The relevance of including delirium in the assessment of sepsis-associated neurological disorders that cause changes in consciousness or confusion
Roberta Esteves Vieira de Castro, Yu Kawai, Daniela Nasu Monteiro Medeiros, Arnaldo Prata-Barbosa, Neelima Marupudi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
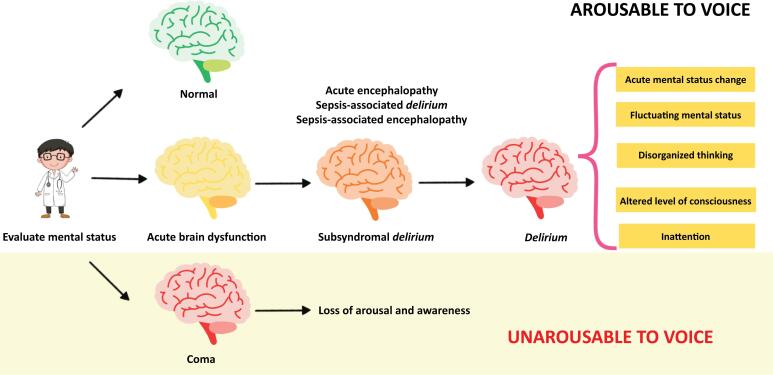 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Anesthesia and Neurotoxicity Research · Anesthesia and Sedative Agents
INTRODUCTION
Recently, the Society of Critical Care Medicine (SCCM) Pediatric Sepsis Definition Task Force developed a new, international pediatric sepsis consensus definition, the Phoenix Sepsis Score (PSS). Sepsis and septic shock in children are now diagnosed using objective clinical and laboratory variables across four major organ systems, including the central nervous system (CNS).^(1,2)^ This marks the first time that CNS organ dysfunction has been incorporated into the core definition of pediatric sepsis. The evaluation of neurologic dysfunction in the PSS involves the Glasgow Coma Scale (GCS) and the pupillary reflex test. To develop the PSS, investigators drew on a broad knowledge base, including an international survey, a systematic review, and the analysis of more than 3 million pediatric health consultations, followed by a rigorous consensus process.^(1)^ However, pediatric delirium (PD), which is a direct manifestation of CNS organ dysfunction, is not mentioned in the PSS. Numerous terms are used in the literature to describe brain dysfunction during acute disease. Therefore, we aim to show the differences in terminologies and their meanings to standardize language in different clinical practices and research contexts. Furthermore, we want to highlight the importance of evaluating PD in sepsis.
PEDIATRIC DELIRIUM
Delirium is a frequent but often underrecognized clinical syndrome of brain dysfunction in septic patients.^(3,4)^ Pediatric delirium is independently associated with adverse short- and long-term outcomes, including longer stays in pediatric intensive care units (ICUs) and hospitals, prolonged durations of mechanical ventilation (MV), higher mortality rates, greater direct hospital costs, and long-term cognitive impairment after hospital discharge.^(5,6)^ Delirium is widely observed (reported rates of up to 80%) among pediatric patients in critical condition across various disease states.^(4)^ Moreover, the literature shows that PD is present in 63% of septic patients, according to a validated bedside screening tool, the Cornell Assessment of Pediatric Delirium (CAP-D).^(6)^
Health care professionals often fail to recognize delirium unless screening tools are utilized. The recent PANDEM guidelines from the SCCM recommend the Preschool and Pediatric Confusion Assessment Methods for the ICU (ps/pCAM-ICU) or the CAP-D as the most valid and reliable delirium monitoring tools for critically ill pediatric patients.^(4)^ In addition, the European Society of Pediatric and Neonatal Intensive Care (ESPNIC) also recommends the CAP-D as an instrument to assess PD (grade of recommendation = A) and acknowledges the use of the pCAM-ICU and Sophia Observation withdrawal Symptoms-Pediatric Delirium scale (SOS-PD).^(7)^ Lastly, the PODIUM Consensus Conference supports a CAP-D score ≥ 9 as an indication of CNS organ dysfunction^(8)^ and the PALICC-2 guideline recommends the use of ps/pCAM-ICU, CAP-D or SOS-PS at least twice daily.^(9)^
The ps/pCAM-ICU is a "point-in-time" assessment tool derived from the highly reliable Confusion Assessment Method for the ICU (CAM-ICU) and adapted for pediatric patients. The pCAM-ICU, validated in patients over 5 years old, has high sensitivity (83%) and specificity (99%), with excellent interrater reliability (kappa [κ] = 0.96). The psCAM-ICU, adapted for children under 5 years of age, has good sensitivity (75%) and high specificity (91%), with reliability (κ = 0.79). It has also been validated in infants younger than 6 months, showing a sensitivity of 95% and specificity of 81%. The CAP-D demonstrated high sensitivity (94%) and specificity (79%) in a mixed medical-surgical pediatric ICU population, with strong interrater reliability among nursing staff (κ = 0.94), although reliability is lower in children under 2 years old (κ = 0.6).^(4,10,11)^ Finally, the SOS-PD scale has an overall sensitivity of 92.3% and a specificity of 96.5%.^(12)^
The use of the term "acute encephalopathy" is discouraged when describing clinical features observed at the bedside.^(5)^ Instead, Slooter et al. suggest using "subsyndromal delirium" to describe acute cognitive changes that resemble delirium but do not meet all the gold standard criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition text revision (DSM-5-TR).^(5,13)^ The term "delirium" should be reserved for cases that meet DSM-5-TR criteria, whereas "coma" should describe a state of severely reduced responsiveness, as defined by diagnostic tools such as the GCS or the Full Outline of UnResponsiveness (FOUR) score^(5)^ (Figure 1). Importantly, prior coma is a nonmodifiable risk factor that has been strongly linked to delirium.^(14)^
Recommended nomenclature for describing acute cognitive disturbances in clinical practice.
WHY THE GLASGOW COMA SCALE FALLS SHORT IN ASSESSING ACUTE BRAIN DYSFUNCTION
The GCS is typically represented as a single score combining three assessments: eye opening, verbal response, and motor response. Although extensively researched and integrated into various scoring systems, the GCS has shown variable interrater reliability. Studies have reported a broad range of κ scores, with one study noting values ranging from 0.39 - 0.79. Discrepancies in scoring are more common between different professional groups (e.g., nurses versus medical doctors), particularly regarding the motor score, with higher disagreement rates observed among less experienced staff and patients with intermediate scores. Conversely, the lowest levels of disagreement are found within specialized professional groups (e.g., neurocritical care nurses), particularly when evaluating the verbal component or assessing patients who are alert or slightly drowsy.^(15)^
Recently, Sanchez-Pinto et al. evaluated sepsis-associated encephalopathy in children using the qSOFA score, which uses the GCS to determine mental state.^(2)^ Cheung et al. also used the GCS to diagnose disorders of consciousness in pediatric patients with severe sepsis (GCS score < 12 with no sedatives).^(16)^ However, the GCS lacks key elements for assessing crucial components of delirium, such as inattention, purposefulness, restlessness, and consolability, making it unsuitable for evaluating this condition.^(5,6)^ For example, a child with a GCS score ≥ 12, who may not have been classified as having encephalopathy in previous studies, can still experience delirium.^(17)^ Additionally, the GCS is difficult to interpret in patients receiving invasive MV, which is a common clinical scenario in septic shock. Additionally, a low GCS score may indicate the effects of interventions related to critical illness, such as sedation or neuromuscular blockade, rather than directly reflecting primary organ dysfunction.^(2)^
CONCLUSIONS
Consistently, bedside screening is essential to prevent the underestimation of delirium incidence, as its fluctuating nature must be considered. We strongly believe that diagnosing delirium using bedside tools as a marker of central nervous system dysfunction is superior to diagnosing "encephalopathy" via the Glasgow Coma Scale. Prompt recognition of pediatric delirium enables timely delirium management. Additionally, it helps identify vulnerable patients with a sepsis phenotype who require additional care to reduce the risk of developing pediatric delirium and supports the identification of an important cohort for future research on adjuvant therapies and prognosis.
Finally, we emphasize that delirium assessment should be a standard part of daily pediatric intensive care unit care. Including this recommendation in pediatric sepsis management will improve quality of care, facilitate timely management, and reduce the risk of negative short- and long-term outcomes. Delirium evaluation is part of a new era in pediatric intensive care medicine.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schlapbach LJ Watson RS Sorce LR Argent AC Menon K Hall MW Society of Critical Care Medicine Pediatric Sepsis Definition Task Force. International Consensus Criteria for Pediatric Sepsis and Septic Shock JAMA 202433186656743824588910.1001/jama.2024.0179 PMC 10900966 · doi ↗ · pubmed ↗
- 2Sanchez-Pinto LN Bennett TD Stroup EK Luo Y Atreya M Bubeck Wardenburg J Derivation, validation, and clinical relevance of a pediatric sepsis phenotype with persistent hypoxemia, encephalopathy, and shock Pediatr Crit Care Med 202324107958063727294610.1097/PCC.0000000000003292 PMC 10540758 · doi ↗ · pubmed ↗
- 3Atterton B Paulino MC Povoa P Martin-Loeches I Sepsis associated delirium Medicina (Kaunas)20205652402403244360610.3390/medicina 56050240 PMC 7279289 · doi ↗ · pubmed ↗
- 4Smith HA Besunder JB Betters KA Johnson PN Srinivasan V Stormorken A 2022 Society of Critical Care Medicine Clinical Practice Guidelines on Prevention and Management of Pain, Agitation, Neuromuscular Blockade, and Delirium in Critically Ill Pediatric Patients with Consideration of the ICU Environment and Early Mobility Pediatr Crit Care Med 2022232 e 741103511943810.1097/PCC.0000000000002873 · doi ↗ · pubmed ↗
- 5Slooter AJ Otte WM Devlin JW Arora RC Bleck TP Claassen J Updated nomenclature of delirium and acute encephalopathy: statement of ten Societies Intensive Care Med 2020465102010223205588710.1007/s 00134-019-05907-4PMC 7210231 · doi ↗ · pubmed ↗
- 6de Araújo BE da Silva Fontana R de Magalhães-Barbosa MC Lima-Setta F Paravidino VB Riveiro PM Clinical features, electroencephalogram, and biomarkers in pediatric sepsis-associated encephalopathy Sci Rep 202212110673106733573923010.1038/s 41598-022-14853-z PMC 9225983 · doi ↗ · pubmed ↗
- 7Harris J Ramelet AS van Dijk M Pokorna P Wielenga J Tume L Clinical recommendations for pain, sedation, withdrawal and delirium assessment in critically ill infants and children: an ESPNIC position statement for healthcare professionals Intensive Care Med 20164269729862708434410.1007/s 00134-016-4344-1PMC 4846705 · doi ↗ · pubmed ↗
- 8Wainwright MS Guilliams K Kannan S Simon DW Tasker RC Traube C Pediatric Organ Dysfunction Information Update Mandate (PODIUM) Collaborative. Acute neurologic dysfunction in critically ill children: The PODIUM Consensus Conference Pediatrics 20221491 Suppl 1S 32S 383497068110.1542/peds.2021-052888 E · doi ↗ · pubmed ↗