Methadone for critically ill patients under mechanical ventilation in the intensive care unit: a systematic review
Sérgio Martins Pereira, Megan Abbott, João Francisco Figueiredo Marcondes Ferraz, Akash Goel, Andrea Rigamonti, Charmaine de Castro, Lisa Burry, Airton Leonardo de Oliveira Manoel, Michael Chaim Sklar

TL;DR
This review explores methadone's use in ICU patients on ventilators, suggesting it may improve outcomes like ventilator-free days, though evidence is limited.
Contribution
The study is the first systematic review evaluating methadone's effectiveness in mechanically ventilated ICU patients.
Findings
Methadone was associated with more ventilator-free days and shorter weaning times compared to non-methadone groups.
The quality of evidence was low, and most studies had high risks of bias.
Patient populations included trauma, burn, and opioid-related conditions.
Abstract
Pain may pose significant challenges in the intensive care unit, especially in mechanically ventilated patients. Methadone has recently emerged as an alternative option for eliciting acute analgesia. In this systematic review, we evaluated the use of methadone in mechanically ventilated patients in the intensive care unit. We searched MEDLINE, EMBASE, Wiley's Cochrane Library, CINAHL, PubMed (non-MEDLINE), Scopus, and LILACS databases from inception to January 24th, 2025. Eligible studies included randomized controlled trials and observational studies that compared the use of methadone to the standard of care or to other analgosedation strategies in mechanically ventilated patients in the intensive care unit. The primary outcome was the duration of mechanical ventilation. The secondary outcomes included opioid-associated adverse effects and scores regarding pain, agitation, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
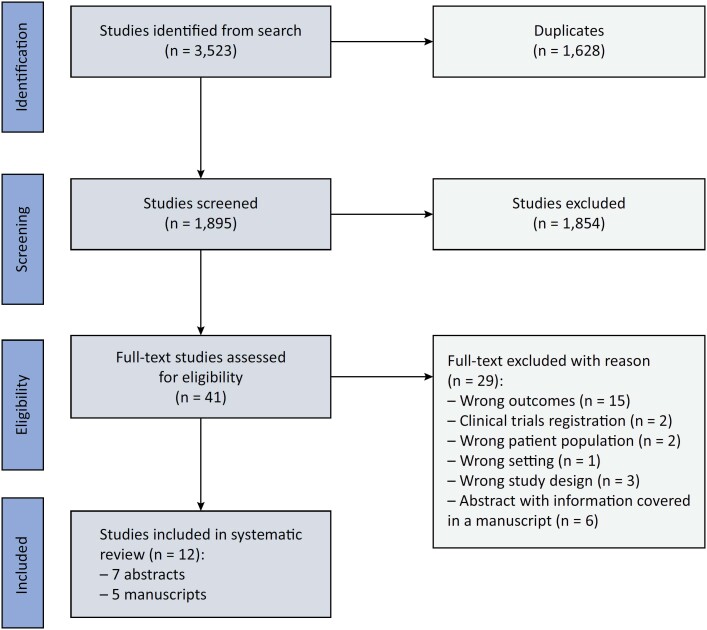 Figure 1
Figure 1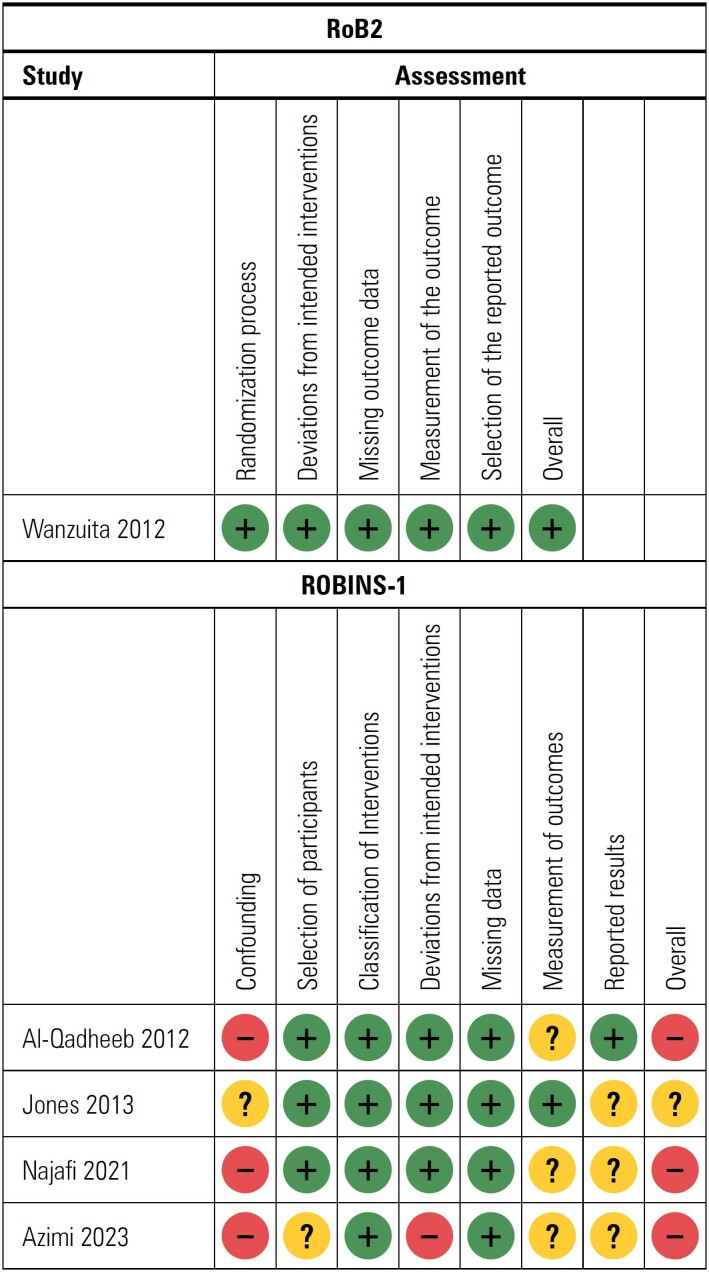 Figure 2
Figure 2| Author, journal and year | Study type | Population | Control | Intervention | Outcomes |
|---|---|---|---|---|---|
| Wanzuita et al.( | Randomized controlled trial | Patients weaning from MV who had been using fentanyl for more than | Placebo | Methadone PO | 1) Probability of successful weaning by the fifth day was higher in methadone patients: HR: 2.64 (1.22 to 5.69); p < 0.02 |
| Kowalski et al.( | Retrospective cohort | MV for 48 hours | Immediate release opioids | Methadone | 1) Time to wean continuous infusion: 57.5 |
| Jones et al. ( | Retrospective cohort with propensity match score | Patients who received methadone within 4 days of intubation and who remained ventilated for | No methadone | Early methadone | 1) Ventilator-free days: 12.6 |
| Zavala et al.( | Retrospective cohort | Adult patients admitted to the burn center for initial management who required MV for at least 48 hours, without prior methadone use and total body surface area > 5% | No methadone | Methadone | 1) Ventilator-free days: 15 |
| Maghsoudi( | Randomized pilot study | Inhalant opium-addicted ICU patients | Opium tincture | Methadone | 1) BPS: benefit in opium tincture group; |
| Wanzuita et al.( | Prospective cohort | Patients fulfilling criteria for weaning from MV | Enteral placebo + IV fentanyl | Enteral methadone + IV placebo | 1) Anticipation of extubation: HR: 1.44 |
| Bonnin et al.( | Retrospective cohort | Patients on continuous opioid infusion for a minimum of 24 hours | No methadone | Enteral methadone | 1) Cumulative dose in MME: |
| Wanzuita et al.( | Randomized controlled trial | Patients under high risk for fentanyl abstinence syndrome (continuous fentanyl > 5 days or more than 5mcg/kg/hour during 12 hours) | Enteral placebo + IV fentanyl | Enteral methadone + IV placebo | 1) ICU LOS: 27 (13) |
| Jones et al.( | Retrospective cohort with propensity match score | Patients between 18 and 89 years of age who required ventilation for at least 2 days | Standard of care | Methadone PO/IV | 1) Ventilator-free days: 11.5 |
| Azimi et al.( | Retrospective cohort | Patients who received fentanyl or hydromorphone continuously for ≥ 72 hours | Oxycodone PO | Methadone PO | 1) Time to discontinuation of IV opioid infusions from the initiation of enteral |
| Al-Qadheeb et al.( | Prospective matched cohort 1:2 | Patients without chronic opioid use who received | Standard of care | Methadone PO/IV | 1) Time to fentanyl discontinuation 7.0 (4.9 to 11.5) |
| Najafi et al.( | Prospective controlled pilot study | Opioid-dependent patients admitted to the toxicology ICU after initiation of their withdrawal syndrome | Fentanyl | Methadone | 1) Duration of intubation: 5 [5 - 50] |
| GRADE assessment and risk of bias | ||||||
|---|---|---|---|---|---|---|
| Primary outcome | Group | Outcome measured (source; units) | GRADE | Risk of bias | Overall effect | |
| Intervention | Control | |||||
| Mechanical ventilation-related | 16.5 | 11.5 | Ventilator-free days, days( | Moderate | Moderate | Likely beneficial |
| HR: 1.89 (1.16 to 3.07) | Probability to be weaned from the ventilator, HR( | Moderate | Moderate | Likely beneficial | ||
| HR: 2.64 (1.22 to 5.69) | Probability of successful weaning by the fifth day, HR( | High | Low | Likely beneficial | ||
| HR: 1.52 (0.87 to 2.64) | Probability of early extubation, HR( | High | Low | Likely beneficial | ||
| HR: 2.06 (1.17 to 3.63) | MV weaning time was lower in the methadone group among patients who were successfully weaned( | High | Low | Likely beneficial | ||
| 9 [4 - 17] | 5 [5 - 50] | Duration of intubation, days( | Low | Serious | No effect | |
| ICU outcomes | 88.9% | 67.3% | % of patients discharged alive from ICU( | Moderate | Moderate | Likely beneficial |
| 10 [7 - 14] | 7 [6 - 14] | Duration of ICU stay, days( | Low | Serious | No effect | |
| Other opioid discontinuation | 104.7 ± 79.4 | 158.3 ± 171.2 | IV opioid infusion, hours( | Moderate | Moderate | Likely beneficial |
| 4.5 (3.9 to 5.8) | 7.0 (4.9 to 11.5) | Time to fentanyl discontinuation, days( | Moderate | Moderate | Likely beneficial | |
| HR: 3.8 (1.7 to 8.8) | Odds to discontinue fentanyl after methadone was initiated( | Moderate | Moderate | Likely beneficial | ||
| Opioid withdrawal | 30 [30 - 60] | 120 [45 - 120] | Symptoms after drug administration, minutes( | Low | Serious | No effect |
| 6 [1 - 21] | 6 [4 - 13] | COWS 30 minutes after administration( | Low | Serious | No effect | |
| 2 [1 - 3] | 0 [0 - 3] | COWS 120 minutes after administration( | Low | Serious | No effect | |
| Study, year | Study design | Risk of bias | Inconsistency of results | Indirectness of evidence | Imprecision | Publication bias | Quality of evidence for individual study (n = 1) |
|---|---|---|---|---|---|---|---|
| Wanzuita et al.( | Randomized trial | Low risk | Not serious | Not serious | Not serious | Undetected | High |
| Jones et al.( | Retrospective cohort with propensity match score | Unclear risk | Serious risk | Not serious | Not serious | Undetected | Moderate |
| Azimi et al.( | Retrospective cohort | Unclear risk | Serious risk | Not serious | Not serious | Undetected | Moderate |
| Al-Qadheeb et al.( | Prospective matched cohort | Unclear risk | Serious risk | Not serious | Not serious | Undetected | Moderate |
| Najafi et al.( | Prospective pilot | High risk | Serious risk | Serious risk | Serious | Undetected | Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Anesthesia and Sedative Agents · Respiratory Support and Mechanisms
INTRODUCTION
Pain and discomfort are pervasive challenges encountered in the intensive care unit (ICU).^(1,2)^ In mechanically ventilated patients, inadequate pain management often manifests as psychomotor agitation and patient-ventilator asynchrony,^(3)^ which may be mitigated via careful titration of analgesia and/or sedation.^(3)^ A recent study revealed that moderate to deep sedation significantly prolongs ventilator weaning and leads to adverse outcomes,^(4)^ thus highlighting the need for targeted strategies to address these challenges.
Opioids induce systemic analgesia, anxiolysis, and sedation; additionally, they are commonly administered to ventilated patients^(5,6)^ to manage the discomfort associated with the insertion of an endotracheal tube or the performance of certain procedures. Methadone is a long-acting μ-opioid receptor agonist that exhibits additional agonist activity at the κ- and σ-opioid receptors. In addition to the inhibition of monoamine and catecholamine reuptake, the effect of methadone on the N-methyl-aspartate-D-aspartate (NMDA) receptor has been postulated to elicit analgesia and euphoria while preventing the development of acute opioid tolerance.^(7,8)^ Although potentially beneficial, only one randomized clinical trial (RCT) has evaluated methadone in mechanically ventilated patients in the ICU.^(9)^
Although there is growing adoption of methadone in the operating room setting,^(10,11)^ limited data on other settings exist. Current clinical practice guidelines highlight the importance of addressing the risks of opioid withdrawal and opioid use disorders when managing ICU patients,^(3)^ scenarios in which methadone is a cornerstone treatment. Based on these considerations, we performed a systematic review to evaluate studies in which methadone was administered to mechanically ventilated patients in the ICU and to understand the effects of methadone on mechanical ventilation (MV)-related outcomes, total opioid exposure, associated complications, and scores regarding pain, sedation, and delirium.
METHODS
Design
We conducted a systematic review with predetermined selection and outcome criteria following the Cochrane Handbook,^(12)^ and this review was registered on PROSPERO (registration: CRD42024517731). Prior to the comprehensive literature search, we searched for ongoing systematic reviews on PROSPERO. Afterwards, an information specialist designed a comprehensive literature search strategy. We searched the following databases from inception to January 24, 2025: MEDLINE, EMBASE, Wiley's Cochrane Library, CINAHL, PubMed (non-MEDLINE), Scopus, and LILACS. Eligible studies included RCTs and observational studies that compared the use of methadone to the standard of care or to other analgosedation strategies in mechanically ventilated patients in the ICU. Additionally, we searched the Clinical Trials Registry Database (https://clinicaltrials.gov) for registered, unpublished, and ongoing studies. We also searched the bibliographies of the included studies and review articles. Studies were restricted to English, Portuguese, and Spanish languages (Supplementary Material).
We included studies that described adult (over 18 years of age) patients receiving MV in the ICU who had also received methadone. In our initial design, pain, sedation, and delirium scores were our main outcomes. During screening and data extraction, we observed that most of the studies focused on MV-related outcomes; therefore, we changed the main outcomes to MV-related outcomes, which included the duration of MV, ventilator-free days, successful weaning, and weaning time. The secondary outcomes included total opioid exposure; incidences of nausea and vomiting, coma, withdrawal to opioids and arrhythmias; ICU and hospital lengths of stay; incidence of hospital-acquired pneumonia; time to weaning from intravenous or oral sedation; and scores regarding pain, sedation, and delirium. Pain and sedation scores were assessed in the included studies via behavioral pain scales,^(13)^ visual analog scales or numeric rating scales; sedation scores were assessed in the studies via the Richmond Analgesia and Sedation Scale (RASS),^(14)^ the Ramsay Sedation Scale,^(15)^ and the Riker Sedation-Agitation Scale;^(16)^ and delirium was assessed in the studies via the Confusion Assessment Method for the ICU.^(17)^ We reported our review based on the PRISMA guidelines.^(18)^
Control and intervention groups
The intervention group included patients who received methadone (either alone or in addition to other opioids) as a strategy of sedation. The control group included patients receiving the standard-of-care strategy of sedation without methadone.
Study selection
Two authors independently reviewed abstracts and assessed eligibility via Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia, 2024). A full-text review was conducted when either reviewer considered that the abstract met the inclusion criteria. Both reviewers agreed on the full text for inclusion, with an independent reviewer resolving any disagreements.
Data extraction and synthesis
All of the data were extracted in duplicate. The authors independently extracted the following data from the included studies: study and patient characteristics, study interventions, total opioid use, and outcomes. Both reviewers independently assessed the risk of bias at the outcome level regarding randomization, deviations from intended interventions, missing outcome data, and selection of the reported result. The Cochrane risk of bias tool for randomized studies (RoB2)^(19)^ and the risk of bias in nonrandomized studies of interventions (ROBINS-I) tool^(20)^ were used to assess the risks of bias in randomized and nonrandomized studies, respectively. The third reviewer resolved any discrepancy that arose during this assessment. Additionally, the quality of evidence for each manuscript was assessed by the reviewers via the GRADE framework and is reported by outcome.^(21)^
RESULTS
Study selection
The search strategy yielded 3,523 citations, of which 1,628 were duplicates. The remaining 1,895 abstracts were screened, with 1,568 being excluded. We completed a full-text review of 38 studies, of which 12 studies met the inclusion criteria, including 7 abstracts^(22-28)^ and 5 manuscripts^(9,29-32)^ (Figure 1).
Identification of studies from the search strategy based on the inclusion and exclusion criteria.
Characteristics of the included studies
Table 1 summarizes the study type, population, control, intervention, and outcomes of the included studies. A total of 773 patients were included among the included abstracts and manuscripts. All of the included studies were generally small in size, with sample sizes ranging from 16 to 118 patients. The included studies had heterogeneous designs, methadone dosages, and patient populations. The characteristics of the patients included trauma (n = 118),^(22)^ burn injuries (n = 153),^(24,29)^ risk for fentanyl abstinence syndrome (n = 84),^(23,26)^ opioid addiction or withdrawal (n = 106),^(25,32)^ and receiving fentanyl for at least 72 hours prior to weaning (n = 221).^(9,23,26,31)^ The administration of methadone was compared to the nonadministration of methadone,^(22,27)^ standard of care (n = 213),^(24,29,31)^ fentanyl administration (n = 140),^(23,26,32)^ opium tincture administration,^(25)^ oxycodone administration,^(30)^ and placebo administration.^(9)^ Standard of care and the nonadministration of methadone were defined as the groups of patients who did not receive methadone; moreover, opium tincture is a medication that is commonly used to treat diarrhea and may be used as an alternative to methadone when treating patients with opioid use disorders.
Mechanical ventilation-related outcomes
Mechanical ventilation-related outcomes were reported (either as a primary or secondary outcome) in all but two of the studies.^(25,31)^ The included studies described ventilator-free days (n = 271),^(22,24,29)^ days on MV,^(23)^ anticipation of extubation,^(26)^ duration of intubation,^(26)^ successful weaning,^(30)^ weaning success on day 5 (n = 136),^(9,26)^ early extubation,^(26)^ and decreased weaning time.^(9)^
One RCT^(9)^ revealed that the enteral administration of methadone led to a significantly greater probability of successful weaning within the first five days (hazard ratio [HR]: 2.64 [1.22 to 5.69]; p < 0.02), as did a retrospective cohort (HR: 1.89 [1.16 to 3.07]; p = 0.01]).^(30)^ These results were corroborated by two abstracts from the same group of investigators.^(23,26)^ Enteral methadone use was also associated with a shorter weaning time (HR: 2.06 [1.17 to 3.63]; p < 0.004) but not with the probability of early extubation (HR: 1.52 [0.87 to 2.64]; p = 0.11).^(9)^ In terms of ventilator-free days, a pilot study^(29)^ and a retrospective chart review^(24)^ indicated that methadone was associated with significantly more ventilator-free days (11.5 days versus 16.5 days; p = 0.03 and 15 days versus 9.5 days; p = 0.009, respectively), whereas a propensity score-matched cohort observed no such benefit (12.6 versus 15.2; p = 0.18).^(22)^
Secondary outcomes
The secondary outcomes included length of stay in the ICU (n = 172),^(23,27,30,32)^ development of ventilator-associated pneumonia,^(22)^ duration of analgesia,^(24)^ cumulative dose of opioids in morphine equivalents,^(27)^ duration of sedation,^(24)^ behavior pain scale,^(25)^ incidence of delirium,^(27)^ RASS score,^(25)^ patients discharged alive,^(29)^ adverse effects from methadone administration,^(27)^ discontinuation of opioids (n = 227),^(28,30,31)^ withdrawal symptoms,^(32)^ and Clinical Opiate Withdrawal Score (COWS) score.^(32)^
The use of methadone to discontinue opioid infusions was evaluated in three studies. One study^(31)^ reported that enteral methadone administration shortened the time needed to discontinue fentanyl infusions in critically ill patients (4.5 [3.9 to 5.8] days versus 7.0 [4.9 to 11.5] days; p = 0.002), which is similar to the results of Azimi et al.,^(30)^ who reported that IV opioid discontinuation was faster with methadone than with oxycodone (104.7 ± 79.4 hours versus 158.3 ± 171.2 hours, respectively; p = 0.04). Conversely, in another study, methadone was not observed to be associated with a reduction in the time to weaning for continuous infusion (57.5 hours versus 69 hours; p = 0.527).^(28)^ Bonnin et al.^(27)^ did not identify any evidence of any effects of enteral methadone administration on total opioid intake, ICU length of stay, incidence of delirium or increased QTc from a baseline cumulative value. Moreover, methadone provided faster alleviation of withdrawal symptoms compared to fentanyl, with symptoms subsiding within 30 minutes for methadone versus 120 minutes for fentanyl (p = 0.007).^(32)^ Both drugs effectively controlled withdrawal symptoms over time, with no significant differences in ICU or hospital stay duration, duration of intubation, or complications being observed between the groups.
Methodological quality of the included studies
A summary of evidence is outlined in table 2 for each outcome that was assessed in the manuscripts included in our review. For the primary outcome, only one study demonstrated high-quality data with a low risk of bias.^(9)^ The other two studies^(29,32)^ demonstrated low-to-moderate quality data, as well as a moderate-to-serious risk of bias. The overall effect of methadone was either likely beneficial^(9,29)^ or had no effect.^(32)^ For secondary outcomes including ICU outcomes, opioid discontinuation, and opioid withdrawal symptoms, the administration of methadone was either likely beneficial or had no effects, although this was based on low-quality evidence and a high risk of bias. The risk of bias summary is presented in figure 2, and the GRADE quality of the evidence assessment per study is presented in table 3.
Risk of bias summary
DISCUSSION
We summarized the current literature on methadone administration in mechanically ventilated patients in the ICU. Overall, in low-quality studies with a high risk of bias, the use of methadone was associated with improved ventilation-associated outcomes and faster opioid infusion discontinuation, although without benefits for managing withdrawal symptoms.
Long-term opioid use can lead to physical dependence, which places 16 - 32% of adult patients at risk for withdrawal syndrome in the ICU.^(33)^ The clinical manifestations of withdrawal syndrome overlap with the criteria assessed in patients who are weaning from the ventilator,^(34)^ thereby potentially postponing extubation. Moreover, the evaluation and management of opioid withdrawal may be challenging.^(33,35)^ Alternative strategies, such as alpha_2_-adrenergic agonists, are associated with more adverse effects compared to methadone.^(36)^ Interestingly, methadone exerts benefits for infants who require prolonged MV;^(37)^ moreover, it is the standard of care for children who are intubated for acute respiratory failure^(38)^ and effectively minimizes opioid withdrawal symptoms in at-risk children.^(39)^ Conversely, in adults with chronic opioid use disorder, methadone use was not observed to be associated with improvements in the RASS or COWS score. At least two factors may explain these discrepancies: (1) the RASS and COWS are unsuitable for assessing opioid withdrawal in intubated patients, which may have biased the results;^(40)^ and (2) inappropriate opioid conversion led to differing dosages between the groups, thereby leading to difficulties in attributing these findings solely to the medications (rather than to the dosing discrepancies). As a result, the effectiveness of methadone administration for opioid withdrawal in adults remains uncertain.
Methadone may also be employed to facilitate opioid tapering, which involves careful adjustments and/or opioid conversion. In the pediatric population, methadone has been suggested for use over other opioid regimens;^(41)^ however, this finding was not corroborated in a meta-analysis.^(42)^ In adults, methadone was observed to be associated with shorter opioid discontinuation times when compared to standard care^(31)^ or other opioids.^(30)^ Notably, pharmacokinetic-dynamic differences exist between methadone and shorter-acting opioids. For example, fentanyl infusion may exhibit an increased context-sensitive half-life^(43)^, whereas the active metabolites of morphine can paradoxically result in hyperalgesia.^(44)^ Conversely, methadone binds to multiple receptors, thereby functioning as a single-drug multimodal analgesic approach.^(45)^ We questioned whether the improved outcomes were secondary to improved pain management, thus leading to less agitation and an increased likelihood of extubation. Unfortunately, none of the studies measured metabolite serum concentrations.
Finally, ICU patients develop neuroplastic changes that contribute to pain^(46)^ and are often treated with opioids.^(47,48)^ However, the benefits of methadone may be limited to patients using high-dose opioids. For example, in the study by Wanzuita et al.,^(9)^ the mean dose of morphine in milligram equivalents was 422mg/day in the methadone group, which was 4 - 8 times greater than that reported by Burry et al.^(48)^ but was half that reported by Payen et al.^(13)^ It is possible that high-dose opioid use is secondary to an analgesia-first approach to achieve appropriate sedation goals, thus leading to opioid misuse. Strategies to minimize opioid use include multimodal analgesia, opioid rotation, and opioid weaning protocols, all of which represent indications for methadone.
Clinical implications and considerations
The applicability of methadone to every intubated patient is not recommended, given that most studies only included patients who were at risk for opioid withdrawal. We suggest adhering to the approach by Wanzuita et al. (the only RCT included in our review).^(9)^ Although intravenous methadone administration offers more reliable bioavailability compared to enteral administration,^(49)^ its use should be approached with caution due to a lack of supporting evidence.
However, the administration of methadone may be associated with adverse cardiac effects.^(50)^ A prolonged QT interval is a surrogate marker for developing Torsades de Pointes, which is a rare and lethal ventricular arrhythmia.^(51)^ QT interval prolongation has been observed to occur when methadone is used at doses higher than 60 - 120mg/day,^(52,53)^ which is a limit that was not exceeded in this review. In addition, inappropriate methadone dosing may impair the function of vital systems, thereby significantly impacting patient outcomes. For example, high doses of methadone may lead to an overly sedated patient who may not trigger the ventilator or participate in physiotherapy, thus prolonging MV; moreover, these patients may also require vasopressors and may be more susceptible to delirium. Conversely, low doses can lead to patient-ventilator dyssynchrony and agitation.^(54)^ Due to these potential adverse effects, we recommend careful work-ups and close monitoring for patients receiving methadone with routine electrocardiograms, especially if there is concomitant administration of medications that may prolong the QT interval. The administration of methadone should be stopped, and patients should be closely assessed if the QT interval is > 500ms.
Strengths and limitations
Several strengths should be highlighted in this study. For example, we conducted a broad systematic review of the literature via the Cochrane Handbook and reported the results following the PRISMA guidelines. Moreover, an extensive literature search was conducted utilizing multiple databases, and we also used a preregistered protocol and analytical plan. Furthermore, we evaluated the risk of bias and quality of evidence via three different tools. However, our review also has several limitations. First, we changed the primary outcome of our review after completing abstract screening due to a lack of data on the initially planned outcomes. However, our research strategy was broad and included methadone and ICU as factors (Supplementary Material), and we updated our PROSPERO registration to reflect the implemented changes. We also reported and discussed the outcomes regarding pain, delirium and agitation scores. Additionally, the overall GRADE quality of the included studies was low, and most of the studies exhibited a moderate-to-serious risk of bias, with notable heterogeneity being observed in patient populations, interventions, comparators, and outcomes. Most of the studies included patients at risk of opioid withdrawal or chronic opioid use, which further limits any benefits related to methadone. Additionally, more than half of the included patients were reported in abstracts that either did not present detailed methodology or were published as manuscripts, thus eliciting concerns about publication bias. Notably, the same group of authors published two abstracts with different outcomes; however, it is impossible to determine whether these publications included the same patients. Low-quality studies may selectively report positive findings, lack external validity, and either overestimate or underestimate the effect of an intervention. Finally, most of the studies compared methadone to shorter-acting opioids or placebo. Thus, the benefits of methadone may be related to its pharmacokinetics and not to its pharmacodynamics.^(55)^ These limitations pose important obstacles to the generalization of our findings.
Implication statement
The management of pain in mechanically ventilated patients is challenging. Low-quality evidence suggests that methadone, which is a synthetic opioid used to treat opioid use disorder, opioid withdrawal, and chronic pain, may be associated with better patient-centered outcomes. Further high-quality studies are warranted to validate this conclusion.
CONCLUSION
Significant limitations in the literature warrant caution regarding the use of methadone in mechanically ventilated patients in the intensive care unit. Most of the included studies demonstrated a low quality of evidence, with a moderate-to-high risk of bias being observed. High-quality, well-designed, and adequately powered studies are needed to rigorously evaluate the potential advantages of methadone in this patient population.
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stein-Parbury J Mc Kinley S Patients’ experiences of being in an intensive care unit: a select literature review Am J Crit Care 200091202710631387 · pubmed ↗
- 2Burry L Cook D Herridge M Devlin JW Fergusson D Meade M SLEAP Investigators; Canadian Critical Care Trials Group. Recall of ICU stay in patients managed with a sedation protocol or a sedation protocol with daily interruption Crit Care Med 20154310218021902618122110.1097/CCM.0000000000001196 · doi ↗ · pubmed ↗
- 3Devlin JW Skrobik Y Gélinas C Needham DM Slooter AJ Pandharipande PP Executive Summary: Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU Crit Care Med 2018469153215483011337110.1097/CCM.0000000000003259 · doi ↗ · pubmed ↗
- 4Pham T Heunks L Bellani G Madotto F Aragao I Beduneau G WEAN SAFE Investigators. Weaning from mechanical ventilation in intensive care units across 50 countries (WEAN SAFE): a multicentre, prospective, observational cohort study Lancet Respir Med 20231154654763669340110.1016/S 2213-2600(22)00449-0 · doi ↗ · pubmed ↗
- 5Shehabi Y Howe BD Bellomo R Arabi YM Bailey M Bass FE ANZICS Clinical Trials Group and the SPICE III Investigators. Early sedation with dexmedetomidine in critically ill patients N Engl J Med 201938026250625173111238010.1056/NEJ Moa 1904710 · doi ↗ · pubmed ↗
- 6Wunsch H Kahn JM Kramer AA Rubenfeld GD Use of intravenous infusion sedation among mechanically ventilated patients in the United States Crit Care Med 20093712303130391963354310.1097/CCM.0b 013e 3181 b 02eff · doi ↗ · pubmed ↗
- 7Elliott K Kest B Man A Kao B Inturrisi CE N-methyl-D-aspartate (NMDA) receptors, mu and kappa opioid tolerance, and perspectives on new analgesic drug development Neuropsychopharmacology 1995134347356874775910.1016/0893-133X(95)00083-P · doi ↗ · pubmed ↗
- 8Murphy GS Szokol JW Avram MJ Greenberg SB Shear TD Deshur MA Clinical effectiveness and safety of intraoperative methadone in patients undergoing posterior spinal fusion surgery: a randomized, double-blinded, controlled trial Anesthesiology 201712658228332841896610.1097/ALN.0000000000001609 · doi ↗ · pubmed ↗