Apnea testing for brain death confirmation in VV-ECMO patients with very low sweep flow: a case reports and practical physiological insights
Carine Carrijo de Faria, Pedro Vitale Mendes, Luis Carlos Cardoso Maia, Gabriel Afonso Dutra Kreling, Marcelo Park

TL;DR
This paper describes a safe method for confirming brain death in patients on VV-ECMO using a low-sweep-flow apnea test.
Contribution
A standardized, physiologically grounded apnea test protocol for brain death confirmation in VV-ECMO patients.
Findings
The apnea test with very low sweep flow is safe and feasible for brain death confirmation in VV-ECMO patients.
Low sweep flow (200mL/minute) effectively increases CO2 levels to meet brain death criteria.
Temporary increases in ECMO blood flow can manage hypoxemia during the test.
Abstract
In recent years, venovenous extracorporeal membrane oxygenation has become a critical therapeutic tool for patients with severe respiratory failure. Neurological complications, including brain death, are common in this population, and confirming brain death in venovenous extracorporeal membrane oxygenation-supported patients presents unique challenges. In Brazil, an apnea test is mandatory for confirming brain death. However, its application in patients on venovenous extracorporeal membrane oxygenation, which predominantly addresses venoarterial extracorporeal membrane oxygenation cases, is not well defined in the literature. This report outlines our standardized approach for conducting apnea tests in three patients with suspected brain death during ongoing venovenous extracorporeal membrane oxygenation support. We describe three cases from a cohort of 93 extracorporeal membrane…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
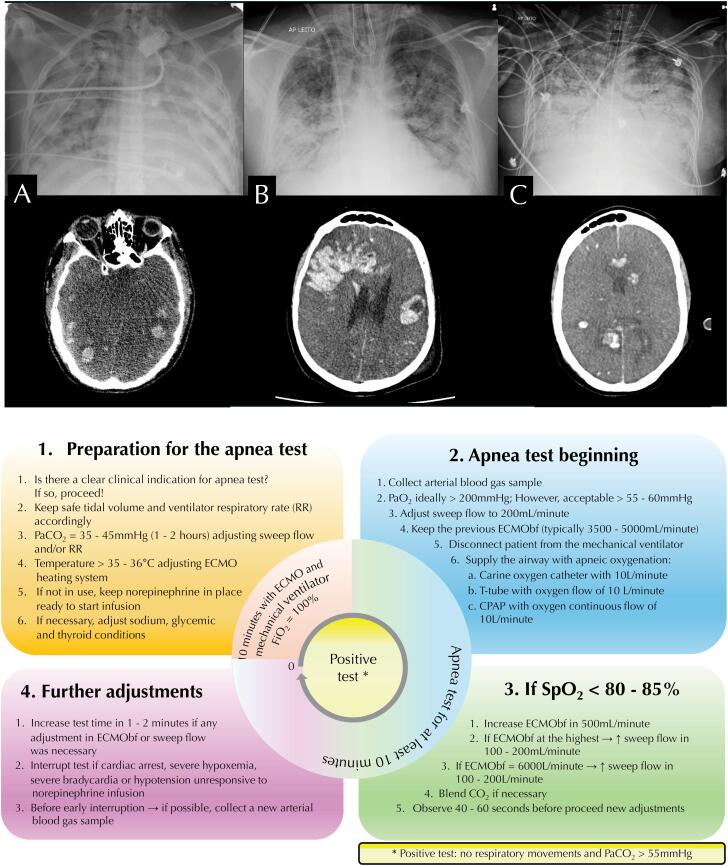 Figure 1
Figure 1| Patient 1 | Patient 2 | Patient 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 32 | 34 | 31 | ||||||
| Sex | Male | Male | Female | ||||||
| SAPS 3 | 74 | 81 | 93 | ||||||
| Weight (kg) | 84 | 85 | 60 | ||||||
| Height (cm) | 191 | 180 | 162 | ||||||
| Admission SOFA | 8 | 16 | 16 | ||||||
| Before ECMO initiation | |||||||||
| Heart rate (BPM) | 135 | 119 | 127 | ||||||
| Mean ABP (mmHg) | 80 | 78 | 66 | ||||||
| Norepinephrine (mcg/kg/minute | ----- | 0.6 | 1 | ||||||
| Vasopressin (IU/minute) | ----- | 0.04 | 0.04 | ||||||
| Temperature (°C) | 38.0 | 37.8 | 36.0 | ||||||
| BUN/creatinine (mg/Dl) | 77/1.76 | 105/9.17 | 42/4.59 | ||||||
| ALT/AST (IU/mL) | 159/481 | 107/197 | 5,941/2,592 | ||||||
| Hemoglobin (g/dL) | 7.9 | 10 | 6.4 | ||||||
| Leukocytes (cels/mm3) | 12,770 | 14,450 | 19,360 | ||||||
| Platelets (units/mm3) | 173,000 | 209,000 | 50,000 | ||||||
| INR | 1.89 | 2.02 | 1.44 | ||||||
| RASS | - 5 | - 5 | - 5 | ||||||
| Midazolam (mg/kg/hour) | 0.25 | 0.2 | 0.3 | ||||||
| Propofol (mg/kg/hour) | ----- | 0.3 | 0.2 | ||||||
| Fentanyl (mcg/hour) | 50 | 40 | 20 | ||||||
| Cisatracurium (mg/kg/hour) | 0.1 | 0.2 | ----- | ||||||
| Rocuronium (mg/kg/hour) | ----- | ----- | 0.2 | ||||||
| Ventilatory mode | PCV | PCV | VCV | ||||||
| Respiratory rate (IPM) | 38 | 40 | 35 | ||||||
| Tidal volume (mL) | > 300 | 400 | 380 | ||||||
| Plateau pressure (cmH2O) | > 32 | 34 | 40 | ||||||
| PEEP (cmH2O) | 17 | 14 | 3 | ||||||
| FiO2 (%) | 100 | 100 | 100 | ||||||
| pH | 7.06 | 7.01 | 7.10 | ||||||
| PaO2 (mmHg) | 43 | 47 | 35 | ||||||
| PaCO2 (mmHg) | 142 | 87.7 | 50 | ||||||
| SBE (mEq/L) | 2 | -2 | -16 | ||||||
| SatO2 (%) | 52 | 76 | 68 | ||||||
| P/F ratio (mmHg) | 43 | 47 | 35 | ||||||
| Rescue maneuvers | TGI/Prone/Recruitment | Prone | Prone/Recruitment | ||||||
| Renal support | CVVH | CVVHDF | CVVHDF | ||||||
| Apnea test | Before | After | Before | After | Before | After | Before | After | |
| Airway support | T-tube with oxygen 10L/minute | T-tube with oxygen 10L/minute | T-tube with oxygen 10L/minute | CPAP with oxygen 10L/minute | |||||
| Heart rate (BPM) | 94 | 95 | 87 | 90 | 115 | 133 | 120 | 124 | |
| Mean ABP (mmHg) | 84 | 85 | 80 | 84 | 107 | 105 | 93 | 113 | |
| Norepinephrine (mcg/kg/minute) | 0.15 | 0.15 | ----- | ----- | 0.12 | 0.12 | 0.02 | 0.02 | |
| Vasopressin (IU/minute) | 0.03 | 0.03 | 0.03 | 0.03 | ----- | ----- | 0.04 | 0.04 | |
| Temperature (°C) | 36.5 | 36.5 | 36.5 | 36.5 | 36.5 | 36.4 | 36.4 | 36.4 | |
| pH | 7.30 | 7.07 | 7.32 | 7.14 | 7.45 | 7.12 | 7.45 | 7,21 | |
| PaCO2 (mmHg) | 50.3 | 87.3 | 44.4 | 73.0 | 35.4 | 99.6 | 45 | 99 | |
| PaO2 (mmHg) | 67 | 61.2 | 100.3 | 66.3 | 91.9 | 58.9 | 74 | 70 | |
| SBE (mEq/L) | -2.6 | -7.5 | -3.9 | -6.3 | 4.2 | 0.2 | 8.2 | 10.1 | |
| SatO2 (%) | 90.5 | 77.1 | 97.0 | 84.2 | 95.2 | 86 | 97.4 | 89.1 | |
| ECMO blood flow (mL/minute) | 4,500 | 4,500 | 4,500 | 4,500 | 4,740 | 4,740 | 4,310 | 4,310 | |
| Sweep gas flow (mL/minute) | 8,000 | 200 | 8,000 | 200 | 5,000 | 200 | 4,000 | 200 | |
| ECMO FiO2 (%) | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | |
| ECMO temperature (°C) | 36.5 | 36.5 | 36.5 | 36.5 | 36.5 | 36.5 | 36.5 | 36.5 | |
| Time spent on apnea test (minutes) | 10 | 10 | 14 | 16 | |||||
| Hemoglobin (g/dL) | 7.3 | 7.3 | 8.6 | 7.0 | |||||
| Leukocytes (cels/mm3) | 25,810 | 25,810 | 27,160 | 12,810 | |||||
| Platelets (units/mm3) | 87,000 | 87,000 | 138,000 | 49,000 | |||||
| INR | 3.01 | 3.01 | 2.10 | 1.33 | |||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Cardiac Arrest and Resuscitation · Organ Donation and Transplantation
INTRODUCTION
Venovenous extracorporeal membrane oxygenation (VV-ECMO) support for patients with severe respiratory failure has increased in recent decades.^(1)^ Neurological complications are common in this population,^(2)^ and brain death is occasionally observed.^(2,3)^ In Brazil, the apnea test is mandatory for confirming brain death,^(4)^ but performing it in patients supported by VV-ECMO is not straightforward. The interplay among disease severity, organ support, and VV-ECMO gas exchange makes carbon dioxide (CO_2_) kinetics particularly complex. Furthermore, most of the current apnea testing literature focuses on venoarterial extracorporeal membrane oxygenation (VA-ECMO).^(5)^ Therefore, we designed a physiologically grounded apnea test for three VV-ECMO-supported patients. Here, we report and discuss our standardized experience.^(3)^
Case description
Informed consent was waived by the Research Ethics Committee of the Hospital das Clinics of the Universidade de São Paulo, due to the observational nature of this study (registration 107.443).
Since 2011, 93 patients have received ECMO at our institution. Of these, 43/93 (46%) died during hospitalization. Among these, 7/43 (16%) were diagnosed with brain death (four after decannulation: 2-VV-ECMO, 1-VA-ECMO, and 1 following venoarterial-venous [VAV]-ECMO). Three patients who progressed to brain death while receiving VV-ECMO support were included in this study. All were referred to our hospital and managed with VV-ECMO support. Suspicion of brain death arose during routine hourly patient evaluation by the multiprofessional team. Clinical signs included fixed, dilated, and nonreactive pupils; absence of motor responses despite low or no sedation at the time of respiratory support; and the absence of respiratory movements.
Patient 1 - Admitted with a diagnosis of severe community-acquired pneumonia without any comorbidity and developed severe hypoxemic respiratory failure. Prone positioning and alveolar recruitment were unsuccessful. Bronchopleural fistula and multiple organ failure (MOF) complicated his clinical status. Brain death was suspected two days after VV-ECMO initiation. Additional clinical details are provided in table 1 and figure 1A show further patients’ characteristics. This case was previously reported, at which time two apnea tests were required in Brazil.^(3)^ During the first test, oxygen saturation of 77% was reached in the final arterial blood gas analysis; however, the peripheral oxygen saturation (SpO_2_) remained above 80%.
Thoracic and cerebral images of the patients (Panels A, B, and C) and the structure of our standardized apnea test during ongoing venovenous extracorporeal membrane oxygenation support (Panel D).
Patient 2 - A patient without comorbidities, admitted with COVID-19 and severe respiratory failure, progressing to MOF. Two days after VV-ECMO initiation, brain death was suspected. Clinical data are shown in table 1 and figure 1B.
Patient 3 - Systemic erythematous lupus patient, with musculoskeletal, cutaneous, and hematologic involvement, treated with prednisone 40mg. She was admitted with severe alveolar hemorrhage and developed MOF with severe acute liver failure, requiring plasmapheresis, VV-ECMO, and renal support. Brain death was suspected four days after referral. Additional details are shown in table 1 and figure 1C.
All patients were observed for 24 hours without any sedative administration prior to initiating the brain death protocol. The apnea test was standardized as described in figure 1D. Transcranial Doppler confirmed circulatory collapse in all patients. Due to MOF, no organs were procured, and life support was subsequently withdrawn.
DISCUSSION
In Brazil, an increase in partial pressure of carbon dioxide (PaCO_2_) from 35 - 45 mmHg to > 55mmHg without spontaneous respiration is currently considered compatible with brain death.^(4)^ During ECMO support, CO_2_ clearance depends primarily on sweep flow and, to a lesser extent, on ECMO blood flow.^(6)^ However, reduced sweep flow to facilitate CO_2_ elevation during the apnea test results in prohibitive hypoxemia.^(6)^ Although oxygenation depends on blood flow, minimal fresh gas from sweep flow is still necessary to supply oxygen.^(6)^ Therefore, current guidelines recommend decreasing sweep flow to 0.5 - 1L/minute.^(5)^
This low sweep flow (0.5 - 1L/minute) still allows a CO_2_-transfer as high as 75mL/minute on an ECMO blood flow of 3,500mL/minute^(6)^ and 45mL/minute on a blood flow of 200 - 400mL/minute.^(7)^ Moreover, all patients received continuous renal support during the apnea test. Hypercapnia increases bicarbonate levels, facilitating both bicarbonate and CO_2_ removal through renal support.^(8)^ This makes it more challenging to achieve a PaCO_2_ > 55mmHg. Therefore, we selected a sweep flow of 200mL/minute.^(3)^
The limited oxygen delivery with this very low sweep flow can result in immediate hypoxemia and an ECMO-blood flow roof effect on oxygen transfer in the oxygenator.^(9)^ However, as a rescue maneuver for severe hypoxemia (SpO_2_ < 80 - 85%) during the apnea test, increasing ECMO-blood flow will increase the oxygen delivery, providing a brief window to finish the test safely. If severe hypoxemia persists, a higher sweep flow will be necessary; however, to reach the targeted CO_2_, a CO_2_ blend with the sweep gas may be required.^(10)^
CONCLUSION
The apnea test using very low sweep flow in patients receiving ongoing venovenous extracorporeal membrane oxygenation support is physiologically grounded, clinically plausible, and safe. Achieving the carbon dioxide levels recommended by Brazilian guidelines at the end of the apnea test is possible. Increasing extracorporeal membrane oxygenation blood flow can be a temporary rescue strategy in cases of significant hypoxemia (oxygen saturation <80 - 85%).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sauer CM Yuh DD Bonde P Extracorporeal membrane oxygenation use has increased by 433% in adults in the United States from 2006 to 2011 ASAIO Journal 201561131362530379910.1097/MAT.0000000000000160 · doi ↗ · pubmed ↗
- 2Mateen FJ Muralidharan R Shinohara RT Parisi JE Schears GJ Wijdicks EF Neurological injury in adults treated with extracorporeal membrane oxygenation Arch Neurol 20116812154315492182521610.1001/archneurol.2011.209PMC 7816483 · doi ↗ · pubmed ↗
- 3Mendes PV Moura E Barbosa EV Hirota AS Scordamaglio PR Ajjar FM Challenges in patients supported with extracorporeal membrane oxygenation in Brazil Clinics (Sao Paulo)20126712151115152329561110.6061/clinics/2012(12)27PMC 3521820 · doi ↗ · pubmed ↗
- 4Conselho Federal de Medicina Resolução CFM N° 2.173/2017 Define os critérios do diagnóstico de morte encefálica Disponível em: https://sistemas.cfm.org.br/normas/visualizar/resolucoes/BR/2017/2173
- 5Sady E Junqueira L Veiga VC Rojas SSO Apnea test for brain death diagnosis in adults on extracorporeal membrane oxygenation: a review Rev Bras Ter Intensiva 20203223123183266744210.5935/0103-507X.20200048 PMC 7405745 · doi ↗ · pubmed ↗
- 6Park M Costa EL Maciel AT Silva DP Friedrich N Barbosa EV Determinants of oxygen and carbon dioxide transfer during extracorporeal membrane oxygenation in an experimental model of multiple organ dysfunction syndrome P Lo S One 201381 e 549542338301110.1371/journal.pone.0054954 PMC 3558498 · doi ↗ · pubmed ↗
- 7Santos YA Cardozo LC Junior Mendes PV Besen BA Park M Factors associated with carbon dioxide transfer in an experimental model of severe acute kidney injury and hypoventilation during high bicarbonate continuous renal replacement therapy and oxygenation membrane support Crit Care Sci 202436 e 20240005 en 10.62675/2965-2774.20240005-en PMC 1120804138985048 · doi ↗ · pubmed ↗
- 8Cove ME Vu LH Ring T Federspiel WJ Kellum JA Respiratory dialysis—a novel low bicarbonate dialysate to provide extracorporeal CO 2 removal Crit Care Med 2020487 e 592e 5983230441810.1097/CCM.0000000000004351 · doi ↗ · pubmed ↗