Resolution of tension pseudomeningocele complicating foramen magnum decompression for Chiari I malformation after ventriculoperitoneal shunt: A case report
Yi-Chen Lee, Yu-Feng Su, Hui-Yuan Su

TL;DR
A 15-year-old girl with a rare complication after surgery for a brain condition was successfully treated with a shunt to resolve cerebrospinal fluid leakage.
Contribution
This case report presents a successful treatment of tension pseudomeningocele using a ventriculoperitoneal shunt after foramen magnum decompression.
Findings
Tension pseudomeningocele can develop after foramen magnum decompression in Chiari I malformation patients.
A ventriculoperitoneal shunt effectively resolved the pseudomeningocele and cerebrospinal fluid leakage.
Cerebrospinal fluid diversion techniques can address pressure imbalances causing the condition.
Abstract
Tension pseudomeningocele is a rare complication that arose after foramen magnum decompression in a patient with Chiari I malformation and syringomyelia. This article presents a case that was effectively managed through cerebrospinal fluid diversion methods, highlighting the mechanisms involved and the treatment option used. A 15-year-old girl came to our clinic with allodynia in the right anterior chest wall that had lasted for six months. An MRI showed a type 1 Chiari malformation along with syringomyelia from C2 to C6. After performing foramen magnum decompression and duraplasty, there was an improvement in the syringomyelia; however, the patient developed a tension pseudomeningocele in the posterior fossa. She then had a ventriculoperitoneal shunt placed, which successfully resolved the tension pseudomeningocele and the cerebrospinal fluid leakage. Pseudomeningocele is a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
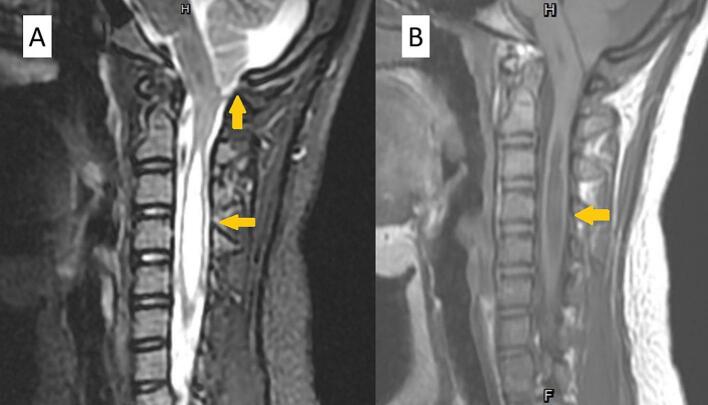 Figure 1
Figure 1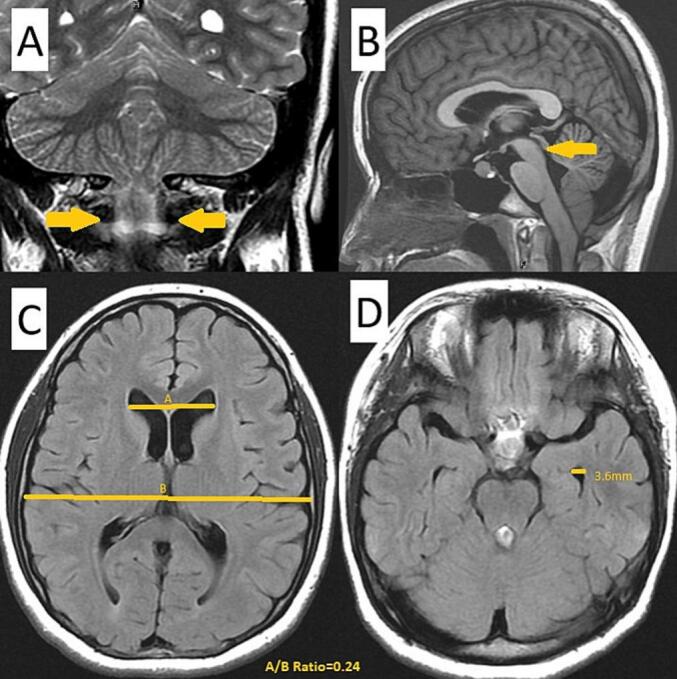 Figure 2
Figure 2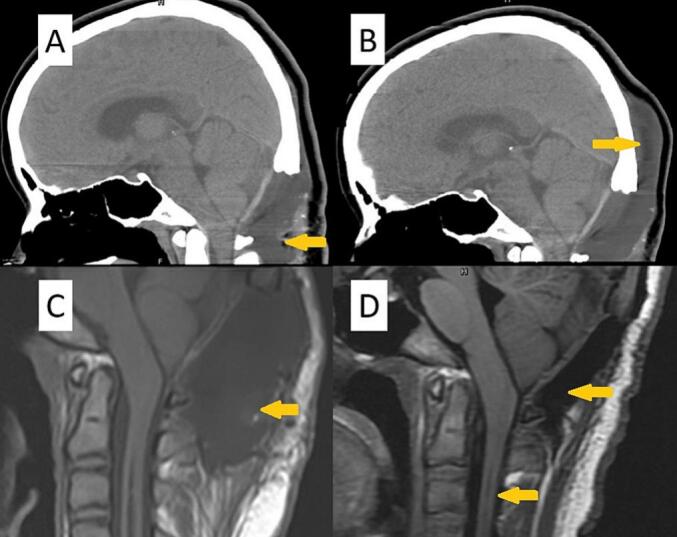 Figure 3
Figure 3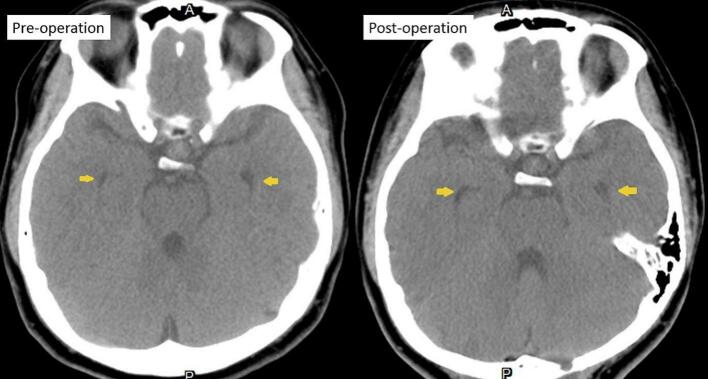 Figure 4
Figure 4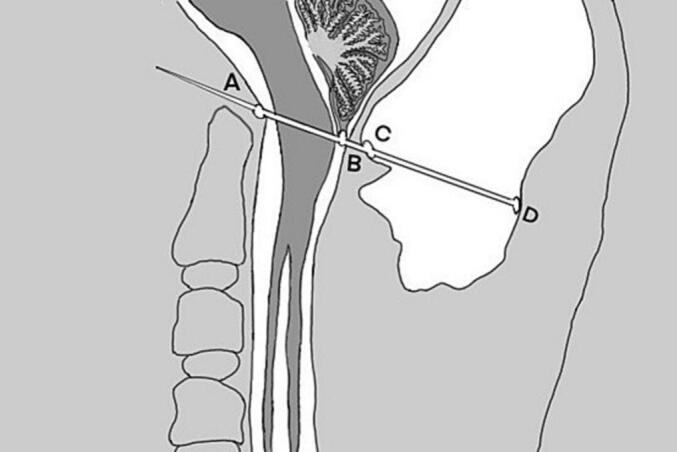 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Dysraphism and Malformations · Cerebrospinal fluid and hydrocephalus · Head and Neck Surgical Oncology
Introduction
1
Chiari I malformation is defined by the herniation of the cerebellar tonsils and a disruption in the dynamics of cerebrospinal fluid at the foramen magnum [1]. The prevalence of Chiari I malformation is estimated to range from 3 to 8 cases per 100,000 individuals; notably, approximately 65 % of those diagnosed with this condition also present with syringomyelia [2]. Presently, surgical intervention, specifically foramen magnum decompression with or without duraplasty, is the preferred treatment for Chiari I malformation accompanied by syringomyelia [3]. Potential complications arising from foramen magnum decompression surgery include infection, subdural collections, epidural fluid accumulation, pseudomeningocele, hydrocephalus, and persistent syringomyelia [3,4]. The occurrence of tension pseudomeningocele following foramen magnum decompression is considered rare [1]. This report presents an exceptionally rare case of tension pseudomeningocele subsequent to foramen magnum decompression in a patient with Chiari I malformation and syringomyelia. Also, it has been developed in accordance with the SCARE Guidelines, which are designed to promote thoroughness and transparency in the reporting of surgical case studies [5].
Case report
2
A 15-year-old female patient with a prior diagnosis of scoliosis presented with a tingling sensation localized to the anterior chest wall, persisting for a duration of six months. This discomfort intensified when the patient maintained a neck flexion posture for periods exceeding 15 min. Additionally, she reported episodes of chest tightness and soreness in the posterior neck and bilateral shoulders. Upon conducting a physical and neurological examination, the area of allodynia was identified at the anterior T3–4 dermatome, with no skin lesions evident on the anterior chest wall. Muscle strength in all four limbs was assessed as normal, and deep tendon reflexes did not exhibit hyperreflexia. The Babinski reflex indicated bilateral plantar flexion. The patient's gait was stable, and there were no signs of truncal ataxia or dysmetria. Proprioception testing yielded normal results. Given the clinical impression of T3–4 radiculopathy, a series of imaging studies were initiated. A plain radiograph of the spine showed signs of scoliosis, with a Cobb angle of 24.1°, which is a decrease from the 30° noted a year prior. Cervicothoracic magnetic resonance imaging (MRI) demonstrated the presence of syringomyelia spanning levels C2 to C6, as well as cerebellar tonsil herniation (Fig. 1). To further investigate the potential diagnosis of Chiari I malformation, a brain MRI was conducted, which indicated sagging of the bilateral cerebellar tonsils (Fig. 2A), the absence of aqueduct stenosis (Fig. 2B), and occult hydrocephalus characterized by an Evan's index of 0.24 (Fig. 2C) and a temporal horn width of 3.6 mm (Fig. 2D). Subsequent lumbar MRI did not reveal additional syringomyelia lesions. The radiological findings included a basal angle of 127.9°, a clivoaxial angle of 139.2°, a basilar impression of 4.5 mm, and tonsillar descent of 7.6 mm. Diagnosed with Chiari I malformation accompanied by C2 to C6 syringomyelia, the patient underwent foramen magnum decompression and duraplasty, with an uneventful surgical course. The patient was discharged on postoperative day 9, reporting improvement in allodynia. However, one week post-discharge, clear fluid was observed discharging from the surgical site, necessitating primary suture with gauze compression. Three weeks following the surgery, a brain computed tomography scan revealed a pseudomeningocele in the posterior fossa adjacent to the duraplasty site (Fig. 3A). After discussions with the patient and her family, conservative management with gauze compression was initiated. Nevertheless, the patient continued to experience persistent occipital headaches and cerebrospinal fluid leakage from the wound. A subsequent brain computed tomography scan indicated an enlargement of the pseudomeningocele with upward and epicranial extension after two weeks of conservative treatment (Fig. 3B), while no significant changes were noted in the size of the bilateral ventricular temporal horns (Fig. 4). Cervicothoracic MRI T1 revealed a tension pseudomeningocele extending into the occipital subgaleal space and partial resolution of the syringomyelia (Fig. 3C). In light of the tension pseudomeningocele complicating the foramen magnum decompression with duraplasty, a ventriculoperitoneal shunt was placed, with the programmable shunt pressure set to 100 mmH2O. One week following the shunt placement, there was a marked improvement in the pseudomeningocele and sustained resolution of the syringomyelia (Fig. 3D). In addition, improvement of headache and absence of cerebrospinal fluid leakage were noted.Fig. 1A. A sagittal T2-weighted magnetic resonance imaging (MRI) scan of the cervicothoracic region reveals a hyperintense signal within the spinal cord at the C2 to C6 levels, accompanied by observable spinal cord enlargement. B. A sagittal T1-weighted MRI of the cervicothoracic region demonstrates a hypointense signal at the C2 to C6 spinal cord levels, as well as spinal cord enlargement. Additionally, herniation of the cerebellar tonsils through the foramen magnum is observed.Fig. 1. Fig. 2presents the results of a brain magnetic resonance imaging (MRI) examination, which demonstrates the presence of bilateral cerebellar tonsil herniation (illustrated in Fig. 2A), the absence of aqueductal stenosis (depicted in Fig. 2B), and evidence of occult hydrocephalus, characterized by an Evan's index of 0.24 (shown in Fig. 2C) and a temporal horn width of 3.6 mm (as indicated in Fig. 2D).Fig. 2. Fig. 3A. Three weeks postoperatively, a non-enhanced brain computed tomography scan reveals a skull defect resulting from prior foramen magnum decompression surgery, as well as a pseudomeningocele located in the posterior fossa adjacent to the duraplasty site. B. A subsequent brain computed tomography scan demonstrates an exacerbation of the pseudomeningocele, characterized by upward and epicranial extension following two weeks of conservative management. C. A T1-weighted magnetic resonance imaging of the cervicothoracic region illustrates a tension pseudomeningocele extending into the occipital subgaleal space, alongside a partial resolution of syringomyelia. D. One week subsequent to the placement of a ventriculoperitoneal shunt, there is a notable improvement in the pseudomeningocele, with sustained resolution of the syringomyelia.Fig. 3. Fig. 4indicates that there is no statistically significant difference in the dimensions of the bilateral ventricular temporal horns when comparing preoperative and postoperative brain computed tomography images.Fig. 4
Discussion
3
Epidural fluid accumulation is a frequently encountered complication following foramen magnum decompression with duraplasty [3]. However, the persistent accumulation of epidural fluid and the subsequent development of a pseudomeningocele represent significant challenges that require attention. The literature indicates that the progressive enlargement of the pseudomeningocele can create a mass effect, which may lead to spinal cord edema and exacerbate syringomyelia [1]. There remains no definitive consensus regarding the closure of the durotomy post-surgery for foramen magnum decompression. The durotomy is often left open to facilitate the dissipation of cerebrospinal fluid (CSF) waves or to prevent pressure on the obex by enlarging the cisterna magna, thereby creating a pseudomeningocele. Alternative techniques, such as primary dural closure, duraplasty, or the use of a patch, which are prone to failure, may counteract the benefits of decompressive surgery performed via foramen magnum decompression [6].
The precise mechanism underlying the development of pseudomeningocele as a complication of foramen magnum decompression with duraplasty in patients with Chiari I malformation remains unclear. One proposed mechanism involves the dissipation of the CSF systolic pressure wave, which shifts from the obex to the expandable cavity of the pseudomeningocele [7]. This phenomenon may explain the observed resolution of syringomyelia alongside the continued enlargement of the pseudomeningocele following foramen magnum decompression. We hypothesize that the persistent craniospinal pressure gradient across the foramen magnum may contribute to the progressive development of pseudomeningocele after decompression surgery with duraplasty. Furthermore, CSF may enter the pseudomeningocele cavity through a flap valve, which results from the dural patch sutured to the aponeurosis. In cases of deterioration, the ongoing accumulation of CSF can lead to the formation of a tension pseudomeningocele [1].
To mitigate the imbalanced pulsations of CSF at the flap valve, it may be beneficial to address the leakage of CSF through the slit of the flap valve. Prior to the complete sealing of the duraplasty site, it is essential to attenuate the pulsatile CSF pressure gradient within the pseudomeningocele cavity. Potential interventions to achieve this include external ventricular drainage, ventriculoperitoneal shunt, and endoscopic third ventriculostomy [[8], [9], [10]]. Additionally, it has been reported that 5.1 % of patients with Chiari I malformation develop hydrocephalus following foramen magnum decompression, with 17 % of these individuals experiencing CSF leakage or pseudomeningocele formation. The shunting procedure is often regarded as the preferred treatment option [4]. In our case, mild dilation of the bilateral temporal horns of the ventricles was observed prior to foramen magnum decompression, although there were no clinical signs or symptoms indicative of hydrocephalus. Nevertheless, persistent CSF leakage and the enlargement of the pseudomeningocele were noted postoperatively. Given the suspicion of hydrocephalus-related progression of the pseudomeningocele and CSF leakage, we opted to perform a programmable ventriculoperitoneal shunt. Following posterior fossa decompression, the ventricular size did not exhibit enlargement. Although the hydrocephalus was not overtly apparent prior to the decompression, it appears to have contributed to the exacerbation of the tension pseudomeningocele. Significant improvements in tension pseudomeningocele and cerebrospinal fluid leakage were observed following shunting surgery. In addition to ventriculoperitoneal shunts, various strategies exist for addressing persistent pseudomeningocele after foramen magnum decompression. A notable drawback of external ventricular drainage is the heightened risk of infection, which leads us to exclude this option [11]. Endoscopic third ventriculostomy presents an alternative; however, we refrain from selecting this procedure due to its potential complications, which include intraventricular hemorrhage, intracerebral hemorrhage, and oculomotor nerve palsy [12].
Despite the numerous disadvantages associated with ventriculoperitoneal shunts—such as under-drainage, over-drainage, shunt malposition, infection, subdural hematoma, and hygroma—this approach appears to be an effective solution for managing progressive pseudomeningocele following foramen magnum decompression surgery [13]. A review of the literature identified seven cases of pseudomeningocele, allowing for the evaluation of pseudomeningocele size post-posterior fossa decompression. We calculated the ratio of pseudomeningocele in the posterior fossa using a defined formula (Fig. 5). To our knowledge, we present a case with the highest ratio of pseudomeningocele in the posterior fossa (Table 1). This literature review encompasses a total of seven patients, among whom one underwent a lumbar-peritoneal shunt, one received a ventriculoperitoneal shunt, one was treated solely with aspiration, and the remaining patients underwent duraplasty. All patients exhibited improvements in clinical symptoms and neurological deficits following appropriate management.Fig. 5presents a schematic representation illustrating the established formula for calculating the ratio of pseudomeningocele. The components are labeled as follows: A represents the basion, B denotes the tonsil, C indicates the dura mater, and D signifies the fascia of the scalp. The line segment AB extends and intersects the dura mater and the fascia of the scalp at points C and D, respectively. The ratio of the pseudomeningocele is defined as the distance between points C and D divided by the distance between points A and D.Fig. 5. Table 1Summary of Patients Characteristics in the Literature Review.Table 1. AuthorAge, yearsGenderInitial presentationTreatmentDural closurePMC ratioPresentationManagementof PMC[14]3Male.Chiari 1.Syrinx.Kleeblattschädel deformitySuboccipital craniectomyand C1 and C2 laminectomiesDurepair patch and running polydioxanone sutures0.28No clinical symptomsObservation[15]22Male.Chiari 1.SyrinxSuboccipital craniectomyAnd C1 laminectomyDura was left open0.4PMC with cord distortion.Draplasty with synthetic graft.Spinal cord adhesiolysis[16]33FemaleChiari 1Craniocervicaldecompression–0.55––[17]34FemaleChiari 1Suboccipital craniectomyand C1 laminectomyDuraplasty with periosteum and DuraGen XS0.53PMC with low-grade infection..Lumbar drain then lumbar peritoneal shunt. Duraplasty with muscular flap[18]54Female.Chiari 1.SyrinxSuboccipital craniectomyand C1 laminectomyDuraplasty with Seamdura and running 5–0 nylon suture.polyglycolic acid sheet.fibrin glue0.5Headache and nauseaAspiration[19]37MaleChiari 1Posterior fossa decompression surgery–0.25–**–**Lee et al.Female.Chiari 1.SyrinxSuboccipital craniectomy and C1 laminectomyDuraplasty with galea aponeurosis + simple interrupted suture + DuraSeal0.57Headache + cerebrospinal leakage from the woundVentriculoperitoneal ShuntNote. a: PMC as abbreviation of pseudomeningocele.
We propose that cerebrospinal fluid diversion techniques, such as pseudomeningocele-peritoneal shunt or ventriculoperitoneal shunt, may be crucial in alleviating pressure within the pseudomeningocele cavity and achieving a balance in the craniospinal pressure gradient between the wave at the obex and the pseudomeningocele cavity.
Conclusion
4
Tension pseudomeningocele is a possible complication that may arise after foramen magnum decompression accompanied by duraplasty in individuals diagnosed with Chiari I malformation. The mechanism contributing to this condition is likely linked to a persistent craniospinal pressure gradient between the obex and the adjacent cavity. The application of cerebrospinal fluid diversion techniques may play a crucial role in the management of tension pseudomeningocele in patients with Chiari I malformation.
Author contribution
Yi-Chen Lee conducted the collection and analysis of the results and authored the manuscript. Yu-Feng Su provided supervision for the paper. Hui-Yuan Su undertook the review of the article and assumed responsibility for data collection and processing. All authors engaged in discussions regarding the results and contributed to the final version of the manuscript.
Parental consent
Written informed consent was obtained from the patient's parents/legal guardian for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Consent
The patient's parents provided written informed consent for the publication and any related images.
Ethical approval
This study does not require ethical approval from our ethics committee.
Guarantor
Hui-Yuan Su.
Research registration number
Not applicable.
SCARE guideline
The study has been conducted in accordance with the SCARE guidelines.
Sources of funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of competing interest
All the authors have no financial and non-financial conflicts of interest relevant to this article to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nurboja B.Choi D.Extensive spinal cord oedema and early syrinx formation due to tension pseudomeningocele after foramen magnum decompression Br. J. Neurosurg.23420094434451963701910.1080/02688690802716137 · doi ↗ · pubmed ↗
- 2Zuev A.A.Kostenko G.V.Treatment of syringomyelia associated with Chiari 1 malformation. Zhurnal Nevrologii I Psikhiatrii Imeni S.S Korsakova 1173201710210610.17116/jnevro 201711731102-10628399105 · doi ↗ · pubmed ↗
- 3Ito K.Appropriate surgical procedures for Chiari type 1 malformation and associated syrinx based on radiological characteristics of the craniovertebral junction Neurosurg. Rev.43220205755803068410810.1007/s 10143-019-01079-3 · doi ↗ · pubmed ↗
- 4Bartoli A.Treatment options for hydrocephalus following foramen magnum decompression for Chiari I malformation: a multicenter study Neurosurgery 86420205005083123242710.1093/neuros/nyz 211 · doi ↗ · pubmed ↗
- 5Kerwan A.Al-Jabir A.Mathew G.Sohrabi C.Rashid R.Franchi T.Nicola M.Agha M.Agha R.A.Revised Surgical C Ase R Eport (SCARE) guideline: an update for the age of artificial intelligence Premier J. Sci.102025100079
- 6Kurzbuch A.R.Magdum S.CSF goes astray no matter what is in the way: occipital intradiploic pseudomeningocele and de novo syringomyelia following foramen magnum decompression for Chiari I malformation in a pediatric patient J. Neurosurg. Pediatr.20201610.3171/2019.12.PEDS 1942732032961 · doi ↗ · pubmed ↗
- 7ParéL.S.Batzdorf U.Syringomyelia persistence after Chiari decompression as a result of pseudomeningocele formation: implications for syrinx pathogenesis: report of three cases Neurosurgery 4341998945948976632510.1097/00006123-199810000-00125 · doi ↗ · pubmed ↗
- 8Perrini P.Extra-arachnoidal cranio-cervical decompression for syringomyelia associated with Chiari I malformation in adults: technique assessment Acta Neurochir.149102007101510221771251210.1007/s 00701-007-1276-0 · doi ↗ · pubmed ↗