Genetic association of preeclampsia to von Willebrand factor and its size-regulator ADAMTS13
A. Inkeri Lokki, Michael Triebwasser, Emma Daly, Mitja I. Kurki, Markus Perola, Kirsi Auro, Anuja Java, Jane E. Salmon, Seppo Heinonen, Eero Kajantie, Juha Kere, Riitta Lassila, Mark Daly, John P. Atkinson, Hannele Laivuori, Seppo Meri

TL;DR
This study finds that genetic variants in von Willebrand Factor and ADAMTS13 are linked to preeclampsia, a pregnancy-related vascular disorder.
Contribution
The study identifies specific genetic variants in VWF and ADAMTS13 associated with preeclampsia and suggests a novel therapeutic target.
Findings
A common VWF variant rs1800385 increases preeclampsia risk.
A low-frequency ADAMTS13 variant rs41314453 is linked to preeclampsia and reduces enzyme activity.
Impaired ADAMTS13 function may promote large VWF polymers, contributing to preeclampsia pathogenesis.
Abstract
Preeclampsia is a common pregnancy-specific vascular disorder that develops during the second half of pregnancy. Preeclampsia shares features with thrombotic microangiopathies. Here we analyzed whether sequence variants in the coagulation system genes predispose to preeclampsia. We performed targeted exomic sequencing of 58 genes in a total of 615 preeclamptic women and 2094 controls. A common missense variant rs1800385 (Val1565Leu) in the gene coding for von Willebrand Factor (VWF) (OR=1.72, p-value=3.57E-4) and a low-frequency missense variant rs41314453 (Ala732Val) in the gene coding for a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS13) (OR=1.97, p-value=0.044) were associated with preeclampsia. rs41314453 is known to decrease ADAMTS13 expression and activity. Thus, the reduced enzyme activity could promote the formation of large vWF…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
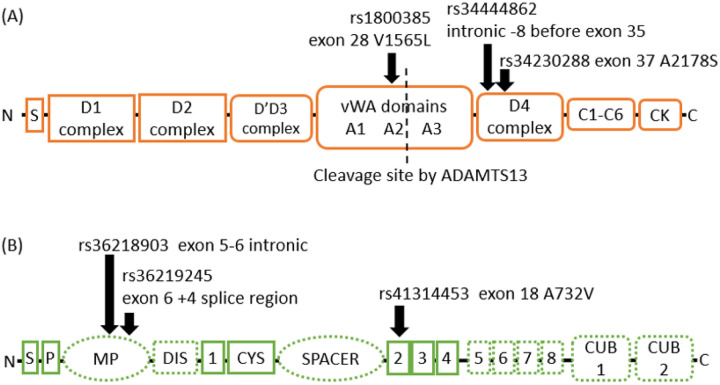 Figure 1
Figure 1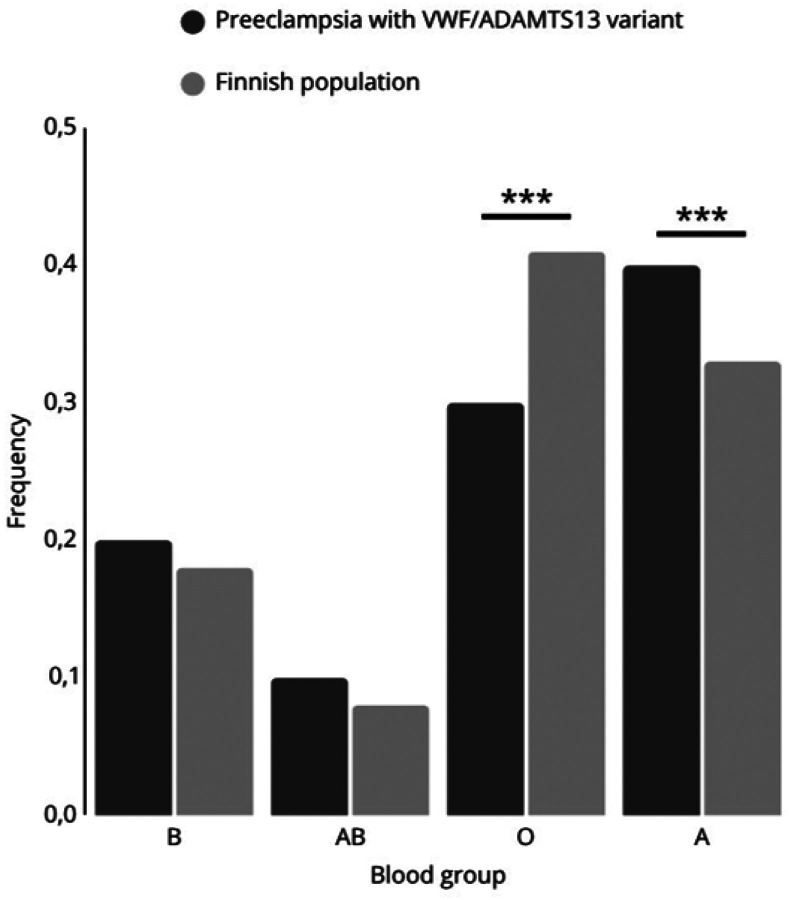 Figure 2
Figure 2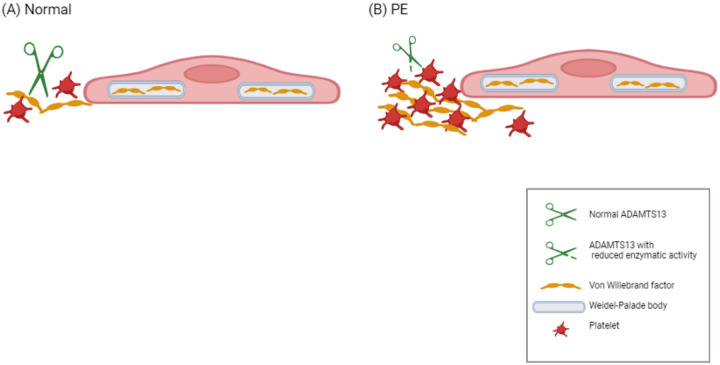 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and preeclampsia studies · Complement system in diseases · Hemoglobinopathies and Related Disorders
Introduction
Preeclampsia (PE) is a common pregnancy-specific vascular disorder with diverse clinical characteristics. It affects approximately 3% of pregnancies and accounts for over 50,000 maternal and 900,000 perinatal deaths annually^1^. No specific treatment, other than delivery, is available for PE. For prevention, low-dose aspirin administered from < 16 weeks of gestation has been suggested to reduce the risk of preterm PE (resulting in delivery before 37 wks of gestation) in women at high risk for PE, but its use remains controversial^2^. Despite common signs, proteinuria and hypertension, the etiology of PE could be heterogeneous, especially in a subset of cases.
There is a familial predisposition to PE and strong epidemiological evidence suggests that the risk for PE is inherited^3^. However, the individual variant effects of the candidate genes discovered thus far are modest. Finnish population presents an opportunity to study complex diseases, because the allele frequencies observed in the modern Finnish population result from several bottleneck events in the founder population which helps to identify relevant pathways for disease pathogenesis due to the enrichment of associating variants^4^.
The coagulation system is activated by changes in the vascular endothelium, and by platelet activation, adhesion, aggregation and interaction among leukocytes. In these processes, platelet interactions with von Willebrand factor (VWF) are an important contributor. Dysregulation of the platelet activity and coagulation system may result in thrombotic microangiopathies, including hemolytic anemia, and thrombocytopenia in women with PE^5^. No firm consensus regarding the role of platelets and coagulation biology in the development of PE has been reached^6–8^. Early results linking common variants such as FV Leiden and the prothrombin 3′ UTR variant to PE risk have not been replicated in larger studies^9^.
To investigate the role of the genetic burden of coagulation proteins in PE, we designed a targeted exome sequencing study to screen the exons and splicing sites of genes involved in blood coagulation and its regulation.
Results
In the 58 selected genes we discovered 107 annotated variants and 151 presumably benign variants (data not shown). Key results of this association analysis are shown in Table 2 (significant and borderline significant variants noted). The significantly associated variants in Table 2 are all listed as variant of unknown significance by the American College of Medical Genetics (ACMG) classification^10^. Overall, the most significant associations were available in the hemostasis axis, including VWF and its size-regulating ADAMTS13 enzyme. Also, two protective antithrombin variants were discovered.
The gene coding for von Willebrand Factor (VWF) wasassociated with PE by three likely or probable LoF variants with significant p-values (Figure 1A). Rs1800385 (p.Val1565Leu) in the middle of the VWF gene is a missense variant that increases the risk for PE (OR=1.72, 95% confidence interval (CI) 1.27–2.32, p-value=3.57E-4). The intronic variant rs34444862 located 8 base pairs downstream of exon 35, and the second missense variant rs34230288 (p.Ala2178Ser) increase the risk for PE (OR=2.30, 95%CI=1.19–4.35, p-value=0.01; OR=2.2, CI 1.11–4.17, p-value=0.017, respectively).
In ADAMTS13, the intronic variant rs36218903 increased the risk for PE (OR=3.06, CI 95%=1.42–6.53; p-value=0.002), while the splice region variant rs36219245 decreased risk (OR=0.57, 95% CI 0.40–0.80; p-value=8.62E-4), (Figure 1B). The missense variant rs41314453 (Ala732Val) in ADAMTS13 had a suggested increase in PE risk (OR=1.97, 95% CI=0.99–3.78; p-value=0.044).
We also found that in our cohorts rs5878 and rs5877 in SERPINC1 encoding for antithrombin (III), a critical plasma protease inhibitor and a member of the serpin superfamily, decreased the risk for PE (OR= 0.85 (95% CI=0.74 – 0.98), and 0.86 (95% CI=0.74–1), p-value=0.02 and 0.03, respectively).
Comparison of the frequency of blood groups between patients carrying VWF and/or ADAMTS13 variants in the Finnish population revealed that women affected by PE blood group A are significantly more prevalent (X^2^ = 16.227, p<0.0001; Figure 2). In contrast, blood group O was significantly underrepresented in the PE patients (X^2^ = 21.403, p<0.0001).
Discussion
Our results suggest that genetic variants in VWF and in its size and functional regulator ADAMTS13 associate with primary hemostasis abnormalities. Variants in genes coding for both proteins may predispose to PE. Women with blood group A are at particular risk of VWF-mediated PE, while mothers with blood group O have a lower incidence of PE.
These observations further support the proposed causative role of platelet dysregulation in a specific subgroup of PE. Importantly, we found associations within the VWF and ADAMTS13 axis, that cooperates to promote platelet-vascular wall interactions. A decrease in ADAMTS13 activity and an increase in VWF levels have also been previously associated with PE^11^, although the underlying and causative mechanisms in the VWF pathway have been under debate^12,13^. It is possible that VWF abnormalities are particularly associated with PE with severe features^14^. Common genetic variants within other coagulation genes are associated with PE^15^. Two of the discovered common PE-associating variants rs5878 and rs5877 in SERPINC1 that encode antithrombin are related reduced generation of thrombin and formation of fibrin. While we were able to confirm the reported association between Factor V Leiden (rs6025) and PE, the literature provides sparse insight into the potential associations we discovered in other F5 loci or variants discovered in F2, F7, and SERPINA5. Overall, the link between common coagulation variants, regulation of the coagulation system and an increased risk of preeclampsia^16,17^ was strongly corroborated by our data.
VWF is a plasma, platelet and endothelial glycoprotein that maintains hemostasis by generating multimers, which induce platelet aggregation and bind several proteins on activated endothelial cells in the vascular wall. Thereby, the multimers can lead to loss of vascular endothelial integrity^18^. This is particularly relevant in the placental vasculature due to its specific hemodynamic conditions. To prevent excessive platelet responses and coagulation, VWF oligomers emerging from endothelial cells or activated platelets are proteolytically cleaved by the ADAMTS13 enzyme^19,20^. ADAMTS13 cleaves VWF between tyrosine and methionine at position 842–843. Mutations in the ADAMTS13 gene or, more commonly, autoantibodies against the ADAMTS13 enzyme cause thrombotic thrombocytopenic purpura (TTP).
The variant rs34230288 results in the replacement of the alanine at position 2178 with a serine in VWF. This variant has been observed in a patient who was in cis heterozygous for two VWF mutations and suffering from a noncanonical type 2B von Willebrand disease characterized by low VWF activity^21^. Similarly, the variant rs1800385 results in the replacement of valine at position 1565 by leucine resulting in significantly elevated ADAMTS13 activity but available data is insufficient to ascertain it’s functional relevance^22^. Rs41314453 is the main genetic determinant of ADAMTS13 activity. It is important to note that it is in linkage disequilibrium with several intronic variants in ADAMTS13 and variants in the regulatory regions of neighbouring genes^23^. The total effect of rs41314453 is dependent on the sequence context, which may influence the extent and direction of its effect on gene expression^24^. It has been estimated that the variant reduces ADAMTS13 levels by approximately 40%^23,24^. Although this magnitude of a decrease does not reach levels that are considered significant in TTP (< 10%), it may be significant in the context of the strong triggers such as pregnancy. The product of the ADAMTS13 gene with the minor allele T of rs41314453 has up to 29% less VWF cleavage activity than the protein coded by the gene with the major allele^24^. Thereby, rs41314453 may increase the risk for platelet deposition by accumulation of ultralarge VWF multimers (Fig. 3). In TTP, the accumulation of platelet-super-adhesive ultralarge VWF multimers on vascular endothelium leads to the spontaneous formation of microthrombi. Pregnancy is also one of the well-known triggers to precipitate attacks of TTP^5^.
We recorded the blood groups of the women due to their role in association with VWF levels. Persons with blood group O have 30% lower VWF expression than the other blood groups, and blood group O has implications for platelet physiology^25^. Previously, blood groups A and more convincingly AB have been linked to a modestly increased risk of PE^26,27^. In addition, blood group A has been found to predispose to severe COVID-19, while blood group O is protective against infection and microthrombosis^28^. Concurrently, blood group O carries a 30% lower level of VWF, which may be highly elevated in COVID-19^29,30^. COVID-19 infection is also an independent risk factor for PE^33^. Our observed genetic variants of VWF, ADAMTS13 and non-O blood groups, likely contribute to the pathogenesis of PE. Furthermore, these findings may be helpful in the future to risk stratify patients and target novel therapies based on the specific analysis of VWF and ADAMTS13 biomarkers^31^
The findings of our study may explain aspects of the pathophysiology of PE and clinical observations related to the preventive use of aspirin. In PE, the placental intervillous blood flow is perturbed due to the lack of vasodilation in the spiral arteries, and local high shear forces prevail, promoting platelet-VWF interactions^32,33^. This also increases the risk of local red blood cell lysis and promotes the release of ADP and thromboxane A2, which are known to further activate platelets. ADP increases the expression and release of VWF on platelets^34^. Associated activation of the complement system results in the formation of C5a and of membrane attack complexes, which can further activate platelets and induce release of VWF from endothelial cell Weibel-Palade bodies^35–37^. Subsequent reduced ability of ADAMTS13 to cleave VWF multimers would thus promote formation of platelet aggregates, which have been shown to be resistant to ADAMTS13^38^. On the other hand, VWF has been shown to protect the endothelium from complement-mediated injury^39^. Aspirin has been shown to reduce expression of VWF on platelet surfaces^34^. Thereby it may partially compensate for the procoagulant effect of rs41314453 on ADAMTS13. Reduced platelet activity may improve blood flow in the intervillous space and reduce local ischemia and the severity of PE. TTP is associated with adverse pregnancy outcomes including PE^40^. Previously, a patient suffering from TTP due to a mutation in ADAMTS13 experienced a successful pregnancy under prophylactic treatment by aspirin^41^. More recently, novel drugs to influence the VWF-ADAMTS13 axis have emerged. Drugs like caplacizumab or recombinant ADAMTS13 could thus potentially be used in severe cases that are linked to high level of VWF multimerization and thrombosis^42^.
In TMA, activation of the coagulation cascade and complement systems often go hand in hand^43^. Similarly, pregnancy is an inflammatory and procoagulative state. In a blood proteomic study, the most different expression patterns between preeclamptic patients and controls were observed in complement and coagulation pathways and platelet function and VWF were also implicated^44^. Thereby patients with a predisposing complement and/or coagulation pathway variants may present with TMA-like PE^45^.
This study was limited by unavailability to study VWF and ADAMTS13 activity or their biomarkers. Furthermore, complete blood cell counts were not measured routinely thereby rendering the analysis of this data inconclusive. The effect of blood group for PE risk in carriers of VWF and ADAMTS13 variants requires further investigation in other well-described case-control cohorts representing varied populations.
In summary, our findings demonstrate a link between PE and two important and related hemostatic components VWF and ADAMTS13. Our results support the concept that in some cases, PE with severe features may present as a thrombotic microangiopathy^45^. The fact that PE-associated rs41314453 reduces ADAMTS13 level suggests that the ADAMTS13-VWF axis and regulated VWF size or multimerization are important in preventing PE. Our results may also relate to aspirin, which may show preventive properties against preeclampsia in high-risk individuals. However, in the future based on laboratory assessment of VWF and ADMTS13, novel medications, such as caplacizumab and recombinant ADAMTS13 should be evaluated in PE.
Methods
Patient cohorts
Two independent case-control cohorts, The Finnish Genetics of preeclampsia Consortium (FINNPEC) cohort and the national FINRISK study cohort were investigated. The study rational is described in detail in the supplementary data. In the final association analyses, we included genotypes of FINNPEC and FINRISK population cohorts, leading to a combined total of 615 cases and 2094 controls. For FINNPEC, all women provided a written informed consent, and the FINNPEC study protocol was approved by the coordinating Ethics Committee of the Hospital District of Helsinki and Uusimaa. (FINRISK license 8/2016)^46^. The patients and controls from the FINNPEC cohort are characterized in the Supplementary table S1. The National FINRISK Study description and ethical approvals are available online: https://www.thl.fi/en/web/thlfi-en/research-and-expertwork/population-studies/the-national-finrisk-study. This study was conducted in accordance with the Declaration of Helsinki.
Targeted Sequencing and Capture Enrichment
Libraries from genomic DNA were prepared in-house (Washington University School of Medicine)^47^. Enzymes were purchased from Enzymatics (Beverly, MA). Briefly, the ends of sheared genomic DNA fragments were repaired by treatment with T4 DNA Polymerase and T4 DNA Polynucleotide Kinase, which phosphorylates the 5’ hydroxyl. Next, an adenosine was added to the 3’ position at each end of the DNA fragment with Taq Polymerase. Illumina adapters with an overhanging “T” were ligated onto the DNA fragment followed by bead-based size selection to remove adapter-dimers and fragments below the desired size. A barcode consisting of a unique index sequence was added by PCR by targeting the two ligated universal adapters on each fragment end. Sequence capture hybridization and other laboratory methods are described in the Supplementary data. The studied genes and intronic loci of interest are listed in Table 1.
Fisher’s exact t-test was used as the primary test of association, and differences in frequencies of variants with p-value < 0.05 were considered significant. Significant and borderline significant variants are listed in Table 2. In addition to the statistical probability test, odds ratios (OR) with 95% confidence intervals (CI95) were calculated for all variants.
Comparison of the distribution of P values in benign (synonymous, intronic/intergenic; 151 observed variants) vs. annotated (missense, truncating, essential splice and splice region; 107 observed variants) variants indicate that the expected incidence of two annotated variants with p<0.001 is less than 0.01 in our data, compared with 0 observed variants with p<0.001. The lack of inflated P values indicates that confounders, such as stratification, are not causing false positives. Loss of function (LoF) analyses were done in silico for all genes with associating variants by the Loss of Function – tool of the Variant Effect Predictor (VEP) (https://github.com/ensembl-variation/VEP_plugins/blob/master/LoFtool.pm). In the LoF tool, the following annotations were calculated: LoF score < 0.2 indicates a probably damaging variant, LoF score 0.2–0.7 possibly damaging and LoF score < 0.7 a benign variant. 5/7 of the genes in Table 2 had scores < 0.2, suggesting a probable LoF.
Data were analyzed using PlinkSeq, Plink^48^ and R. Kaviar^49^. VEP Build 37 was used for additional annotations^50^.
Supplementary Files
This is a list of supplementary files associated with this preprint. Click to download.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van Lerberghe W., Manuel A., Matthews Z. & Cathy W. The World Health Report 2005 - Make Every Mother and Child Count. (2005).
- 2Rolnik D. L. Aspirin versus Placebo in Pregnancies at High Risk for Preterm Preeclampsia. New England Journal of Medicine (2017) doi:10.1056/nejmoa 1704559.28657417 · doi ↗ · pubmed ↗
- 3Skjaerven R. Recurrence of pre-eclampsia across generations: exploring fetal and maternal genetic components in a population based cohort. BMJ 331, 877 (2005).16169871 10.1136/bmj.38555.462685.8FPMC 1255793 · doi ↗ · pubmed ↗
- 4Lim E. T. Distribution and Medical Impact of Loss-of-Function Variants in the Finnish Founder Population. P Lo S Genet 10, e 1004494 (2014).25078778 10.1371/journal.pgen.1004494 PMC 4117444 · doi ↗ · pubmed ↗
- 5Mc Crae K. R. Thrombocytopenia in pregnancy. Hematology.American Society of Hematology.Education Program 2010, 397–402 (2010).21239825 10.1182/asheducation-2010.1.397 · doi ↗ · pubmed ↗
- 6Boij R. Biomarkers of coagulation, inflammation, and angiogenesis are independently associated with preeclampsia. Am J Reprod Immunol 68, 258–270 (2012).22626009 10.1111/j.1600-0897.2012.01158.x · doi ↗ · pubmed ↗
- 7Dehkordi M. A. e. R., Soleimani A., Haji-Gholami A., Vardanjani A. K. & Dehkordi S. A. e. R. Association of deficiency of coagulation factors (Prs, Prc, ATIII) and FVL positivity with preeclampsia and/or eclampsia in pregnant women. Int J Hematol Oncol Stem Cell Res (2014).PMC 434529925774262 · pubmed ↗
- 8Han L. Blood coagulation parameters and platelet indices: Changes in normal and preeclamptic pregnancies and predictive values for preeclampsia. P Lo S One (2014) doi:10.1371/journal.pone.0114488.PMC 425214725464515 · doi ↗ · pubmed ↗