Renal cell carcinoma with cavoatrial ventricular involvement
Laurna McGovern, Roman Roy, Antonio Rullan

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
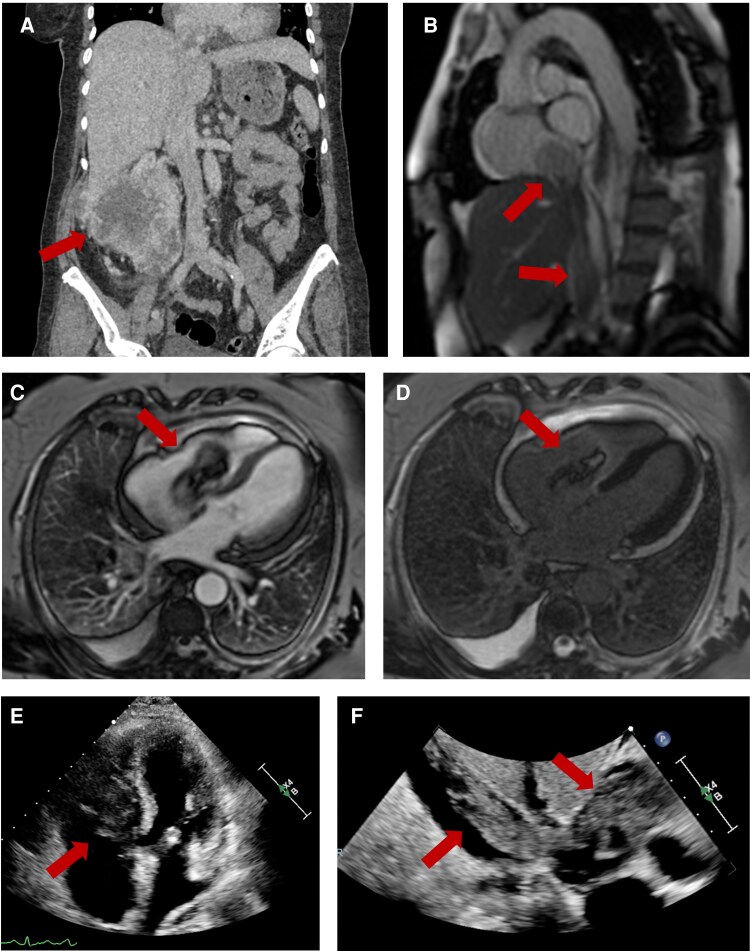 Figure 1
Figure 1- —National Institute for Health
- —Care Research Integrated Academic Training Programme
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal cell carcinoma treatment · Renal and Vascular Pathologies
A 71-year-old woman with no significant past medical history presented to the emergency department with a 1-month history of worsening abdominal pain and bilateral lower-limb oedema. Computed tomography of chest, abdomen, and pelvis showed a large right renal mass (12 cm × 10 cm; Panel A), multiple lung metastasis, mediastinal, and right hilar adenopathy. Tumour thrombus was seen within the inferior vena cava (IVC) with extension to the right atrium and ventricle (Panels E and F). Cardiac magnetic resonance imaging (MRI) demonstrated a large, mobile mass (53 mm × 25 mm) extending along the whole IVC into the right atrium across the tricuspid valve into the right ventricle (Panels B and C; Supplementary material online, Video S1). There was no contrast uptake on first pass perfusion with heterogeneous late gadolinium enhancement in the periphery and central avascular core (Panel D). The patient was asymptomatic at diagnosis, with mild–moderate tricuspid regurgitation and preserved biventricular systolic function. She was started on anticoagulation with heparin.
Right renal biopsy confirmed Grade 4 clear cell renal cell carcinoma (RCC; AE1/AE3, CD10 and PAX-8 positive) with areas of necrosis and sarcomatoid differentiation. Following cardio-oncology multidisciplinary team discussion, treatment with ipilimumab and nivolumab was commenced. Unfortunately, the patient experienced disease progression to first-line treatment, developed significant right-sided cardiac failure, and died 3 months after diagnosis.
Intravascular invasion of the IVC complicates 5%–15% of RCC cases with 1% involving extension to the right atrium. Right ventricular involvement is even less frequent, with case reports of right ventricular outflow tract obstruction published in the literature. The median overall survival for patients with metastatic RCC after first-line treatment is 4 years. Although echocardiography is commonly the first line in assessing cardiac masses, cardiac MRI is particularly valuable in characterizing their aetiology.
(A) Computed tomography: coronal view of the primary renal cell carcinoma. (B) Cardiac magnetic resonance: Sagittal view of tumour/thrombus in inferior vena cava extending to right atrium. (C) Cardiac magnetic resonance: four-chamber early gadolinium enhanced image showing a large, mobile mass (53 mm × 25 mm) in the right atrium extending across the tricuspid valve into the right ventricle. (D) Cardiac magnetic resonance: four-chamber late gadolinium image demonstrating heterogeneous late gadolinium enhancement in the periphery and central avascular core. (E) Echocardiogram: apical four-chamber view of tumour thrombus in right ventricle. (F) Echocardiogram: subcostal view of tumour thrombus extending from inferior vena cava to right atrium.
Supplementary Material
ytaf305_Supplementary_Data