 6.0, and the average weight of the newborns was 3020g ± 594.32 and 3165gr ± 459.9, respectively. Regarding obstetric clinical data, only shoulder dystocia and coital incontinence were statistically different between participants, despite the single occurrence in the VL group. Stress urinary incontinence (SUI) was more frequent in participants with VL (62.50%) compared to participants without VL (45.65%). In the same evaluation period, 100% of participants with VL were sexually active compared with only 65.22% of participants without VL (Table 1).
Urinary, bowel and sexual data were collected in two periods, both at initial recruitment and six months postpartum. The majority of urinary symptoms investigated improved six-months after birth, with statistical significance between the two periods. Anal incontinence, coital incontinence and dyspareunia worsened six-months postpartum, but there was no statistically significant difference (Table 2).
The total score of the ICIQ-SF questionnaire decreased significantly (p<0.001) six months after birth when compared to initial recruitment, indicating an improvement in the symptoms of UI and the impact on quality of life. In the vaginal symptoms score of the ICIQ-VS questionnaire, a statistically significant difference was found for the same period (p=0.002). The other ICIQ-VS scores for sexual issues (p=0.117) and quality of life (p=0.204) also decreased, suggesting an improvement in symptoms, but did not reach a statistically significant difference. The total score of the FSDS-R questionnaire (p=0.722) was higher six-months after birth, signalling a worsening of sexual distress during this period, but there was no statistically significant difference (Table 3).
The clinical data SUI, urgency urinary incontinence (UUI), coital incontinence and intestinal constipation were associated with VL symptoms in the univariate analysis. However, only UUI and coital incontinence remained associated with VL in the multivariate-analysis (Table 4). Regarding the questionnaire scores, the ICIQ-VS, the FSDS-R and the ICIQ-SF increased the risk of VL in the participants by one, in the univariate analysis. However, only the ICIQ-VS (vaginal symptoms domain) and the ICIQ-SF remained associated with VL in the multivariate-analysis, OR 1.32 and OR 1.25, respectively.
Discussion
VL remains little investigated in the literature, being a complaint that negatively affects women's sexual function and quality of life.^(12,13)^ In the present study, the prevalence of VL in women after their first birth was 8%. The symptom of UI and the impact on quality of life assessed by the ICIQ-SF, as well as the vaginal symptoms assessed by the ICIQ-VS improved six-months after delivery. In the univariate analysis, the scores of the ICIQ-SF, ICIQ-VS and FSDS-R questionnaires, in addition to clinical data such as SUI, UUI, coital incontinence and intestinal constipation six-months postpartum were associated with VL symptoms. However, only the ICIQ-VS vaginal symptoms domain, the ICIQ-SF score, UUI and coital incontinence maintained an association with the VL symptom in the multivariate-analysis.
Regarding clinical/obstetric data, only shoulder dystocia (p=0.029) and coital incontinence (p<0.001) were statistically different between the participants. Packet et al.,^(20)^ identified that shoulder dystocia was one of the predictive factors for obstetric injury to the anal sphincter in primiparous women. This type of injury could have some implications for the integrity of the PFM and be related to VL. However, we found no association between VL and shoulder dystocia and coital incontinence.^(20)^ Coital incontinence appears to be a multifactorial, underreported symptom, associated with the severity of SUI and with a negative effect on quality of life and female sexual function.^(21)^
Most urinary symptoms and ICIQ-SF scores improved six-months postpartum. This can be explained by the physiological changes during pregnancy that imply a greater occurrence of urinary dysfunction during this period compared to postpartum.^(22–24)^
It is worth mentioning that the presence of urinary incontinence before pregnancy is the predictive factor for UI during pregnancy, in addition to increasing the chances of developing UI in the postpartum period by up to three times.^(25,26)^ However, we did not evaluate urinary complaints in the period before pregnancy. Leeman et al.^(27)^ found a higher number of reports of UI in the third trimester of pregnancy (74.1%) compared to six-months postpartum in primiparous women (59.8%) and van Delft et al.^(28)^ revealed fewer UI symptoms three months postpartum (64%) compared to the third gestational trimester (74%). Stress urinary incontinence was the most prevalent type of UI in the present study (47%), similar to other studies.^(22,24,25,28)^ The ICIQ-SF score and the UUI symptom remained associated with the VL symptom in our multivariate-analysis, similar to the study by Campbell et al.^(5)^ and Pereira et al.^(29)^ The findings of Dietz et al.^(1)^ and Talab et al.^(4)^ contrast with ours, since VL was not associated with any type of UI investigated. To date, we have not found studies that investigated the association between coital incontinence and the symptom of VL. Although the multivariate-analysis was statistically significant for these variables, the small number of VL cases in this sample does not allow these findings to be extended to all women with VL.
Obstetric data such as type of delivery (caesarean section), laceration (grade 2) and position of the expulsion (sitting), despite not having reached statistical significance, presented values close to 5% and clinical relevance for our research. Similarly to the study by Talab et al.,^(4)^ caesarean section (p=0.069) when compared to vaginal delivery, appeared to be a protective factor against the symptom of VL. Perineal trauma is common during vaginal birth, reaching a prevalence of 85%, with primiparity being a risk factor for severe lacerations (grades 3 and 4).^(30)^ However, only four participants without VL presented grade III tears, with grade I and II tears (mild lacerations) being more frequent in our sample. In participants with VL, grade II laceration had a significance level close to 5% (p=0.074). This may suggest that damage to the integrity of the PFM, caused by grade II lacerations, contributes to the presence of the VL symptom after the first birth. However, we did not objectively assess the presence or absence of injury to the levator ani muscle.
The position during the expulsion period that came closest to the significance value of p=0.05 was the sitting position (p=0.063). In the study by Reis et al.,^(31)^ the sitting position was the most used and no association was established between this position and the symptom of VL.
The presence of vaginal symptoms assessed by the ICIQ-VS in this study significantly decreased six-months after birth but increased the chance of developing VL by one. The study by McDonald et al.^(32)^ contrasts with our findings due to the increase in vaginal symptoms in primiparous women in the postpartum period due to lack of lubrication (29.6% during pregnancy and 48.2% six-months postpartum); vaginal tightness (21.2% during pregnancy and 34.1% six-months postpartum). O’Malley et al.^(33)^ evaluated vaginal symptoms such as vaginal tightness, lubrication and VL in primiparous women at the beginning of pregnancy and six-months after birth and also found worsening in the second stage. However, the authors did not use a validated questionnaire. Another study that differs from our results is by Abdool et al.,^(34)^ who evaluated 83 primiparous South African women in the third trimester and three to six-months after giving birth to determine the impact of giving birth on PFM. ICIQ-VS vaginal symptom scores for VL, dry vagina, interference with sexual life and quality of life were significantly higher in the postpartum period.
Despite not reaching a statistically significant difference between participants, the total FSDS-R score worsened six-months after birth. First-time women can take three to eighteen months to improve pelvic floor disorders that negatively affect sexual health.^(35)^ In the study by Witting et al.,^(36)^ primiparous women had lower sexual satisfaction and greater intensity of pain during sexual intercourse when compared to multiparous women. Pereira et al.^(2)^ found higher scores on the FSDS-R in women with VL when compared to those without VL. In another study, the symptom of VL was predictive of sexual distress assessed by the FSDS-R in women with and without breast cancer.^(6)^
Approximately 31% of participants had not resumed sexual activity six months after delivery. The low prevalence of VL in primiparous women in our study may have been influenced by this rate, since the symptom of VL is perceived during sexual intercourse.^(1,4,5)^ However, to date, we have not found any study in the literature that evaluated VL in a population exclusively of primiparous women as a primary outcome, based on a validated questionnaire and its associations with sexual, urinary, intestinal symptoms and obstetric data.
This study has limitations. First, participants were not assessed for the presence of symptoms prior to pregnancy. Additionally, the maternity hospital where the research was conducted serves multiple cities within the state, making it unfeasible to contact participants during the gestational period; thus, contact was only possible upon admission for delivery. Furthermore, key factors such as the impact of breastfeeding on sexual function, the nature of sexual activity, and the reasons for the absence of sexual relations were not evaluated. The diagnosis of VL was based on self-reported data obtained through direct questioning and a validated questionnaire. However, no physical examinations or ultrasound assessments were performed, which may have affected diagnostic accuracy. Moreover, the retrospective nature of the question regarding the presence or absence of VL during pregnancy at the time of initial recruitment introduces a potential recall bias. Additionally, the study design does not allow for the establishment of causal relationships. Another limitation is the small number of participants with VL (n=8), which restricts the generalizability of the findings and increases the risk of Type II errors. Therefore, the results should be interpreted with caution. Future studies should aim for a larger sample size and a longitudinal design to provide a better understanding of the role of pregnancy and childbirth in the development of VL.
Despite these limitations, the strengths of our study include the assessment of the prevalence of an underreported symptom, specifically among primiparous women without a history of this complaint, thereby mitigating the confounding effects associated with parity. Additionally, the study successfully identified associations between VL and symptoms of pelvic floor dysfunction—specifically urinary, vaginal, and sexual symptoms—using validated questionnaires.
Conclusion
The prevalence of VL, in this sample of primiparous women, was lower than that reported in other studies and showed an association with the occurrence of vaginal symptoms, urgency urinary incontinence and coital incontinence, six-months postpartum.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dietz HP Stankiewicz M Atan IK Ferreira CW Socha M Vaginal laxity: what does this symptom mean?Int Urogynecol J 201829572372810.1007/s 00192-017-3426-028762179 · doi ↗ · pubmed ↗
- 2Pereira GM Juliato CR Gomes DA de Souza Beltramini T de Castro Monteiro MV Brito LG Cross-cultural adaptation and validation of the Brazilian Portuguese version of the Female Sexual Distress Scale-Revised questionnaire for women with vaginal laxity Int Urogynecol J 202233113163317010.1007/s 00192-022-05227-035588319 PMC 9118812 · doi ↗ · pubmed ↗
- 3Haylen BT Maher CF Barber MD Camargo S Dandolu V Digesu A An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint report on the terminology for female pelvic organ prolapse (POP)Int Urogynecol J 201627216519410.1007/s 00192-015-2932-126755051 · doi ↗ · pubmed ↗
- 4Talab S Al-Badr A Al Kusayer GM Dawood A Bazi T Correlates of vaginal laxity symptoms in women attending a urogynecology clinic in Saudi Arabia Int J Gynaecol Obstet 2019145327828210.1002/ijgo.1281030924525 PMC 7027493 · doi ↗ · pubmed ↗
- 5Campbell P Krychman M Gray T Vickers H Money-Taylor J Li W Self-reported vaginal laxity-prevalence, impact, and associated symptoms in women attending a urogynecology clinic J Sex Med 201815111515151710.1016/j.jsxm.2018.08.01530327263 · doi ↗ · pubmed ↗
- 6Qureshi AA Sharma K Thornton M Myckatyn TM Tenenbaum MM Vaginal laxity, sexual distress, and sexual dysfunction: a cross-sectional study in a plastic surgery practice Aesthetic Surg J 201838887388010.1093/asj/sjx 25529370358 · doi ↗ · pubmed ↗
- 7Krychman M Rowan CG Allan BB Durbin S Yacoubian A Wilkerson D Effect of single-session, cryogen-cooled monopolar radiofrequency therapy on sexual function in women with vaginal laxity: The VIVEVE I Trial J Womens Health (Larchmt)20182729730410.1089/jwh.2017.633529182498 PMC 5865245 · doi ↗ · pubmed ↗
- 8Manzini C Friedman T Turel F Dietz HP Vaginal laxity: which measure of levator ani distensibility is most predictive?Ultrasound Obstet Gynecol 202055568368710.1002/uog.2187331568590 PMC 7417815 · doi ↗ · pubmed ↗