Cost-Effectiveness of Early Versus Late Interventional Radiology Drainage in Necrotizing Pancreatitis: A Decision Analysis Based on Cost Utility and Budget Impact
Rami Ahmad, Osborne P Vaz, Laken Boochoon, Maria Korontzi, Caroline Wolstenholme, Rami Obeidallah

TL;DR
This study finds that early interventional radiology drainage for necrotizing pancreatitis is more cost-effective than late drainage, with shorter ICU stays and lower costs.
Contribution
The study introduces a decision analysis model to compare the cost-effectiveness of early versus late IR drainage in necrotizing pancreatitis.
Findings
Early IR drainage was associated with shorter ICU stays and fewer drainage sessions compared to late drainage.
Total costs were lower in the early drainage group, with slightly higher quality-adjusted life years.
The budget impact analysis projected annual healthcare savings of £75,835 with early intervention.
Abstract
Introduction: The optimal timing of interventional radiology (IR) drainage in patients with necrotizing pancreatitis remains uncertain. This study compares the cost-effectiveness of early (five to six weeks) vs. late (> six weeks) IR drainage using a decision analysis model. Methods: A retrospective cohort of 76 patients with severe necrotizing pancreatitis (2017-2021) was screened. Twenty-two patients met the inclusion criteria and were included in a decision analysis model; 11 underwent early IR drainage and 11 underwent late IR drainage. Costs, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratios (ICERs) were calculated. A budget impact analysis was also conducted. Results: Early IR drainage was associated with shorter ICU stays (mean 17 vs. 26 days, p=0.01) and fewer IR drainage sessions (median 12 vs. 28, p=0.04) compared to late drainage. Readmissions…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
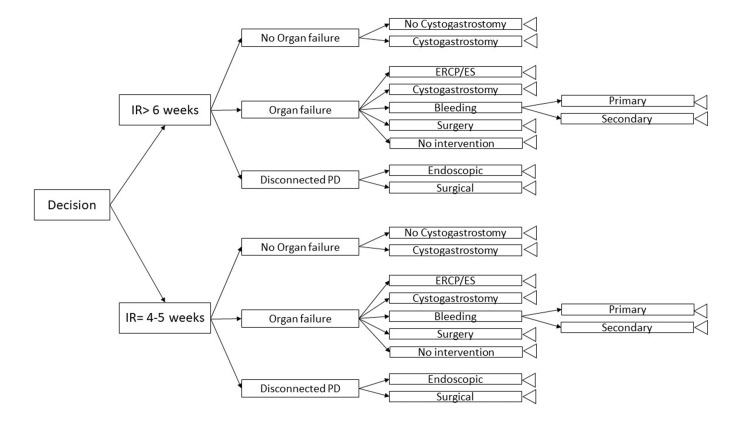 Figure 1
Figure 1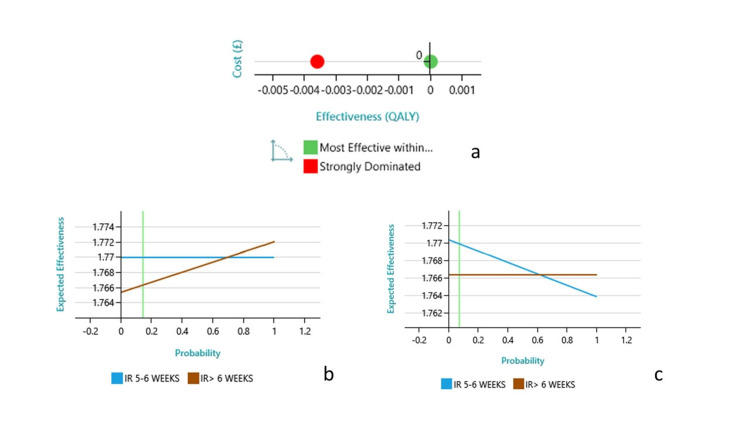 Figure 2
Figure 2| Parameters | Estimate | Standard error | Wald statistic | p-value |
| Intercept | 7.08673 | 0.045721 | 24025.22 | <0.001 |
| Number of IR sessions* | -0.15453 | 0.010102 | 233.98 | <0.001 |
| Days of first IR since onset | 0.00073 | 0.000269 | 7.39 | 0.006 |
| Number of readmissions | 0.99740 | 0.008999 | 12285.54 | <0.001 |
| System dysfunction | -3.29953 | 0.033770 | 9546.53 | <0.001 |
| Endoscopy | 0.08727 | 0.014958 | 34.04 | <0.001 |
| Bleeding | -1.51307 | 0.014049 | 11599.66 | <0.001 |
| Disconnected pancreatic duct | -1.80792 | 0.021621 | 6992.29 | <0.001 |
| Surgery/Bowel ischaemia/fistula | 0.22059 | 0.011676 | 356.93 | <0.001 |
| Activity | 2017 | 2018 | 2019 | 2020 | All year total costs (£) | N | Costs of activity per patient (£) |
| All other tests | 3365.72 | 2126.93 | 13076.40 | 8273.97 | 26843.02 | 76 | 353.20 |
| Anaesthesia | 1944.23 | 1253.85 | 1412.94 | 1150.84 | 5761.86 | 76 | 75.81 |
| Biochemistry | 3295.75 | 1292.48 | 9558.17 | 5595.00 | 19741.40 | 76 | 259.76 |
| Cellular sciences | 118.14 | 4.92 | 474.56 | 411.10 | 1008.72 | 76 | 13.27 |
| CNST indemnity | 25435.70 | 20549.57 | 45747.47 | 39507.41 | 131240.15 | 76 | 1726.84 |
| Dispensing blood products and factor products | 2402.02 | 1107.47 | 1823.11 | 1165.30 | 6497.90 | 76 | 85.50 |
| Dispensing high-cost drugs (on the list) | – | – | 7586.93 | 1318.95 | 8905.88 | 76 | 117.18 |
| Dispensing non-patient-identifiable medicines | 3450.88 | 3404.74 | 10311.56 | 8799.59 | 25966.77 | 76 | 341.67 |
| Dispensing high-cost drugs (duplicate entry) | – | 1409.28 | 7143.89 | 2451.83 | 11005.00 | 76 | 144.80 |
| Fluoroscopy | 7.95 | – | 120.54 | 97.11 | 225.60 | 76 | 2.97 |
| Hematology | 1824.54 | 1850.37 | 5965.20 | 4202.45 | 13842.56 | 76 | 182.14 |
| Microbiology | 1080.71 | 449.15 | 348.09 | 233.51 | 2111.46 | 76 | 27.78 |
| MRI | 519.87 | 744.44 | 242.28 | 118.11 | 1624.70 | 76 | 21.38 |
| No activity required | – | 1114.32 | 29336.10 | 30826.74 | 61277.16 | 76 | 806.28 |
| Diagnostic imaging: primary bleeding | 6510.62 | – | 20057.35 | 3513.49 | 30081.46 | 4 | 4377.28 |
| Diagnostic imaging: primary and secondary bleeding | – | – | – | 16045.88 | 16045.88 | 1 | 16045.88 |
| Other multidisciplinary team meetings | 175.68 | 142.17 | 1489.07 | 1414.49 | 3221.41 | 76 | 42.39 |
| Outpatient care | – | – | 272.13 | 141.35 | 413.48 | 76 | 5.44 |
| Outreach contacts | – | 7114.67 | 8070.68 | 5508.53 | 20693.88 | 76 | 272.29 |
| Pharmacy (other activity) | 1749.71 | 7233.23 | 22217.70 | 18810.65 | 50011.29 | 76 | 658.04 |
| Plain film | 132.03 | 201.92 | 257.35 | 145.63 | 736.93 | 76 | 9.70 |
| Readmission | 16356.97 | 24685.00 | 87315.19 | – | 128832.00 | 9 | 14315.00 |
| Ultrasound | 387.83 | 1132.53 | 3222.40 | 2529.11 | 7271.87 | 76 | 95.68 |
| Ward care | 97269.59 | 98207.02 | 218493.22 | 215221.56 | 629191.39 | 76 | 8278.83 |
| CT-scan | 3168.11 | 4514.30 | 3439.57 | 2205.27 | 13327.25 | 76 | 175.36 |
| Support services | 1882.41 | 11775.38 | 14592.49 | 14107.33 | 42357.61 | 15 | 2823.84 |
| Supporting contacts | 7226.08 | 9486.92 | 58831.46 | 36405.73 | 111950.19 | 15 | 7463.35 |
| Endoscopy | 4176.28 | 3762.53 | 14338.65 | 13885.97 | 36163.43 | 27 | 1339.39 |
| Prosthesis, implant, or device insertion | – | 1292.48 | 9558.17 | 5595.00 | 16445.65 | 27 | 609.10 |
| Surgical care | 6714.20 | 6518.47 | 7065.27 | 6505.82 | 26803.76 | 11 | 2436.71 |
| Time period | Clinical characteristics/Events | QALY value | Measurement tool | Reference |
| 4 months | ICU stay >25 days | 0.63 | PCS*, SF-36 | [ |
| 4 months | No ICU stay or ICU stay <25 days | 0.76 | PCS, SF-36 | [ |
| >4–12 months | Pain, analgesic use, readmissions, recurrent/chronic pancreatitis, diabetes | 0.70 | PCS, SF-36 | [ |
| >12–24 months | Not specified | 0.80 | PCS, SF-36 | [ |
| Characteristic | Early IR drainage (n=11) | Late IR drainage (n=11) | p-value |
| Age (mean ± SD) | 56.2 ± 14.1 | 58.6 ± 13.7 | 0.68 |
| Gender (M/F) | 07-Apr | 06-May | 0.68 |
| ASA Grade | 0.81 | ||
| ASA I | 1 | 0 | |
| ASA II | 3 | 2 | |
| ASA III | 5 | 6 | |
| ASA IV | 2 | 3 | |
| Comorbidities | |||
| Diabetes mellitus | 4 | 5 | 0.66 |
| Hypertension | 5 | 6 | 0.68 |
| Ischemic heart disease | 3 | 4 | 0.64 |
| Chronic kidney disease | 2 | 3 | 0.61 |
| COPD | 2 | 2 | 1 |
| Etiology of pancreatitis | 0.86 | ||
| Biliary | 7 | 5 | |
| Alcohol-induced | 3 | 4 | |
| Idiopathic | 1 | 1 | |
| Post-ERCP | 0 | 1 |
| Outcome | Early IR (n = 11) | Late IR (n = 11) | Statistical test | p-value | Factors impacted |
| Readmissions | 4 | 8 | Fisher’s exact test | 0.31 | Costs/Quality of life |
| IR sessions (median) | 12 | 28 | Mann–Whitney U test | 0.04 | Costs |
| ICU stay (mean) | 17 days | 26 days | Mann–Whitney U test | 0.01 | Quality of life |
| Surgery (including ischemia/fistula) | 2 | 2 | Fisher’s exact test | 1 | Costs/Quality of life |
| Disconnected pancreatic duct | 3 | 2 | Fisher’s exact test | 1 | Costs/Quality of life |
| Primary bleeding | 1 | 2 | Fisher’s exact test | 1 | Costs/Quality of life |
| Secondary bleeding | 0 | 1 | Fisher’s exact test | 1 | Costs/Quality of life |
| Terminal | Total payoffs |
| IR> 6 weeks | |
| → Chance → No organ failure → Chance → No cystogastrostomy | 1.77 QALY; £29,168 |
| → Chance → No organ failure → Chance → Cystogastrostomy | 1.77 QALY; £31,116 |
| → Chance → Organ failure → Chance → ERCP/ES | 1.78 QALY; £40,794 |
| → Chance → Organ failure → Chance → Cystogastrostomy | 1.76 QALY; £43,352 |
| → Chance → Organ failure → Chance → Surgery | 1.76 QALY; £41,892 |
| → Chance → Organ failure → Chance → No intervention | 1.76 QALY; £39,455 |
| → Chance → Disconnected duct → Chance → Endoscopic management | 1.77 QALY; £31,116 |
| → Chance → Disconnected duct → Chance → Surgical management | 1.77 QALY; £32,944 |
| → Chance → Organ failure → Chance → Bleeding → Chance → Primary | 1.76 QALY; £44,441 |
| → Chance → Organ failure → Chance → Bleeding → Chance → Secondary | 1.76 QALY; £56,110 |
| IR 5-6 weeks | |
| → Chance → No organ failure → Chance → Cystogastrostomy | 1.77 QALY; £23,533 |
| → Chance → No organ failure → Chance → No cystogastrostomy | 1.77 QALY; £21,584 |
| → Chance → Disconnected duct → Chance → Surgery | 1.77 QALY; £25,360 |
| → Chance → Disconnected duct → Chance → Endoscopic intervention | 1.77 QALY; £23,533 |
| → Chance 2 → Organ failure → Chance → No intervention | 1.77 QALY; £31,872 |
| → Chance 2 → Organ failure → Chance → Surgery | 1.77 QALY; £34,308 |
| → Chance 2 → Organ failure → Chance → Cystogastrostomy | 1.77 QALY; £35,768 |
| → Chance 2 → Organ failure → Chance → ERCP/ES | 1.77 QALY; £33,211 |
| → Chance 2 → Organ failure → Chance → Bleeding→ Chance → Secondary | 1.76 QALY; £48,526 |
| → Chance 2 → Organ failure → Chance → Bleeding → Chance → Primary | 1.76 QALY; £36,858 |
| Metric | Early IR drainage | Late IR drainage | Increment/difference |
| Average cost per patient (£) | £23,533 – £35,768 | £29,168 – £56,110 | Early is £5,635 – £20,342 less costly |
| Quality-adjusted life years (QALYs) | 1.77 years | 1.76 years | +0.01 QALYs (slight improvement) |
| Incremental cost-effectiveness ratio (ICER) | – | – | £15,340.96 per QALY gained (early vs. late) |
| Year | Current period (Year 0) | 2022/23 | 2023/24 | 2024/25 | 2025/26 | 2026/27 |
| Eligible population | 16 | 16 | 16 | 16 | 16 | 16 |
| Uptake of IR drainage at five to six weeks (%) | 100% | 100% | 100% | 100% | 100% | 100% |
| Number of people using new technology | 16 | 16 | 16 | 16 | 16 | 16 |
| Pathway description | Cost (£) |
| No organ failure → Cystogastrostomy | 29,168 |
| No organ failure → No cystogastrostomy | 31,116 |
| Disconnected duct → Surgery | 40,794 |
| Disconnected duct → Endoscopic | 43,352 |
| Organ failure → No intervention | 41,892 |
| Organ failure → Surgery | 39,455 |
| Organ failure → Cystogastrostomy | 31,116 |
| Organ failure → ERCP/ES | 32,944 |
| Organ failure → Bleeding → Secondary intervention | 44,441 |
| Organ failure → Bleeding → Primary intervention | 56,110 |
| Pathway description | Cost (£) |
| No organ failure → Cystogastrostomy | 23,533 |
| No organ failure → No cystogastrostomy | 21,584 |
| Disconnected duct → Surgery | 25,360 |
| Disconnected duct → Endoscopic | 23,533 |
| Organ failure → No intervention | 31,872 |
| Organ failure → Surgery | 34,308 |
| Organ failure → Cystogastrostomy | 35,768 |
| Organ failure → ERCP/ES | 33,211 |
| Organ failure → Bleeding → Secondary intervention | 48,526 |
| Organ failure → Bleeding → Primary intervention | 36,858 |
| Year | 2022/23 | 2023/24 | 2024/25 | 2025/26 | 2026/27 |
| Total cost of current practice (£) | 3,90,388 | 3,90,388 | 3,90,388 | 3,90,388 | 3,90,388 |
| Total cost of future practice (£) | 3,14,553 | 3,14,553 | 3,14,553 | 3,14,553 | 3,14,553 |
| Net budget impact (£) | -75,835 | -75,835 | -75,835 | -75,835 | -75,835 |
| Clinical event/Intervention | Number of patients | Notes/Details |
| Organ/system dysfunction | 13 | 59% of total patients |
| Endoscopic cystogastrostomy with necrosectomy | 3 | Total of six sessions |
| ERCP performed | 10 | Includes both diagnostic and therapeutic |
| Bleeding complications | 4 | Three primary bleeds, one secondary delayed |
| Pancreatic duct disruption requiring transpapillary stenting | 5 | - |
| Surgical intervention (bowel ischemia or fistula) | 4 | - |
| Readmission post-discharge | 12 | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Pancreatic and Hepatic Oncology Research · Gastrointestinal disorders and treatments
Introduction
Severe acute pancreatitis (AP) is a life-threatening disease following a natural course consisting of early severe AP and late severe AP. The management of infected necrotizing pancreatitis is associated with prolonged hospital stays and high costs [1]. Antibiotics are administered, and intervention is postponed as long as possible in cases of proven or suspected infected pancreatic necrosis in the initial four weeks after onset of disease [2], but it is a worldwide practice for expectant management after the initial four weeks as well in stable or mildly septic patients. However, antimicrobial therapy to reduce systemic illness from the infected necrosis may lead to increased incidence of *Candida *infections and antibiotic resistance [3].
Interventional procedures are generally only performed in cases of suspected or confirmed infection of pancreatic necrosis or peripancreatic necrosis alone [2].
It is unclear whether mildly ill patients with sterile necrosis and a degree of systemic toxicity should undergo any form of invasive therapy, including debridement. It is credible, however, that inpatients with sterile necrosis who clinically deteriorate despite aggressive supportive therapy may benefit from percutaneous catheter drainage [1, 4, 5]. An international survey among expert pancreatologists has demonstrated “equipoise” between immediate and postponed catheter drainage of infected necrotizing pancreatitis [6].
Evidence of benefits from early intervention has started accumulating in recent literature: in a published systematic review of percutaneous catheter drainage as primary treatment for necrotizing pancreatitis, it was found that no additional surgical necrosectomy was required after percutaneous catheter drainage in 55.7% [7]. The Patients With Infected Necrotizing Pancreatitis (POINTER) trial is the first randomized controlled trial designed to determine the optimal timing of catheter drainage in infected necrotizing pancreatitis [8].
To the best of our knowledge, only a few studies have been conducted to compare clinical experience with primary CT-guided percutaneous catheter drainage in patients with sterile necrosis with the same drainage procedure in patients with infected necrosis. The effect of clinical comorbid conditions, such as multisystem organ failure, on the outcome of primary CT-guided percutaneous catheter drainage in patients with sterile necrosis has not been assessed.
Sugimoto et al. found better outcomes of early and proactive use of percutaneous drainage during the course of necrotizing pancreatitis (lower incidences of organ failure, need for necrosectomy, and in-hospital mortality) [9]. The use of a preemptive percutaneous catheter drainage protocol early, before the development of severe sepsis, appeared to be effective.
Walser et al. found that the presence of sterile necrosis did not confer a more favorable patient outcome. The patients with sterile necrosis presumably had a higher mortality since their clinical presentation was much inferior to that of patients with infected necrosis. This observation reinforces the hypothesis, validated by other investigators [10].
Our aim was to define the optimal timing of radiological intervention for abdominal collections between five to six weeks and > six weeks in patients with absent or mild organ dysfunction during the late phase of acute necrotizing pancreatitis. For this, we conducted a cost-effectiveness decision analysis using our hospital database and data from the international literature.
Materials and methods
This retrospective study was conducted at East Lancashire Teaching Hospitals NHS Trust, Blackburn, UK, and included anonymized data from 76 patients admitted with severe necrotizing pancreatitis and abdominal collections between 2017 and 2021. Clinical and economic data such as hospital length of stay, ICU admissions, organ dysfunction, collection characteristics, procedures (radiological, endoscopic, surgical), complications, readmissions, and direct medical costs were organized using Microsoft Excel (Microsoft Corp., Armonk, NY).
A literature review from 2010 to 2021 was performed via Medical Literature Analysis and Retrieval System Online (MEDLINE), PubMed, and Cochrane Library, focusing on necrotizing pancreatitis-related terms including cystogastrostomy, image-guided drainage, cholangitis, bleeding complications, and Short Form-36 (SF-36) health survey scores. Systematic reviews and clinical guidelines were prioritized [8,11,12].
Inclusion criteria were patients aged ≥18 years diagnosed with necrotizing pancreatitis and radiologically confirmed abdominal collections, hospitalized for over four weeks, with recurrent or new collections, and initial single organ dysfunction or less. Exclusion criteria included absence of collections, drainage within four weeks of onset, interhospital transfer, multi-organ failure, known ductal disruption or minimal fluid collections [12], chronic pancreatitis, pancreatic malignancy, and death within two years of follow-up.
Interventional radiology (IR) drainage was classified as early (five weeks post-onset) or late (> six weeks). Clinical outcomes such as readmissions, number of IR sessions, ICU stay, surgeries, pancreatic duct disruption, and bleeding were compared between groups using Fisher’s exact test for categorical data and the Mann-Whitney U Test for continuous variables. These analyses informed economic modeling by identifying cost- and quality-of-life-related variables.
Quality-adjusted life years (QALYs) were the primary outcome, reflecting survival duration and quality (0 = death, 1 = perfect health). Utility values were derived from published sources [13]. The incremental cost-effectiveness ratio (ICER) was calculated as the cost difference divided by the QALY difference; a negative ICER indicates dominance. Cost-effectiveness was interpreted using UK willingness-to-pay (WTP) thresholds [13,14]. One-way sensitivity analyses assessed model robustness by varying individual parameters [13].
A decision tree was built using Decision Tree Analyzer v3.7.1 (Spicelogic Inc., Ontario, Canada), incorporating clinical and economic outcomes (Table 1, Figure 1).
Decision analysis model to examine the cost-effectiveness of the two strategies for the optimal timing of interventional radiology (IR) procedure.PD: pancreatic duct; ERCP: endoscopic retrograde cholangiopancreatography; ES: endoscopic sphincterotomy
The model compared IR drainage timing groups, accounting for possible clinical courses including organ failure, duct syndrome, cystogastrostomy, endoscopic retrograde cholangiopancreatography (ERCP), bleeding, surgery, or conservative recovery. Outcome probabilities were based on cohort data and literature.
QALYs were calculated from SF-36 Physical Component Summary (SF-36 PCS) scores across three intervals: 0 to four months, four to 12 months, and 12 to 24 months [15-17]. Cost data per patient and intervention are summarized in Tables 2, 3.
The model assumed all patients required IR drainage. Single-organ dysfunction occurred in ~41%, with progression to multi-organ failure included. Cystogastrostomy was anticipated in 10% to 14%, ERCP in 14% of biliary cases, bleeding complications in 6.5% (3% delayed), surgery in 14%, conservative recovery in 12.5%, and disconnected duct syndrome in ~19.7% [18]. Average readmissions ranged from 0.5 to one, and IR sessions from 1.2 to 1.9 per patient. Cost and utility inputs were drawn from institutional data and literature.
Cost-effectiveness was analyzed from a societal perspective with base-case and sensitivity analyses. A five-year budget impact analysis followed National Institute for Health and Care Excellence (NICE) digital health technology standards [19], using Mauskopf’s framework for care pathways and costs [16].
Statistical analysis predictors of total hospital costs were identified using generalized linear models (GLM) with maximum likelihood estimation. Group comparisons for clinical outcomes employed Fisher’s exact test for categorical variables and the Mann-Whitney U Test for continuous variables. Analyses were conducted using STATISTICA v7 (StatSoft Inc., Tulsa, OK).
Results
The systematic literature review found limited studies directly comparing early and late percutaneous catheter drainage in patients with sterile necrosis or infected necrosis without significant organ dysfunction [1,7,11,20]. Cost values for individual healthcare activities per patient, based on the entire 76-patient cohort, are presented in Table 2.
Among the 76 patients, 22 met the study’s inclusion criteria and underwent image-guided IR drainage. Baseline characteristics were similar between early and late IR groups, with comparable age, gender, American Society of Anesthesiologists (ASA) grades, and comorbidities. Biliary pancreatitis was more common in the early group; alcohol-related causes were slightly higher in the late group (Table 4).
These patients accounted for a total of 40 procedures and were evenly divided into early and late drainage groups. A decision-analysis model was employed to compare outcomes.
Patients in the early drainage group demonstrated better clinical outcomes. They had shorter ICU stays (17 vs. 26 days, p=0.01 by Mann-Whitney U Test), fewer readmissions (four vs. eight, p=0.31 by Fisher’s Exact Test), and required fewer IR drainage sessions (median 12 vs. 28, p=0.04 by Mann-Whitney U Test). Surgical intervention rates (including ischemia or fistula), rates of disconnected pancreatic duct syndrome, and bleeding complications (primary and secondary) were similar between groups, with no statistically significant differences (all p=1.00 by Fisher’s exact test). These outcomes were considered important drivers of both costs and quality of life (Table 5).
Over the two-year follow-up, the early group also accrued a slightly higher average QALY score (1.77 compared to 1.76 years), although the difference was modest (Table 6).
The average cost per patient was lower in the early drainage group, ranging from £23,533 to £48,526, compared to £29,168 to £56,110 in the late group (Table 6). The ICER for early drainage was calculated as £15,340.96 per QALY gained, which falls within the accepted WTP range in the UK of £20,000 to £30,000 per QALY (Table 7).
Multivariate regression identified several independent predictors of increased cost (Table 1). These included a higher number of IR drainage procedures, delayed drainage, an increased number of readmissions, the presence of organ dysfunction, the use of endoscopic interventions (including cystogastrostomy and necrosectomy), bleeding complications, duct disruption requiring stenting, and surgical interventions for bowel ischemia or fistula. Each of these factors contributed significantly to both the economic and clinical burden.
The budget impact analysis was based on the local population of East Lancashire, estimated at 377,111 people. With an annual pancreatitis incidence of 0.06%, approximately 207 patients were expected each year, of whom 30% would develop necrotizing pancreatitis. An estimated 16 of these patients would qualify for early IR drainage annually (Table 8).
Implementing early drainage in this group was projected to result in annual healthcare savings of £75,835 (Tables 9-11)
The decision-analysis model integrated empirical clinical data with real-world cost estimates and probabilities for clinical events. Early drainage consistently emerged as the dominant strategy across most scenarios with favorable clinical outcomes and economic efficiency. Visual representation of model outcomes is provided in Figure 2.
(a) Interventional radiology (IR) drainage within five to six weeks at the late phase of necrotizing pancreatitis is the preferred cost-effective option. Shifting cost-effectiveness towards the IR > six weeks option, there is a need for 70% of patients (probability 0.7) to have an early (endoscopic retrograde cholangiopancreatography) (ERCP) (for biliary pancreatitis) (b), or if bleeding is present in 60% of patients (c).The vertical green line in panels b and c indicates the base-case probability value used in the deterministic model. It serves as a reference point to assess how variations in the input probability influence the expected effectiveness of the two strategies.QALY: quality-adjusted life years
However, as shown in Figure 2, the one-way sensitivity analysis revealed two factors that could influence this outcome: if more than 70% of patients required early ERCP for biliary pancreatitis or if the bleeding complication rate exceeded 60%, late drainage could become more favorable.
Analysis of clinical events revealed that 13 patients (59%) experienced organ or system dysfunction. Endoscopic cystogastrostomy with necrosectomy was performed in three patients (across six sessions), and ERCP was conducted in 10 patients. Four patients experienced bleeding (three primary, one secondary), while five patients were diagnosed with disconnected pancreatic duct syndrome. Four patients required surgical intervention for bowel ischemia or fistula. In total, 12 patients were readmitted after discharge. These clinical events significantly influenced both outcomes and costs (Table 12).
Discussion
The aim of our decision analysis was to determine the optimal timing for IR percutaneous catheter drainage in patients with sterile pancreatic necrosis or infected necrosis with or without single organ dysfunction during the late phase of acute necrotizing pancreatitis. Our findings indicate that IR drainage at five to six weeks is more cost-effective than later drainage (> six weeks), offering both lower costs and slightly improved QALYs. The presence of a cost-effectiveness frontier for drainage at five to six weeks makes this timing an optimal choice, influenced mainly by biliary etiology rates and risks of bleeding. These conclusions remained robust across a wide range of model assumptions; for example, even a bleeding rate as high as 60% would not negate the cost-effectiveness of earlier drainage [21].
To the best of our knowledge, this is the only study that addresses the cost-effectiveness of CT-guided percutaneous catheter drainage in sterile and mildly infected necrosis within a late phase of the acute necrotizing pancreatitis population using a robust decision-analysis model.
Our analysis aligns with broader recommendations from the Institute for Clinical and Economic Review [22], which advocates combining (1) a systematic review of comparative effectiveness and (2) a de novo decision model informed by base-case parameters. We adhered to these principles, supplementing the literature where gaps existed with predictors derived from our own real-world clinical dataset.
Several recent studies further support the clinical and strategic relevance of our analysis. Van Veldhuisen et al., 2024 [23], compared early versus late drainage in necrotizing pancreatitis and emphasized improved patient-centered outcomes such as reduced complications and faster recovery in the early group. Similarly, findings from the POINTER trial (Boxhoorn et al., 2021) [24] have reinforced the relevance of timely, step-up interventions, especially where delayed drainage may lead to progression of sepsis or complications. These studies highlight the need for individualized, early interventions, which our economic analysis now validates from a cost-effectiveness and budget impact perspective.
From a health economics standpoint, our model suggests that decision-making for IR drainage should incorporate ICER thresholds, biliary disease burden, and anticipated bleeding risk. The analysis confirms that drainage at five to six weeks is not only clinically sound but also financially advantageous under the NHS framework.
Additionally, budget impact analysis (BIA) is essential alongside cost-effectiveness modeling. It estimates the financial implications of adopting early drainage strategies across NHS trusts, especially when considering the potential transfer of patients from district general hospitals. BIA supports real-world implementation by mapping costs to current service delivery constraints [13].
Our use of net benefit analysis confers advantages: it provides a direct comparison across strategies regardless of the number of alternatives, and it reduces the instability often associated with ICERs in scenarios where differences in effect size are small [25].
Our study has several limitations. Although we analyzed clinical outcomes, we did not include genetic risk factors such as SPINK1, IL-1β, or IL-10 mutations, which may influence disease severity [26]. The study was single-center with a relatively small sample size, limiting external generalizability. Costs from district general hospitals were not included for transferred patients. We did not evaluate health opportunity costs. The impact of pancreatitis on mental health and quality of life, especially in alcohol-related cases, was not considered due to a lack of robust published data. Finally, long-term morbidity costs, including follow-up for pseudocyst, endocrine, or exocrine insufficiency, were not incorporated.
Conclusions
In summary, early IR drainage performed at five to six weeks in necrotizing pancreatitis appears to be a cost-effective approach. It was associated with shorter ICU stays, fewer procedures, and lower overall costs, with comparable complication rates and a slight improvement in QALYs. The ICER was within accepted UK thresholds, and the budget impact analysis projected significant annual savings.
Although the sample size was limited and the study was conducted at a single center, the findings align with emerging clinical evidence supporting early intervention. Larger, prospective studies are needed to confirm these results and guide practice. Overall, early IR drainage may offer both clinical and economic advantages in appropriate patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1CT-guided percutaneous catheter drainage of acute necrotizing pancreatitis: clinical experience and observations in patients with sterile and infected necrosis AJR Am J Roentgenol MorteléKJ Girshman J Szejnfeld D Ashley SW Erturk SM Banks PA Silverman SG 11011619220091909818810.2214/AJR.08.1116 · doi ↗ · pubmed ↗
- 2A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome Gastroenterology van Santvoort HC Bakker OJ Bollen TL 1254126314120112174192210.1053/j.gastro.2011.06.073 · doi ↗ · pubmed ↗
- 3Timing of surgical intervention in necrotizing pancreatitis Arch Surg Besselink MG Verwer TJ Schoenmaeckers EJ 1194120114220071808698710.1001/archsurg.142.12.1194 · doi ↗ · pubmed ↗
- 4Role of percutaneous catheter drainage as primary treatment of necrotizing pancreatitis Turk J Gastroenterol Mehta V Kumar R Parkash S Singla S Singh A Chaudhary J Bains H 1841873020193045755910.5152/tjg.2018.17542 PMC 6408166 · doi ↗ · pubmed ↗
- 5Acute necrotizing pancreatitis: role of CT-guided percutaneous catheter drainage Abdom Imaging Segal D Mortele KJ Banks PA Silverman SG 3513613220071750298210.1007/s 00261-007-9221-5 · doi ↗ · pubmed ↗
- 6Diagnostic strategy and timing of intervention in infected necrotizing pancreatitis: an international expert survey and case vignette study HPB (Oxford) van Grinsven J van Brunschot S Bakker OJ 49561820162677685110.1016/j.hpb.2015.07.003PMC 4766363 · doi ↗ · pubmed ↗
- 7Systematic review of percutaneous catheter drainage as primary treatment for necrotizing pancreatitis Br J Surg van Baal MC van Santvoort HC Bollen TL Bakker OJ Besselink MG Gooszen HG 18279820112113656210.1002/bjs.7304 · doi ↗ · pubmed ↗
- 8Postponed or immediate drainage of infected necrotizing pancreatitis (POINTER trial): study protocol for a randomized controlled trial Trials van Grinsven J van Dijk SM Dijkgraaf MG 2392020193102338010.1186/s 13063-019-3315-6PMC 6482524 · doi ↗ · pubmed ↗