One-hour positive pressure ventilation after a successful spontaneous breathing trial: a multicenter feasibility randomized clinical trial
Aline Braz Pereira, Michelli Marcela Dadam, Bruna de Albuquerque Catelano, Daniela Delvan, Vitor Hugo Silva Pastorello, Luana Caroline Radun, Israel Silva Maia, Cassio Luis Zandonai, Eliana Vieira Santucci, Gabriela Souza Murizine, Marcelo Luiz Pereira Romano

Abstract
Click any figure to enlarge with its caption.
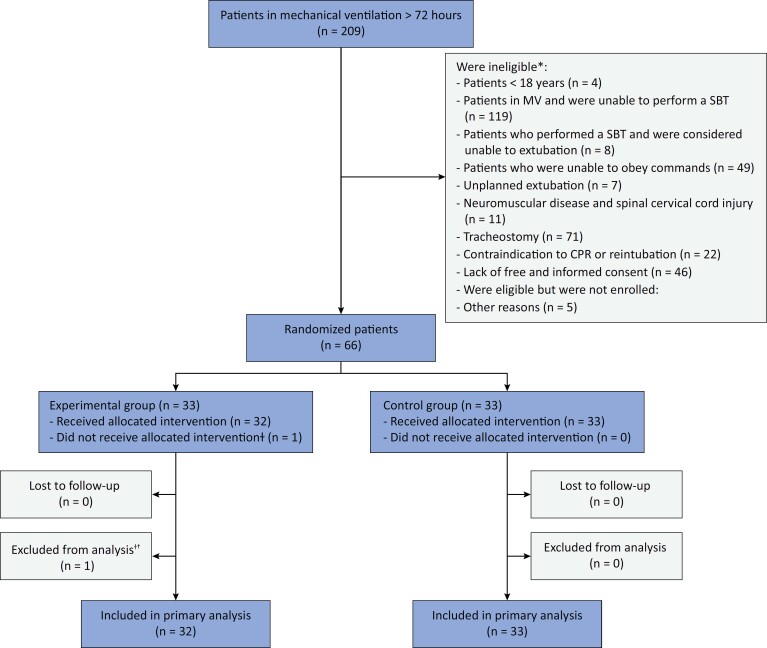 Figure 1
Figure 1| Experimental Group (n = 32) | Control Group (n = 33) | Difference (95%CI) | |||
|---|---|---|---|---|---|
| Relevant baseline characteristics | |||||
| Weaning
| |||||
| Short | 22 (68.7) | 21 (63.6) | - | ||
| Difficult | 10 (31.2) | 11 (33.3) | - | ||
| Prolonged | 0 (0) | 1 (3.0) | - | ||
| Indication of orotracheal intubation | |||||
| Surgical procedure | 12 (37.5) | 9 (27.2) | - | ||
| Neurological | 10 (31.2) | 10 (30.3) | - | ||
| Respiratory failure | 9 (28.1) | 10 (30.3) | - | ||
| Circulatory | 1 (3.1) | 3 (9.0) | - | ||
| Other | 0 (0) | 1 (3.0) | - | ||
| SAPS 3 | 70 (61.5 - 78.5) | 67 (57 - 80) | |||
| High risk of extubation failure | 31 (96.8) | 31 (94.0) | |||
| Very high risk of extubation failure
| 11 (34.3) | 8 (24.2) | |||
| Feasibility outcomes | |||||
| Primary outcome - adherence to mandatory items
| 30 (93.7)
| 33 (100) | - | ||
| Adherence to suggested items | |||||
| Checklist for assessing eligibility for weaning and SBT | 32 (100) | 33 (100) | - | ||
| SBT, according to the protocol | 32 (100) | 33 (100) | - | ||
| Assessment and management of laryngeal edema risk | 32 (100) | 33 (100) | - | ||
| NIV and/or HFNC after extubation in high-risk patients | 14/31 (45.1) | 14/31 (45.1) | - | ||
| NIV and/or HFNC duration (hours) | 2.5 (2 - 3.5) | 3 (2 - 4.5) | - | ||
| Clinical outcomes | |||||
| Extubation failure within 7 days
| 9 (28.1) | 14 (42.4) | -14.4 (-35.3 to 8.5)
| ||
| SBT in pressure support | 4/14 (28.5) | 5/16 (31.2) | - | ||
| SBT in T-piece | 5/18 (27.7) | 9/17 (53.0) | - | ||
| Extubation failure – reasons | |||||
| Respiratory failure | 8/9 (88.8) | 11/14 (78.5) | - | ||
| Neurological | 1/9 (11.1) | 0/14 (0) | - | ||
| Procedure | 0/9 (0) | 3/14 (21.5) | - | ||
| MV free days at 28 days | 28 (23 - 28) | 28 (17 - 28) | 1.52 (0.57 to 4.15)
| ||
| ICU length of stay (days) | 12.5 (6 - 17.5) | 11 (8 - 20) | - | ||
| Hospital length of stay (days) | 26.5 (17.7 - 53.5) | 24 (16 - 39) | - | ||
| ICU mortality | 2 (6) | 5 (15) | - | ||
| Hospital mortality | 6 (19) | 5 (15) | - | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory Support and Mechanisms · Cardiac Arrest and Resuscitation · Intensive Care Unit Cognitive Disorders
INTRODUCTION
A small, randomized trial suggests that 1-hour positive pressure ventilation after a successful spontaneous breathing trial (SBT) on a T-piece may decrease extubation failure.^( 1 )^ However, the effect on extubation failure was not statistically significant in another similar trial, despite a possible benefit for the subgroup of patients with more than 72 hours of mechanical ventilation (MV).^( 2 )^ The primary objective of this study was to evaluate the feasibility of conducting large randomized controlled trials to determine whether, in patients with more than 72 hours of MV, 1-hour positive pressure ventilation following a successful SBT, either on T-piece or pressure support, reduces the risk of extubation failure within 7 days. Feasibility was defined as the capability to complete the study according to the planned schedule (enrolment within 6 months) and with adherence above 90% to the procedures in the experimental group (1-hour positive pressure ventilation [± 10 minutes] after an SBT followed by extubation) and control group (immediate extubation after an SBT).
METHODS
This randomized, multicenter feasibility (pilot) trial was conducted at four Brazilian hospitals. Patients and healthcare professionals were not blinded to treatment assignments. The trial was approved by the Ethics Committee of the coordinating center and the sites participating in the study (CAAE 70984323.1.1001.5362) and registered with Clinicaltrials.gov (Clinical Trials identifier: NCT 05999526). The study protocol is available in the Supplementary Material .
Eligible participants were adults aged 18 years or older, admitted to the intensive care unit, intubated with an orotracheal tube, receiving MV for more than 72 hours, who underwent a successful SBT (as defined by the study protocol) and were deemed ready for extubation. Investigators randomized eligible participants immediately after a successful SBT to one of two groups: 1-hour positive pressure ventilation with ventilatory parameters as used before the SBT followed by extubation; or immediate extubation. The study protocol recommended for both groups daily assessment checklist to evaluate the eligibility for weaning and SBT;^( 3 – 5 )^ performing the SBT on pressure support or T-piece for 30 minutes;^( 6 )^ assessment and management of laryngeal edema risk;^( 7 , 8 )^ use of noninvasive ventilation and/or high flow nasal cannula for up to 24 hours after extubation in patients at high risk of extubation failure.^( 9 , 10 )^ As this was a study to assess feasibility (pilot), a convenience sample size of 60 patients was defined. Statistical analysis was described in the Supplementary Material .
RESULTS
From November 2023 to March 2024, 66 patients fulfilled eligibility criteria and were enrolled in the study well within the planned schedule ( Figure 1 ). One patient was excluded from the analysis due to ineligibility and incorrect randomization.
Enrollment, randomization, intervention, and follow-up.
Table 1 describes the relevant baseline characteristics and outcomes. The study interventions were performed as assigned in 95% of patients (33 [100%] in the Control Group versus 30 [93.7%] in the Experimental Group). In the Experimental Group, two patients did not receive 1-hour positive pressure ventilation according to protocol but were included in the intention-to-treat analysis. Noninvasive ventilation and/or high-flow nasal cannula after extubation were used in 45.1% of patients of high-risk patients. Adherence to other protocol items was 100%. Extubation failure within 7 days occurred in 35% of patients (9 [28%] in the Experimental Group versus 14 [42.4%] in the Control Group). Additional results are available in figure 1S and tables 1S and 2S ( Supplementary Material ).
DISCUSSION
These results demonstrate that it is feasible and needed to perform large, randomized trials to determine whether 1-hour positive pressure ventilation after a successful SBT, on T-piece or pressure support, reduces the risk of extubation failure within 7 days in patients who have undergone more than 72 hours of MV. Considering that the evidence for interventions involving SBTs using a T-piece is limited due to the small sample size of previous studies, and there is no trial regarding intervention during SBTs with pressure support, it is important to conduct a randomized trial to determine the effect of this intervention following a successful SBT using a T-piece and a separate trial after SBT on pressure support.
This study also tested the protocol, interventions, case report form, and data collection system. In addition, it identified areas to be improved in the large trials, such as the adherence to ventilatory support after extubation. The main differences between our feasibility trials and those of Fernandez et al. and Dadam et al.^( 1 , 2 )^ are presented in the Supplementary Material . If large clinical trials demonstrate a reduction in extubation failure within 7 days, the impact on critically ill patients could be significant, as extubation failure dramatically increases the risk of healthcare-associated infections (especially ventilator-associated pneumonia), length of hospital stay, mortality, and costs.^( 11 )^
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fernandez MM González-Castro A Magret M Bouza MT Ibañez M García C Reconnection to mechanical ventilation for 1 h after a successful spontaneous breathing trial reduces reintubation in critically ill patients: a multicenter randomized controlled trial Intensive Care Med 20174311166016672893667510.1007/s 00134-017-4911-0 · doi ↗ · pubmed ↗
- 2Dadam MM Gonçalves AR Mortari GL Klamt AP Hippler A Lago JU The effect of reconnection to mechanical ventilation for 1 hour after spontaneous breathing trial on reintubation among patients ventilated for more than 12 hours: a randomized clinical trial Chest 202116011481563367699710.1016/j.chest.2021.02.064 · doi ↗ · pubmed ↗
- 3Boles JM Bion J Connors A Herridge M Marsh B Melot C Weaning from mechanical ventilation Eur Respir J 2007295103310561747062410.1183/09031936.00010206 · doi ↗ · pubmed ↗
- 4Girard TD Alhazzani W Kress JP Ouellette DR Schmidt GA Truwit JD ATS/CHEST Ad Hoc Committee on Liberation from Mechanical Ventilation in Adults. An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Rehabilitation Protocols, Ventilator Liberation Protocols, and Cuff Leak Tests Am J Respir Crit Care Med 201719511201332776259510.1164/rccm.201610-2075 ST · doi ↗ · pubmed ↗
- 5Schönhofer B Geiseler J Dellweg D Fuchs H Moerer O Weber-Carstens S Prolonged Weaning: S 2k Guideline Published by the German Respiratory Society Respiration 2020991111023330226710.1159/000510085 · doi ↗ · pubmed ↗
- 6Thille AW Gacouin A Coudroy R Ehrmann S Quenot JP Nay MA REVA Research Network. Spontaneous-breathing trials with pressure-support ventilation or a T-piece N Engl J Med 202238720184318543628631710.1056/NEJ Moa 2209041 · doi ↗ · pubmed ↗
- 7François B Bellissant E Gissot V Desachy A Normand S Boulain T Association des Réanimateurs du Centre-Ouest (ARCO). 12-h pretreatment with methylprednisolone versus placebo for prevention of postextubation laryngeal oedema: a randomised double-blind trial Lancet 20073699567108310891739830710.1016/S 0140-6736(07)60526-1 · doi ↗ · pubmed ↗
- 8Jaber S Chanques G Matecki S Ramonatxo M Vergne C Souche B Post-extubation stridor in intensive care unit patients. Risk factors evaluation and importance of the cuff-leak test Intensive Care Med 200329169741252802510.1007/s 00134-002-1563-4 · doi ↗ · pubmed ↗