Impact of clonal hematopoiesis of indeterminate potential on arterial atherothrombosis and venous thromboembolism: Protocol for a systematic review and meta-analysis
Angela Todorovski, Tzu-Fei Wang, Evan Sterling, Erin Collins, Marc Carrier, Deborah Siegal, Natasha Kekre, Roy Khalifé, Yan Xu

TL;DR
This study will review and analyze how clonal hematopoiesis of indeterminate potential affects the risk of arterial and venous blood clots.
Contribution
The study introduces a systematic review and meta-analysis protocol to clarify CHIP's role in thromboembolic events.
Findings
CHIP is associated with an increased risk of atherothrombosis, but results vary across studies.
The relationship between CHIP and venous thromboembolism remains poorly understood.
The impact of CHIP on health outcomes in patients with existing thromboembolic disease is unclear.
Abstract
Clonal hematopoiesis of indeterminate potential (CHIP) is a novel risk factor for thromboembolic events. While CHIP is linked to an increased risk of incident atherothrombosis (ATE), the link between these two conditions varies across studies. Furthermore, the association between CHIP and incident venous thromboembolism (VTE) has not yet been well characterized. Among patients with established ATE and VTE, it is still unclear how CHIP carriership influences their health outcomes. We aim to conduct a systematic review and meta-analysis to: i) determine the impact of CHIP carriership on incident ATE and VTE; and ii) evaluate the prevalence and clinical consequences of CHIP mutations among individuals with established ATE or VTE. We will search MEDLINE, EMBASE, Scopus and CINAHL for randomized trials, cohort studies, or case control studies reporting thromboembolic events among adult CHIP…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
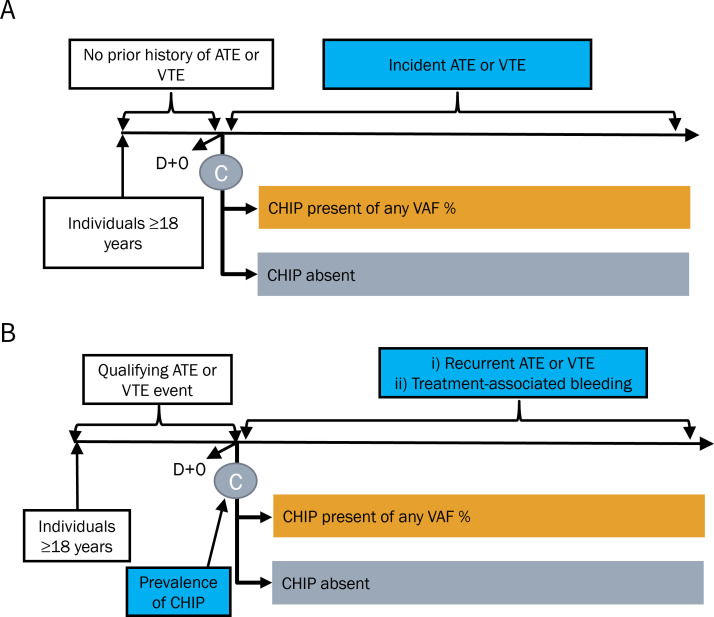 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Blood Coagulation and Thrombosis Mechanisms · Myeloproliferative Neoplasms: Diagnosis and Treatment
1. Introduction
One in four deaths worldwide are attributable to thrombosis, manifest as atherothrombosis (ATE, e.g., coronary artery disease, acute myocardial infarction, acute ischemic stroke, and peripheral artery disease) and venous thromboembolism (VTE, e.g., pulmonary embolism and deep vein thrombosis) [1]. Risks of ATE and VTE increase with age, and recent data have identified clonal hematopoiesis of indeterminate potential (CHIP), a set of age-dependent, inflammation-driven genetic changes in the hematopoietic system, as a novel predictor of ATE and VTE [2–4].
CHIP is defined as the presence of a somatic (acquired) mutation of a myeloid malignancy-associated gene with a variant allele fraction (VAF) of ≥2%, in the absence of a diagnosed hematologic disorder [5]. Over the past decade, CHIP has emerged as an important contributor to ATE. Using whole-exome sequencing data from two prospective cohorts that comprised 1,010 participants without a history of cardiovascular events, Jaiswal et al reported a 1.9-fold increased risk of ATE among CHIP carriers compared to their non-CHIP counterparts (odds ratio [OR] 1.9, 95% confidence interval [CI] 1.4 to 2.7) [2]. In the same report, a 4-fold increase in risk of early-onset myocardial infarction was observed among CHIP carriers compared to matched non-carriers among 7,245 participants who were less than 50 years of age at the time of their acute coronary syndrome [2].
An updated knowledge synthesis is needed for several reasons. First, while a systematic review and meta-analysis in 2022 reported a 1.6-fold increased risk of ATE among individuals with CHIP compared to those without CHIP (OR 1.6, 95% CI 1.3–2.1), more contemporary data with larger sample size (e.g., UK Biobank 500k cohort) have reported a much more modest impact of CHIP on ATE [6]. Second, increasing number of studies have now examined the impact of CHIP on VTE. For example, high prevalence of CHIP carriership has been observed among individuals with unprovoked pulmonary embolism [3], and the presence of CHIP has been associated with increased risks of incident VTE [7]. While the incidence of VTE is strongly correlated with increasing age [8], the impact of CHIP on VTE has not been summarized. Third, contemporary evidence indicates increased cardiovascular risk and mortality associated with CHIP detected far below 2% variant allele fraction (VAF) [9,10], a threshold that was originally established by detection limit associated with sequencing technologies [11]. There is heterogeneity in CHIP case identification due to differences in sequencing strategies (e.g., panel-based sequencing vs. whole genome sequencing), sequencing platforms (e.g., digital droplet polymerase chain reaction vs. next generation sequencing) and gene lists used for variant calling and curation. Finally, the prognostic impact of CHIP carriership on recurrent thromboembolic events and bleeding complications among adults with an established diagnosis of ATE or VTE has not been systematically reviewed.
2. Objectives
The primary objective of this systematic review and meta-analysis is to determine the impact of CHIP on the incidence of ATE and VTE among individuals with no previous history of thromboembolic disease. Secondary objectives are to: 1) determine the prevalence of CHIP among patients with first episode of ATE and VTE with stratification by their respective risk factors; and 2) evaluate the impact of CHIP on recurrent thromboembolism and treatment-related bleeding complications among patients with established ATE and VTE.
3. Methods
This protocol is reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) Statement (2015) [12]. Amendments to the current protocol, if required, will be reported in the final study report.
Eligibility criteria
Study design and characteristics,.
For the primary objective, we will include randomized controlled trials, prospective and retrospective cohort studies, and case-control studies. For the secondary objective, we will include aforementioned study types with addition of cross-sectional studies to capture CHIP prevalence.
We will include peer-reviewed published manuscripts. We will exclude case reports, case series, pre-prints, trial registries, protocols, or unpublished or non-peer reviewed studies, including grey literature. These exclusions are intended to ensure that each screened study has appropriate peer-review. The findings of relevant conference abstracts will only be included if a subsequent targeted search identifies a peer-reviewed manuscript of the same study at the time of data extraction. There will be no restriction based on the year, language, or geographical region. Non-English manuscripts will be translated using an online translation service [13].
Participants.
To determine the impact of CHIP on incident ATE or VTE, we will include studies that enrolled individuals aged 18 years of age or older without a prior history of ATE or VTE at the time of CHIP testing (Fig 1A).
Flow diagram for eligible studies evaluating populations without prior atherothrombosis or venous thromboembolism (A) and populations with established atherothrombosis and venous thromboembolism (B) of this systematic review and meta-analysis.ATE, atherothrombosis; VTE, venous thromboembolism, CHIP, clonal hematopoiesis of indeterminate potential; VAF, variant allele fraction.
To determine the prevalence and prognostic impact of CHIP among those with history of thromboembolism, we will include studies of patients 18 years of age or older with an established diagnosis of ATE or VTE at the time of their CHIP testing (Fig 1B). ATE includes one or more of the following: coronary artery disease, acute myocardial infarction, acute ischemic stroke, or peripheral arterial disease (as defined in individual studies). Similarly, VTE will be defined by one or more of the following: pulmonary embolism, deep vein thrombosis, or superficial vein thrombosis (as defined in individual studies). We will include VTE involving atypical sites, such as cerebral venous thrombosis and splanchnic vein thrombosis. Study definitions of qualifying ATE or VTE diagnoses will be recorded.
We will include individuals of any sex, gender, racial, ethnic and ancestry groups, and geographical location. We will not restrict patients based on use of antithrombotic or conditions associated with CHIP (e.g., cancer or receipt of anti-cancer therapy), and these characteristics will be included will be recorded if available. Consistent with the definition of CHIP, individuals with an established hematologic diagnosis (e.g., myelodysplastic syndrome, acute myeloid leukemia, myeloproliferative neoplasms) will be excluded.
Studies involving individuals <18 years of age at time of enrolment will be excluded, as CHIP is an age-related condition that is very rare to occur in the pediatric population [14].
Exposure/Comparators.
The exposure of interest is CHIP carriership. While CHIP is defined as variant allele frequency (VAF) ≥2%, we will not restrict by VAF in this systematic review and meta-analysis, based on emerging data that suggest increased thromboembolic risks associated with CHIP carriers with VAF < 2% [15–17]. The comparator group will be patients without CHIP carriership at any detectable VAF.
Outcomes.
The primary outcome will be ATE or VTE. ATE will include incident diagnosis of coronary artery disease, acute myocardial infarction, acute ischemic stroke, or peripheral artery disease [18]. Coronary artery disease will be defined by the 2023 AHA/ACC guideline, and includes individuals with angina symptoms (with or without imaging confirmation), those following acute myocardial infarction or after coronary revascularization procedure, and those with ischemic cardiomyopathy [19]. Acute myocardial infarction will be defined as per the 2018 Joint Task Force universal definition of MI, and will be inclusive of non-ST elevation myocardial infarction or ST elevation myocardial infarction [20]. Acute ischemic stroke will be defined as any neurological dysfunction caused by focal cerebral, spinal, or retinal infarction [21]. Peripheral artery disease will include ATE involving the upper or lower extremities, as well as cervical arteries (e.g., carotid artery stenosis).
VTE will be defined as imaging-confirmed diagnosis of pulmonary embolism, upper and lower extremity deep vein thrombosis, superficial vein thrombosis, or VTEs involving atypical sites, including cerebral venous thrombosis and splanchnic vein thrombosis. We will include incidental VTE and VTE of any clot burden, including subsegmental pulmonary embolism and isolated distal deep vein thrombosis. Studies that reported VTE outcomes without appropriate imaging will not be included.
If an included study did not specify the definition used to classify the outcome, diagnostic criteria as reported by the study will be used as the endpoint of interest and recorded.
As part of the secondary objective (Fig 1B), we will include studies that captured treatment-related bleeding complications as defined by the individual studies.
Information sources and search strategy
In collaboration with a research librarian (E.S.), a comprehensive systematic literature search will be performed using Medline, Embase, Scopus, and CINAHL from database inception to July 2024. A draft Medline search strategy is included in S1 Appendix and will be adapted across the other databases. We will use Medical Subject Heading (MeSH) terms with supplementation by keywords, with vocabulary and syntax adjusted based on the databases queried. The search has been designed with two concept groups: 1) Clonal hematopoiesis or genetic markers associated with CHIP, and 2) cardiovascular disease/ATE and VTE.
Data management
Search results from the included databases will be uploaded into Covidence ® (Alfred Hospital, Melbourne, Australia), and duplicate references will be excluded. Ten articles for level 1 (title and abstract) screening, and ten articles for level 2 (full text review) screening will be piloted by all study authors to ensure agreement in handling of inclusion/exclusion criteria. Studies with multiple publications (e.g., interim analyses, extended follow up publications) will be assessed as a single study by cross referencing trial name and registration, author name, and institution.
Selection process
At least two independent reviewers will use Covidence to screen titles and abstracts based on the pre-selected inclusion and exclusion criteria. At both level 1 (title and abstract) and level 2 (full text review) screening, each title, abstract, and eligible full text article will be assessed by two reviewers. Disagreements in screening will be resolved initially by discussion between the two reviewers, and eventually by a third and adjudicating reviewer if the conflict remains unresolved. Articles excluded at title and abstract screening and full text review will be recorded and presented in a PRISMA flow diagram. At full text review, reasons for exclusion will be selected by the reviewers and will be recorded in the flow chart. Study authors will not be blinded to the study title and author information. Additional notes or tags that are added by reviewers to the articles through the Covidence platform are also not blinded.
Data collection
A standardized data extraction form will be developed and piloted in Microsoft Excel to record author, publication year, study design, follow-up duration, number of patients (total and per intervention group) included, patient demographics, baseline ATE and VTE risk factors, CHIP detection methods, CHIP-related risk factors, and outcomes. Full list of data extracted are included in Table 1. Where an eligible study has multiple publications involving the same cohort of patients, outcomes for all studies will be collected in a single collection form. Data will be extracted by two authors independently, and each study will be extracted in duplicate. All reviewers will pilot extraction data for one study. Any discrepant data fields will be resolved by consensus, with a third and adjudicating reviewer to resolve any conflicts that remain.
Table 1: Data to be extracted from included studies.
Risk of bias in individual studies
Risk of bias assessment will be conducted by two reviewers independently using the QUIPS tool, which is used to evaluate the prognosis studies [22]. Studies will be analyzed based on five bias domains (S2 Appendix): study participation, study attrition, prognostic factor measurement, outcome measurements, study confounding, and statistical analysis and reporting. Each of the categories will be scored using the following four descriptions: yes (low risk of bias), probably yes, probably no, and definitely no (high risk of bias). A high risk of bias is assigned if a study contains ≥1 domains as “definitely no”, or ≥2 domains marked as “definitely no” or probably no”. A low risk of bias is assigned if all domains are assessed as “probably yes” or “definitely yes.” All other studies will be considered as unclear risk of bias. Disagreements will be resolved by discussion between the two reviewers, with involvement of a third reviewer if necessary.
Data synthesis
To determine the association between CHIP and occurrence of ATE or VTE, we will derive pooled ORs with 95% CIs at the study level. Additionally, we will pool the incidence/ recurrence rates (reported as events per person-years) and rate ratios using data from randomized controlled trials, prospective cohort and retrospective cohort studies. Each arm of a randomized trial will be treated as a prospective cohort for this step. We will generate pooled summary statistics using logit transformation of proportions, followed by inverse-variance weighted random effects meta-analysis using the DerSimonian and Laird model for CHIP carriers and non-carriers [23]. If there are insufficient and heterogenous data to perform meta-analysis at the subgroup level, a narrative synthesis will be done. A descriptive summary of the key characteristics of each of the included studies will be tabulated.
To determine the prevalence of CHIP carriership, we will analyze individuals with CHIP mutations as proportion of all ATE and VTE patients at each study level. This will be followed by transformation of proportions and random-effects meta-analysis using the DerSimonian and Laird method detailed above. Heterogeneity between studies will be assessed using visual inspection and the I² statistic. We plan to perform complete case analysis as primary analysis while capturing the proportion of missing primary outcomes of interest. When missingness of a specific outcome is ≥ 5% among included studies, we will perform four assumptions as sensitivity analyses: best case scenario, none of the participants with missing data had the outcome, all participants with missing data had the outcome, and worse case scenario.
We will conduct subgroup analyses to assess the robustness of the association between CHIP and thromboembolic outcomes by the following potential variables provided sufficient data are available: age, sex, self-reported race, ethnicity and ancestry, geographical location of the reported study, high-risk CHIP as defined by VAF ≥ 10%, specific CHIP-defining genes (e.g., DNMT3A, TET2, ASXL1, JAK2), presence of hyperlipidemia, obesity, smoking, hypertension, VTE associated with a persistent risk factor (e.g., active malignancy, autoimmune conditions), VTE associated with a transient risk factors (e.g., surgery, immobilization, acute medical illness, COVID-19 infections), VTE associated with no observed risk factor (e.g., unprovoked VTE), and presence of family history. Interaction testing will be performed to determine subgroup effects, and its associated Chi-squared statistic and p-value will be reported.
We will perform sensitivity analyses by excluding studies with high risk of bias using the QUIPS tool, and studies using adjudicated ATE and VTE endpoints rather than those reported in routine clinical care (e.g., administrative database coding). If at least ten studies are extracted in the primary analysis, publication bias will be visually assessed using funnel plots and through Egger’s test.
Finally and data permitting, we will assess the strength of the body of evidence using the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach [24]. The QUIPS tool will be incorporated into the GRADE process as part of rating for risk of bias.
Dissemination
This systematic review and meta-analysis will use publicly available information; as such, research ethics approval will not be required. While handling of individual patient-level data are not expected in context of this study-level systematic review and meta-analysis, we will seek appropriate ethics approval and data sharing agreements if individual patient-level data are required. Search strategy, extraction protocols, and handled discrepancies will be reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines [25]. We aim to submit this work for presentation at an international conference and submit our results for publication in a peer-reviewed journal. Extracted data used for data synthesis will be available to researchers upon request to the corresponding author, upon completion and publication of this systematic review and meta-analysis.
4. Conclusions
Despite the evolving role of CHIP as a novel cardiovascular biomarker, the prognostic impact of CHIP for incident ATE and VTE remain uncertain. Furthermore, the clinical consequences of carrying CHIP mutations among those with established ATE and VTE remain poorly understood. Our systematic review and meta-analysis will establish summary estimates on CHIP’s performance as a prognostic tool, thereby informing the net clinical benefit associated with CHIP screening in the general population and individuals with established cardiovascular disease. This is especially relevant given the lack of consensus recommendations on CHIP screening [26]. In addition, no interventional study has prospectively incorporated CHIP to evaluate its performance as a predictive variable to inform precision prevention of cardiovascular disease despite promising post-hoc data [27]. Therefore, our study outputs will also inform both primary and secondary prevention strategies that incorporate CHIP in adequately powered interventional trials. By understanding the intersection between ATE, VTE and CHIP, our research output will improve the understanding of this thrombo-inflammatory nexus and catalyze innovative research aimed at reducing the global burden of ATE and VTE through CHIP-directed therapies.
Supporting information
S1 AppendixMedline search strategy.(DOCX)
S2 AppendixComponents of the Quality in Prognosis Studies (QUIPS) tool for risk of bias assessment.(DOCX)
S1 FilePRISMA-P-checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Goldhaber SZ, Bounameaux H. Pulmonary embolism and deep vein thrombosis. Lancet. 2012;379(9828):1835–46. doi: 10.1016/S 0140-6736(11)61904-1 22494827 · doi ↗ · pubmed ↗
- 2Jaiswal S, Natarajan P, Silver AJ, Gibson CJ, Bick AG, Shvartz E, et al. Clonal hematopoiesis and risk of atherosclerotic cardiovascular disease. N Engl J Med. 2017;377:111–21.28636844 10.1056/NEJ Moa 1701719 PMC 6717509 · doi ↗ · pubmed ↗
- 3Soudet S, Jedraszak G, Evrard O, Marolleau JP, Garcon L, Pietri MAS. Is hematopoietic clonality of indetermined potential a risk factor for pulmonary embolism? TH Open. 2021;5(3):e 338–42. doi: 10.1055/s-0041-1733856 34414354 PMC 8370792 · doi ↗ · pubmed ↗
- 4Zon B, Sekar A, Clapham K, Niroula A, Bick AG, Gibson CJ, et al. Clonal Hematopoiesis and venous thromboembolism in the UK Biobank. Blood. 2023;142(Supplement 1):568–568. doi: 10.1182/blood-2023-180764 · doi ↗
- 5Marnell CS, Bick A, Natarajan P. Clonal hematopoiesis of indeterminate potential (CHIP): linking somatic mutations, hematopoiesis, chronic inflammation and cardiovascular disease. J Mol Cell Cardiol. 2021;161:98–105. doi: 10.1016/j.yjmcc.2021.07.004 34298011 PMC 8629838 · doi ↗ · pubmed ↗
- 6Kessler MD, Damask A, O’Keeffe S, Banerjee N, Li D, Watanabe K, et al. Common and rare variant associations with clonal haematopoiesis phenotypes. Nature. 2022;612(7939):301–9. doi: 10.1038/s 41586-022-05448-9 36450978 PMC 9713173 · doi ↗ · pubmed ↗
- 7Zon RL, Sekar A, Clapham K, Oren O, Niroula A, Bick AG, et al. JAK 2-mutant clonal hematopoiesis is associated with venous thromboembolism. Blood. 2024;144(20):2149–54. doi: 10.1182/blood.2024024187 39102652 PMC 11600088 · doi ↗ · pubmed ↗
- 8White RH. The epidemiology of venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I 4-8. doi: 10.1161/01.CIR.0000078468.11849.66 12814979 · doi ↗ · pubmed ↗