Portal Venous Gas After Trans-arterial Radioembolization in Hepatocellular Carcinoma: A Rare but Critical Imaging Finding
Ahmed Ali Aziz, Nosheen Omar, Rehan Shah, Muhammad Ali Aziz, Ijlal Akbar Ali

TL;DR
This paper reports the first case of portal venous gas after a treatment called trans-arterial radioembolization for liver cancer, highlighting a rare but important side effect.
Contribution
The paper presents the first documented case of portal and variceal venous gas following trans-arterial radioembolization for hepatocellular carcinoma.
Findings
Portal and variceal venous gas was observed in a patient after Y90 TARE for HCC.
The patient's symptoms resolved with antibiotic treatment and improved on follow-up imaging.
This finding suggests a new potential complication of TARE therapy.
Abstract
Transarterial radioembolization (TARE) is a relatively new treatment option available for unresectable hepatocellular carcinoma (HCC). TARE therapy involves the delivery of radiation directly to the tumor to cause tumor necrosis. Yttrium-90 (Y90) is commonly used as a source of radioembolization in TARE. TARE is very well tolerated and has a low rate of complications. Main complications of TARE for HCC include postembolization syndrome and radiation-induced injury to nearby organs such as the liver, gallbladder, and stomach, causing hepatitis, cholecystitis, or gastric ulceration. A side effect not previously described in TARE literature is portal venous gas after TARE therapy. We present the first ever reported case of portal and variceal venous gas in a 77-year-old male patient who had unresectable HCC and had previously failed chemotherapy. He underwent Y90 TARE for HCC. Following…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
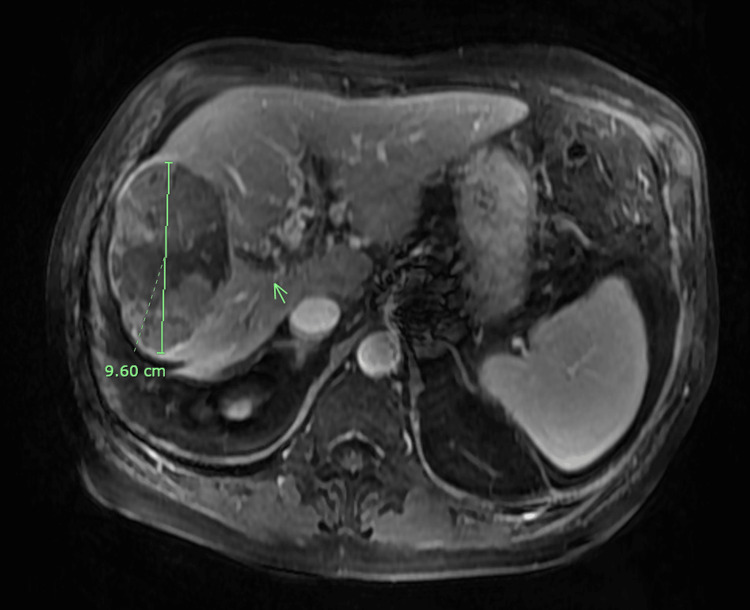 Figure 1
Figure 1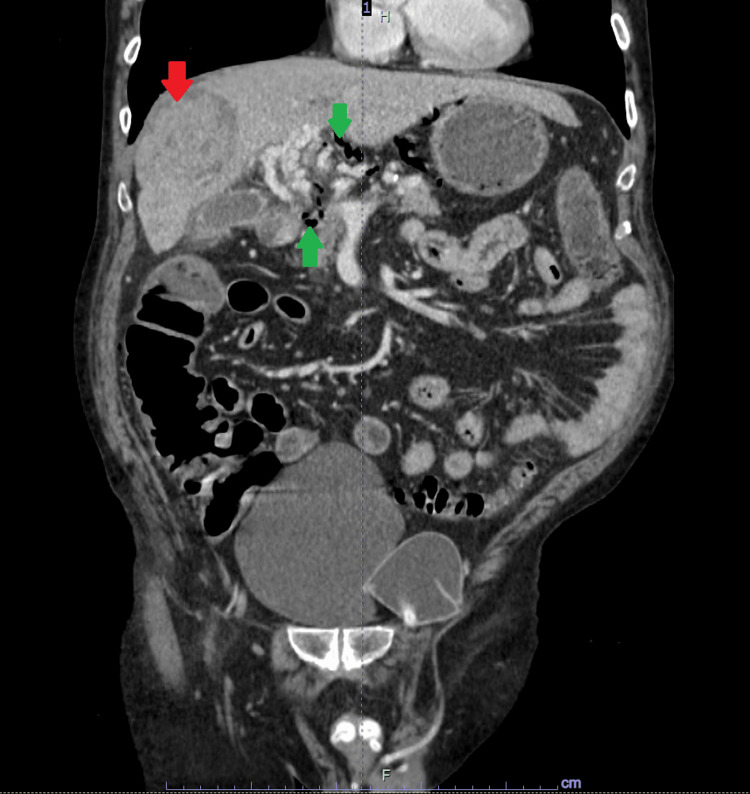 Figure 2
Figure 2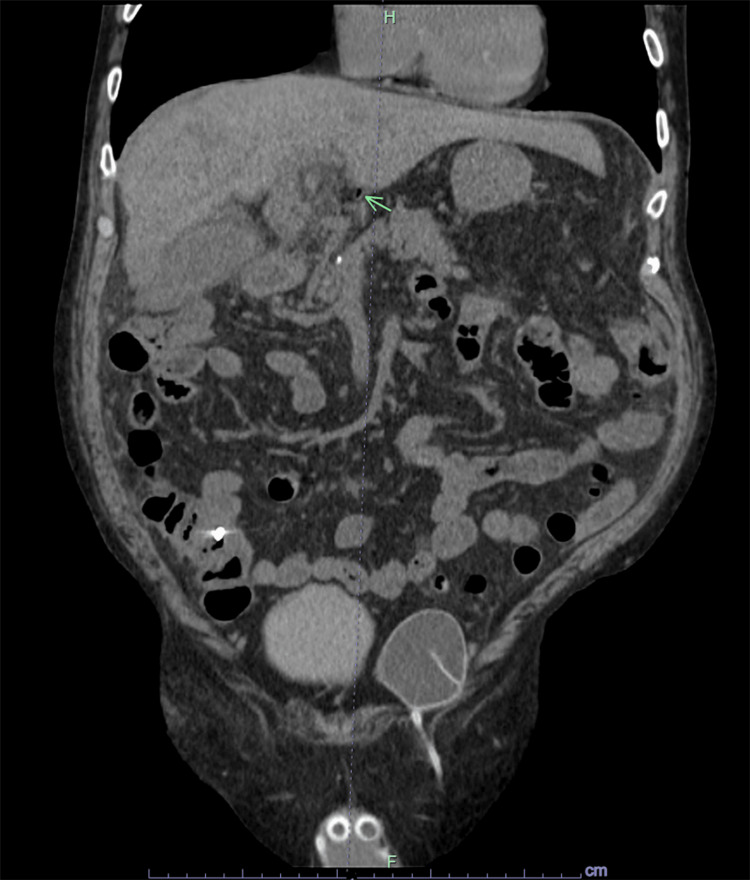 Figure 3
Figure 3| Lab Parameters (units) | Reference Range | Lab Result |
| Sodium (mmol/L) | 135 – 145 | 139 |
| Potassium (mmol/L) | 3.5 – 5.5 | 4.2 |
| Chloride (mmol/L) | 96 – 106 | 105 |
| BUN (mg/dL) | 6 – 24 | 16 |
| Creatinine (mg/dL) | 0.7 – 1.3 | 1.47 |
| Bicarbonate (mmol/L) | 22 – 29 | 20 |
| Glucose (mg/dL) | 70 - 100 | 96 |
| Aspartate Aminotransferase (U/L) | 13 – 39 | 36 |
| Alanine Aminotransferase (U/L) | 7 – 52 | 41 |
| Alkaline Phosphatase (U/L) | 34 – 104 | 98 |
| Total Bilirubin (mg/dL) | 0.2 – 1.3 | 0.8 |
| White Blood Cells (k/uL) | 3.8 – 10.2 | 6.2 |
| Hemoglobin (g/dL) | 12.9 – 16.7 | 13.6 |
| Hematocrit (%) | 39.2 – 48.8 | 43.0 |
| Platelets (k/uL) | 150 – 450 | 219 |
| International Normalized Ratio (INR) | 0.8 - 1.1 | 1.6 |
| Partial thromboplastin time (seconds) | 25 – 35 | 28 |
| Prothrombin Time (seconds) | 11 – 13.5 | 17 |
| Lactic Acid (mmol/L) | 0.90 – 1.60 | 1.30 |
| Clostridium difficile Toxin B Gene PCR | Not Detected | Not Detected |
| Campylobacter jejuni (TEM-PCR) | Not Detected | Not Detected |
| Cryptosporidium parvum | Not Detected | Not Detected |
| Enterohemorrhagic Escherichia Coli (EHEC) | Not Detected | Not Detected |
| Enteroinvasive Escherichia Coli (EIEC) | Not Detected | Not Detected |
| Enteropathogenic Escherichia Coli (EPEC) | Not Detected | Not Detected |
| Enterotoxigenic Escherichia Coli (ETEC) | Not Detected | Not Detected |
| Giardia lamblia | Not Detected | Not Detected |
| Norovirus | Not Detected | Not Detected |
| Rotavirus | Not Detected | Not Detected |
| Salmonella Enterica (TEM-PCR) | Not Detected | Not Detected |
| Shiga-Like Toxin Gene (STX1) | Not Detected | Not Detected |
| Shiga-Like Toxin Gene (STX2) | Not Detected | Not Detected |
| Vibrio Parahaemolyticus (TEM PCR) | Not Detected | Not Detected |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Abdominal vascular conditions and treatments · Heme Oxygenase-1 and Carbon Monoxide
Introduction
Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related mortality worldwide. It is the sixth most common malignancy in the world [1]. The treatment for HCC is based on staging, which considers tumor characteristics, liver function, and overall patient health. The Barcelona Clinic Liver Cancer (BCLC) staging system is a widely used staging system for HCC and categorizes HCC into five stages (0, A, B, C, and D) to guide treatment decisions. Curative treatments like surgical resection or liver transplant are considered for early stages (0 and A), while treatments like TACE or systemic therapy are used for advanced stages (B and C). Patients with end-stage disease (D) receive supportive care and palliation [2].
Transarterial radioembolization (TARE) is a relatively new treatment option for unresectable HCC [3,4]. TARE therapy involves the use of Yttrium-90 (Y90) radiation therapy directed selectively to the hepatic segments with tumor to induce necrosis by occlusion of the vessel feeding the tumor. TARE works on the principle that primary and secondary hepatic tumors are usually vascularized by arterial blood supply, while healthy liver tissue obtains blood supply mostly from the portal network. Hence, TARE has a low side effects profile as therapy is directed directly to the tumor through the arterial supply, and surrounding structures are spared [5]. Common complications include pain, fever, nausea, and vomiting, often termed as postembolization syndrome (PES), along with radiation-induced injury to neighboring organs, causing hepatitis, gastritis, and cholecystitis [6]. Portal and variceal venous gas after TARE therapy is a side effect not previously found in TARE literature, secondary to radiation-induced necrosis of HCC. Here, we present a case of a 77-year-old man with a history of nonresectable HCC and underlying cirrhosis who underwent TARE therapy and presented with right upper quadrant abdominal pain associated with diarrhea. Imaging revealed portal and variceal venous gas. He was started on antibiotics, his symptoms improved, and repeat imaging showed improvement in portal and variceal venous gas.
Case presentation
A 77-year-old man presented to our emergency department with generalized abdominal pain and multiple episodes of new-onset non-bloody diarrhea ongoing for the past six days. He denied any nausea or vomiting. He had a past medical history of liver cirrhosis secondary to hepatitis C virus, BCLC Stage B infiltrative HCC with thrombosis in the main, right, and left portal veins that was diagnosed 2 - 3 months prior to presentation to our ER, hypertension, and esophageal varices. He had previously received bevacizumab and atezolizumab therapy for treatment of HCC, which were discontinued due to hematochezia. He underwent TARE of segment VIII of the HCC lesion using Y90 radiation eight days ago. His magnetic resonance imaging (MRI) of the abdomen with and without intravenous (IV) contrast, done two months prior to his TARE procedure, showed a 9.6 cm HCC lesion in segment VIII of the liver (Figure 1).
Magnetic resonance imaging of the abdomen with and without contrast transverse section. The green line shows the 9.6 cm hepatocellular carcinoma in the right lobe of the liver. The green arrow points at the hepatocellular carcinoma nodules in the periphery of the large lesion.
On presentation, his vital signs were stable. His blood pressure was 135/85 mmHg, his pulse was 68 beats per minute, he was afebrile and had a respiratory rate of 18 respirations/minute, and his oxygen saturation was 98% on room air. On physical exam, his abdomen was soft, non-distended, with generalized tenderness to palpation and normal bowel sounds. His blood work was significant for normal complete cell count, normal lactic acid levels, and elevated creatinine to 1.47 mg/dL. Blood cultures and stool testing including Clostridium difficile and gastrointestinal (GI) biofire panel were sent (Table 1).
A computed tomography (CT) scan of the abdomen and pelvis (A&P) with IV contrast was done due to abdominal pain. The CT scan showed moderate portal venous gas in the intra-gastric, peri-gastric, and hepatic hilar varices with stable 10 cm partially necrotic mass within the right lobe of the liver compatible with his history of recently treated hepatocellular carcinoma with Y90 therapy (Figure 2).
Computed tomography scan of the abdomen and pelvis with intravenous contrast. Portal venous gas is indicated by green arrows. Partially necrotic right hepatic lobe hepatocellular carcinoma treated with Y90 therapy is indicated by a red arrow.
The CT A&P did not show any inflammatory conditions of the small or large bowel, emphysematous gastritis, perforated viscus, and obstruction, and the patient denied any retching or vomiting. The portal venous gas was thought to be secondary to recent Y90 radiation therapy to the HCC causing disseminated necrosis in the tumor and production of gas from gas-forming bacteria in necrotic HCC causing dissemination of gas into portal venous system. He was started on antibiotic piperacillin-tazobactam and IV fluids. Hepatology service was consulted and agreed with infectious workup, antibiotics and recommended repeating CT A&P after 48 hours to assess portal venous gas burden. Patient’s diarrhea improved and his clostridium difficile and GI panel were negative. Blood cultures remained negative, and his abdominal pain improved. His creatinine normalized and he was advanced to regular diet. A repeat CT A&P showed marked improvement and reduction in portal venous gas (Figure 3).
Computed tomography scan of the abdomen and pelvis with intravenous contrast showing improvement in portal venous gas indicated by a green arrow.
He was discharged on oral ciprofloxacin and metronidazole for seven days in a stable condition with outpatient follow-up with his oncologist and hepatologist.
Discussion
HCC is one of the leading causes of liver-related deaths worldwide [7]. TARE is a new treatment option for unresectable HCC [3,4]. TARE has been shown to increase the time of progression of HCC [8]. Radioembolization with TARE involves the injection of intra-arterial radioactive microspheres like the Y90, which targets the tumor of interest, leading to vessel occlusion and hence causing ischemia and necrosis of the target tumor [9].
TARE therapy generally has good tolerability and a low incidence of complications. This is because pre-procedure angiograms are used to assess vascular distribution to the tumor prior to performing TARE to minimize radioembolization to normal tissues [10]. However, complications still do arise due to the irradiation of non-target tissues, including the tumor-free liver segments [11,12]. The main complications of TARE for HCC are generally classified into PES, GI ulceration, hepatic dysfunction, biliary injury, lymphopenia, and radiation pneumonitis [10].
PES is the most common complication after TARE therapy. It presents as clinical symptoms of nausea and vomiting, fatigue, fever, abdominal discomfort, and anorexia, usually within 72 hours of the procedure [13]. Radiation-induced liver damage secondary to TARE therapy is characterized as liver injury in the form of jaundice, liver enzyme derangement, ascites, and elevated alkaline phosphatase [14]. TARE can lead to toxic effects on neighboring organs and cause radiation-induced gastritis, enteritis, or gastroduodenal ulcerations [10]. The clinical course is usually self-limited [15]. Radiation-induced injury to biliary structures might cause gallbladder wall thickening and signs of cholecystitis on imaging. The incidence of cholecystitis post-TARE requiring intervention is low [16]. Migration of Y90 radiation microspheres to pulmonary vasculature from hepatic vasculature can lead to radiation pneumonitis and pulmonary fibrosis [10]. TARE therapy might also cause mild to moderate lymphopenia; however, an increased susceptibility to infections has not been demonstrated [17].
Our patient was a 77-year-old man with a history of nonresectable HCC. He had previously failed treatment with Avastin and Tecentriq. He presented with non-bloody diarrhea and abdominal pain eight days after receiving Y90 TARE therapy. Infectious etiology was ruled out with a negative GI panel, Clostridium difficile testing, and negative blood cultures, which demonstrates the possibility of this being an unusual complication of TARE therapy. His imaging showed portal and variceal venous gas, thought to be secondary to the Y90 radiation therapy to the HCC, causing disseminated necrosis with gas production in the tumor and portal venous system. His clinical condition improved after antibiotic initiation. To our knowledge, this is the first reported case of portal venous gas reported in a patient with HCC after TARE. The TARE procedure is considered to be relatively safe, and patients are usually discharged after the procedure without requiring inpatient monitoring. Our case report is important as it alerts clinicians to be aware of the possibility of late-onset complications such as portal venous gas, like in our patient, which might require hospitalization and treatment with antibiotics.
Conclusions
TARE is becoming a popular option for the treatment of HCC. It is a relatively safe procedure and has low post-procedure complications, but as with any therapy, knowledge of the potential complications of this therapy is essential. Common complications arise from radiation-induced injury to nearby organs such as the stomach, gallbladder, and liver. TARE is offered as an outpatient treatment, and patients are usually not observed in the hospital. Our case report highlights an important post-procedure complication of TARE, i.e., the development of portal and variceal venous gas, likely from radiation-induced necrosis of HCC. Since our patient presented eight days after his TARE therapy and had necrotic HCC on imaging without inflammatory conditions of the small or large bowel, emphysematous gastritis, perforated viscus, or obstruction on imaging, it was reasonable that necrotic HCC and portal venous gas were from his recent TARE therapy.
Physicians should be aware of late-onset complications of TARE and should educate their patients about these complications. Patients should be asked to seek care in the hospital if they develop abdominal pain and diarrhea post-TARE therapy. Our case report is also important as it adds to the limited literature available on TARE, which is a relatively new treatment option for HCC and is still being explored. Future systemic literature reviews or multicenter research will help elucidate the mechanistic aspects and incidence of such complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Unique situation of hepatocellular carcinoma in Egypt: a review of epidemiology and control measures World J Gastrointest Oncol Ezzat R Eltabbakh M El Kassas M 191919381320213507003310.4251/wjgo.v 13.i 12.1919 PMC 8713321 · doi ↗ · pubmed ↗
- 2Hepatocellular carcinoma: current therapeutic algorithm for localized and advanced disease J Oncol Jose A Bavetta MG Martinelli E Bronte F Giunta EF Manu KA 3817724202220223662480110.1155/2022/3817724 PMC 9825221 · doi ↗ · pubmed ↗
- 3Transarterial chemoembolization in hepatocellular carcinoma treatment: Barcelona clinic liver cancer staging system World J Gastroenterol Han K Kim JH 10327103352120152642095910.3748/wjg.v 21.i 36.10327 PMC 4579879 · doi ↗ · pubmed ↗
- 4Heterogeneity of patients with intermediate (BCLC B) Hepatocellular Carcinoma: proposal for a subclassification to facilitate treatment decisions Semin Liver Dis Bolondi L Burroughs A Dufour JF 3483593220122339753610.1055/s-0032-1329906 · doi ↗ · pubmed ↗
- 5Radioembolization with Yttrium-90 microspheres in hepatocellular carcinoma: role and perspectives World J Hepatol Mosconi C Cappelli A Pettinato C Golfieri R 738752720152591477410.4254/wjh.v 7.i 5.738PMC 4404379 · doi ↗ · pubmed ↗
- 6Radioembolization with yttrium-90 microspheres work up: Ppactical approach and literature review Diagn Interv Imaging Vesselle G Petit I Boucebci S Rocher T Velasco S Tasu JP 5475629620152477681010.1016/j.diii.2014.03.014 · doi ↗ · pubmed ↗
- 7Hepatitis C virus and hepatocellular carcinoma: a narrative review J Clin Transl Hepatol Axley P Ahmed Z Ravi S Singal AK 7984620182960730810.14218/JCTH.2017.00067 PMC 5863002 · doi ↗ · pubmed ↗
- 8Y 90 radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma Gastroenterology Salem R Gordon AC Mouli S 1155116315120162757582010.1053/j.gastro.2016.08.029PMC 5124387 · doi ↗ · pubmed ↗