A Case Series on the Effectiveness of Abdominal Belts for Postural Blood Pressure Disorders in Parkinson’s Disease
Katsunori Yokoi, Keisuke Suzuki, Akiko Yamaoka, Masahisa Katsuno, Yutaka Arahata

TL;DR
This study explores how abdominal belts affect blood pressure in Parkinson’s disease patients with orthostatic hypotension, finding some improvement in daytime BP stability.
Contribution
The study provides new clinical insights into using abdominal belts as a non-pharmacological intervention for postural blood pressure disorders in Parkinson’s disease.
Findings
Three out of four patients showed improved blood pressure stability during daytime with abdominal belt use.
One patient experienced significant increases in systolic and diastolic blood pressure.
Nocturnal blood pressure remained unchanged despite belt use.
Abstract
Orthostatic hypotension (OH) is a common non-motor complication of Parkinson’s disease (PD), significantly affecting the quality of life and increasing fall risk. While pharmacological treatments are available, their efficacy is often limited. Abdominal belts have been proposed as a non-pharmacological intervention, but their effects on blood pressure (BP) fluctuations remain unclear. In this case series, we examined four patients with PD and OH, all of whom underwent 24-hour ambulatory BP monitoring (ABPM) before and after using an abdominal belt. The belt was applied with a pressure of 20 ± 2 mmHg and worn during waking hours. The mean systolic BP (SBP) and diastolic BP (DBP) during daytime and nighttime were compared using the Mann-Whitney U test. BP variability was assessed. Three patients demonstrated improved BP stability with abdominal belt use, particularly in reducing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
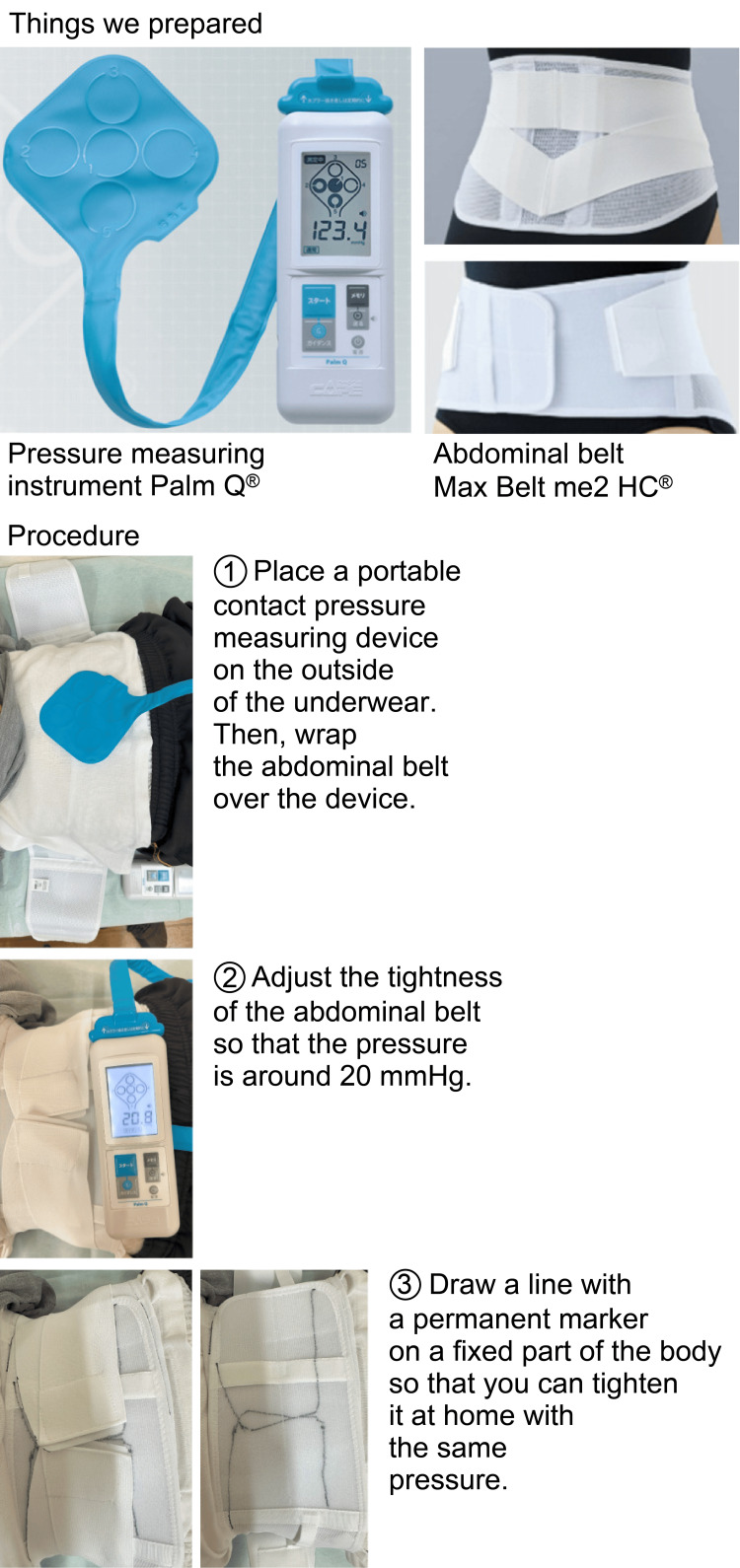 Figure 1
Figure 1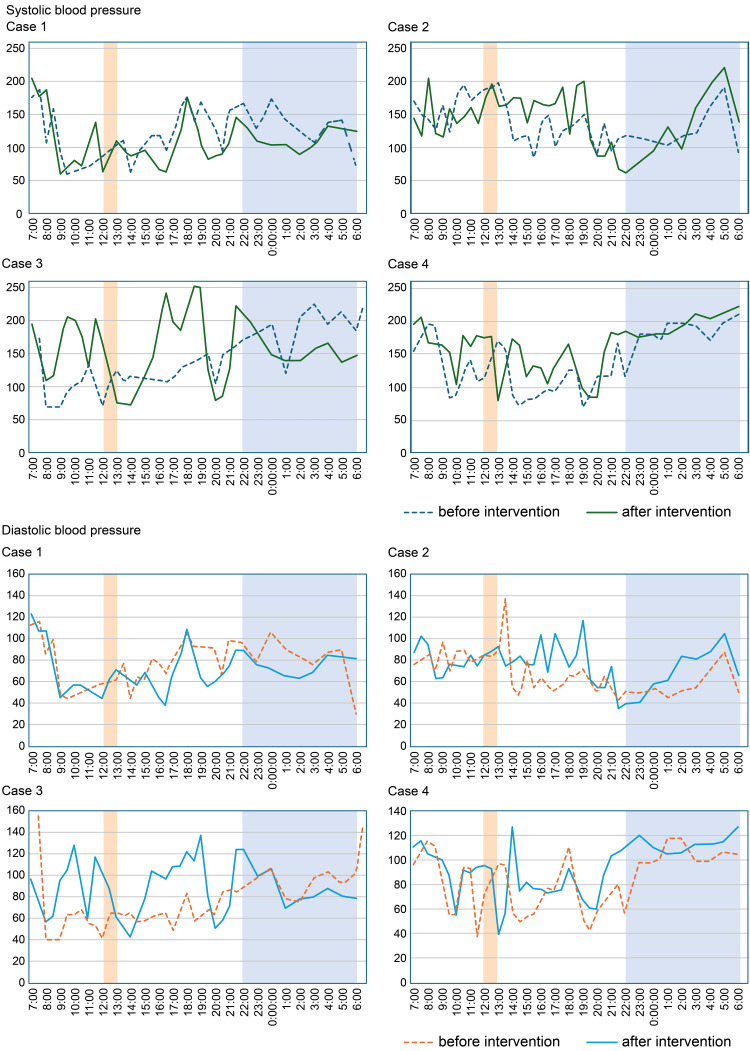 Figure 2
Figure 2| Age | Sex | Years from onset | Parkinson’s disease phenotype | Levodopa equivalent daily dose (LEDD) | Specific dopaminergic drugs (/day) | Pressor agents (/day) | Anti-hypertensive drugs (/day) | |
| Case 1 | 78 | Male | 5 | Postural instability and gait difficulty type | 675 mg/day | Levodopa/benserazide 600 mg, zonisamide 25 mg, safinamide 50 mg | Droxidopa 600 mg, midodrine 4 mg | Antihypertensive discontinued at onset |
| Case 2 | 81 | Male | 7 | Akinetic-rigid type | 569 mg/day | Levodopa/carbidopa/entacapone 300 mg, levodopa/benserazide 50 mg, zonisamide 50 mg, safinamide 50 mg, istradefylline 20 mg | Midodrine 6 mg | Arotinolol 10 mg |
| Case 3 | 83 | Male | 4 | Postural instability and gait difficulty type | 450 mg/day | Levodopa/benserazide 450 mg | Droxidopa 600 mg, midodrine 8 mg, fludrocortisone 0.05 mg | No history of antihypertensive medication use |
| Case 4 | 74 | Female | 9 | Postural instability and gait difficulty type | 766 mg/day | Levodopa plus benserazide 350 mg, rasagiline 1 mg, opicapone 25 mg, amantadine 200 mg | Droxidopa 600 mg | No history of antihypertensive medication use |
| Pre-lunch Maximum SBP | Post-lunch Minimum SBP | ΔSBP or DBP (Drop) | |||
| Case 1 | Before | Systolic | 106 | 63 | 43 |
| Diastolic | 62 | 45 | 17 | ||
| After | Systolic | 111 | 88 | 23 | |
| Diastolic | 71 | 57 | 14 | ||
| Case 2 | Before | Systolic | 200 | 109 | 91 |
| Diastolic | 89 | 53 | 36 | ||
| After | Systolic | 197 | 163 | 34 | |
| Diastolic | 88 | 75 | 13 | ||
| Case 3 | Before | Systolic | 124 | 107 | 17 |
| Diastolic | 65 | 62 | 3 | ||
| After | Systolic | 128 | 73 | 55 | |
| Diastolic | 87 | 43 | 44 | ||
| Case 4 | Before | Systolic | 172 | 73 | 99 |
| Diastolic | 97 | 50 | 47 | ||
| After | Systolic | 177 | 80 | 97 | |
| Diastolic | 93 | 39 | 54 |
| Before | After | U-value | Z-value | p-value | Effect size, r | |||||||
| Blood pressure | SD | CV | Blood pressure | SD | CV | |||||||
| Case 1 | During activities | Systolic | 126.08 ± 7.48 | 36.64 | 0.29 | 110.37 ± 7.79 | 39.71 | 0.36 | 432.5 | 1.740 | 0.083 | 0.241 |
| Diastolic | 80.4 ± 3.92 | 20.04 | 0.25 | 70.26 ± 3.19 | 21.59 | 0.31 | 436.5 | 1.813 | 0.071 | 0.251 | ||
| Bedtime | Systolic | 128.86 ± 7.77 | 29.75 | 0.23 | 109.86 ± 6.25 | 13.2 | 0.12 | 38 | 1.725 | 0.097 | 0.461 | |
| Diastolic | 79.86 ± 8.92 | 21.85 | 0.27 | 73.00 ± 3.08 | 7.54 | 0.1 | 37.5 | 1.661 | 0.109 | 0.444 | ||
| Case 2 | During activities | Systolic | 141.14 ± 6.04 | 31.94 | 0.23 | 146.39 ± 6.93 | 37.94 | 0.26 | 399 | -0.747 | 0.459 | -0.096 |
| Diastolic | 71.07 ± 4.02 | 19.5 | 0.27 | 77.81 ± 3.52 | 17.82 | 0.23 | 338.5 | -1.642 | 0.102 | -0.212 | ||
| Bedtime | Systolic | 127.25 ± 6.32 | 30.9 | 0.24 | 140.50 ± 14.80 | 46.84 | 0.33 | 28 | -0.420 | 0.721 | -0.105 | |
| Diastolic | 58.00 ± 4.98 | 13.17 | 0.23 | 73.13 ± 7.15 | 18.92 | 0.26 | 16 | -1.680 | 0.105 | -0.420 | ||
| Case 3 | During activities | Systolic | 117.85 ± 5.92 | 29.59 | 0.25 | 162.74 ± 10.80 | 55.06 | 0.34 | 178 | -3.078 | 0.002 | -0.423 |
| Diastolic | 66.35 ± 3.36 | 22.73 | 0.34 | 91.19 ± 5.24 | 26.33 | 0.29 | 169.5 | -3.229 | 0.001 | -0.444 | ||
| Bedtime | Systolic | 190.13 ± 10.23 | 29.5 | 0.16 | 158.56 ± 11.44 | 14.39 | 0.09 | 55.5 | 2.468 | 0.015 | 0.617 | |
| Diastolic | 94.13 ± 4.16 | 11.02 | 0.12 | 85.00 ± 4.28 | 11.34 | 0.13 | 42.5 | 1.103 | 0.293 | 0.276 | ||
| Case 4 | During activities | Systolic | 120.07 ± 6.91 | 35.22 | 0.29 | 148.79 ± 6.68 | 35.36 | 0.24 | 221 | -2.796 | 0.005 | -0.374 |
| Diastolic | 75.00 ± 3.99 | 21.87 | 0.29 | 85.66 ± 3.92 | 20.14 | 0.24 | 286 | -1.730 | 0.085 | -0.231 | ||
| Bedtime | Systolic | 189.56 ± 9.36 | 12.96 | 0.07 | 197.86 ± 4.02 | 16.51 | 0.08 | 24.5 | -1.107 | 0.288 | -0.268 | |
| Diastolic | 104.67 ± 2.54 | 7.2 | 0.07 | 113.63 ± 2.56 | 6.78 | 0.06 | 14.5 | -2.069 | 0.043 | -0.502 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParkinson's Disease Mechanisms and Treatments · Restless Legs Syndrome Research · Cardiovascular Syncope and Autonomic Disorders
Introduction
Parkinson’s disease (PD) is the second most common neurodegenerative disorder after Alzheimer’s disease, with prevalence increasing with age. It is primarily caused by the progressive degeneration of dopaminergic neurons in the substantia nigra, leading to both motor and non-motor symptoms. Epidemiological studies report a PD prevalence of 3.1% in individuals aged >75 years and 4.5% in those aged >85 years [1,2]. Among the non-motor symptoms, orthostatic hypotension (OH) is a frequent and clinically significant complication that severely impacts daily functioning.
OH is clinically defined as a sustained reduction of at least 20 mmHg in systolic blood pressure (SBP) or 10 mmHg in diastolic blood pressure (DBP) within three minutes of standing up or head-up tilt to ≥60 degrees [3]. In PD, OH is primarily attributed to autonomic dysfunction caused by degeneration of the peripheral sympathetic nervous system and central autonomic pathways [4]. This autonomic impairment leads to inadequate vasoconstriction upon standing, resulting in insufficient venous return, decreased cardiac output, and subsequent BP drops. OH not only contributes to physical disability and reduced quality of life but also increases the risk of falls by 2.6 times, potentially affecting prognosis [4,5]. Furthermore, OH in PD has been associated with cognitive decline and increased mortality risk, underscoring the need for effective management strategies [6,7].
The current treatment options for OH in PD primarily include pharmacological interventions, such as midodrine, an alpha1-adrenergic receptor agonist; droxidopa, a precursor of norepinephrine; and fludrocortisone acetate. However, these treatments often have limited efficacy owing to side effects such as supine hypertension, short duration of action requiring frequent dosing, and variability in individual responses, leading to inconsistent therapeutic outcomes [8,9]. Consequently, non-pharmacological approaches, including lifestyle modifications and mechanical interventions, such as elastic stockings and abdominal belts, have been explored as complementary strategies for managing OH [10]. Abdominal binders can help mitigate OH by increasing venous return and stabilizing blood pressure (BP) [11]. Despite their theoretical benefits on orthostatic tolerance, evidence supporting their effectiveness remains limited. Current clinical guidelines for PD do not universally recommend their use, reflecting a lack of consensus on their efficacy and the need for further research [3].
BP variability (BPV) is a clinically significant factor in patients with PD and OH, as it has been linked to an increased risk of cardiovascular events, cognitive decline, and disease progression [12,13]. Monitoring BPV is essential for assessing the effectiveness of OH interventions, and 24-hour ambulatory BP monitoring (ABPM) has been identified as a useful tool for evaluating these fluctuations [11]. However, comprehensive studies on the impact of abdominal binders on BPV in patients with PD remain limited [3].
To address this gap, we conducted a case series of four patients with PD and OH who underwent 24-hour ABPM before and after the application of an abdominal belt. We aimed to provide insights into the effectiveness of abdominal belts in stabilizing BP and reducing variability throughout the day. Ultimately, our findings may inform clinical guidelines and improve treatment strategies for OH in PD, offering a more personalized approach to non-pharmacological management [11,13].
Case presentation
Study design and ethical approval
We present a case series of four patients with OH associated with PD who used abdominal belts. Changes in BP were assessed using a 24-hour BP monitor by comparing measurements taken with and without the abdominal belt for each patient. This study was approved by the Ethics Committee of the National Center for Geriatrics and Gerontology (NCGG) (approval number: 1450-3). Since the information was extracted in a manner that prevents individual identification through the opt-out process, individual informed consent was not required. However, for the four patients included in this study, verbal and written consent was obtained for the use of lidocaine injections and muscle hardness gauges before administration. Verbal informed consent was obtained for the use of patient information in research.
Inclusion criteria
To be included in this study, patients needed a diagnosis of PD, a diagnosis of OH, and daily life-impairing BP fluctuations. Moreover, they had to be willing to undergo 24-hour BP monitoring and use an abdominal belt. OH was defined as a decrease in systolic BP (SBP) of ≥20 mmHg and a decrease in diastolic BP (DBP) of ≥10 mmHg within three minutes of transitioning from a supine to a standing position [14]. This threshold (≥20 mmHg in SBP) was also used as the criterion for interpreting clinical changes in response to the intervention.
Exclusion criteria
Patients were excluded if they had OH due to a condition other than PD, cognitive decline preventing the ability to follow instructions, inability to wear an abdominal belt for any reason, or were unwilling to wear a 24-hour BP monitor.
Procedure
First, baseline BP was measured using a 24-hour BP monitor before abdominal belt use. Then, patients were fitted with the abdominal belt and provided with instructions on its use (Figure 1). On the following day, patients wore the abdominal belt, and BP was measured again using the 24-hour BP monitor. Patients were instructed to wear the abdominal belt from 07:00 to 22:00 during daytime activities. Although actual adherence was based on patient self-report, all participants indicated general compliance with this schedule. Finally, changes in BP before and after using the abdominal belt were compared.
Protocol for using the abdominal beltPermission to use the product names and images of Palm Q® (CAPE Co., Ltd.) and Max Belt me2 HC® (Nippon Sigmax Co., Ltd.) was obtained from the respective manufacturers on April 24, 2025.
The abdominal belt was applied to exert an abdominal wall pressure of 20 ± 2 mmHg [15]. Markings were made to ensure consistent tightening pressure. The pressure measurement device used was the PalmQ® (CAPE Co., Ltd., Yokosuka, Kanagawa, Japan), and the abdominal belt was the Max Belt me2HC® (Sigmax Co., Ltd., Tokyo, Japan).
BP was continuously monitored while wearing the abdominal belt, including during sleep. All four patients were monitored for 24 hours on the day following their initial use of the abdominal belt. One patient (Case 1) refused to wear the abdominal belt during 24-h monitoring; hence, measurements were taken without it. This case is included as an exception for comparison purposes.
For all patients, medication was not altered for at least one month prior to the use of the abdominal belt and remained unchanged until 24-hour BP monitoring was completed to accurately assess the device’s effectiveness.
BP measurements were categorized into two periods: daytime (07:00-22:00, excluding bedtime) and nighttime (23:00-06:00, during sleep).
To evaluate the impact of abdominal band application on postprandial blood pressure regulation, we compared the maximum systolic and diastolic blood pressure during the pre-lunch period (12:00-13:00) with the minimum values during the post-lunch period (13:00-14:00), both before and after the intervention, across all four cases.
BP values with and without the abdominal belt were compared. Changes in BP for each patient were analyzed using the Mann-Whitney U test. Additionally, standard deviation and coefficient of variation were calculated and evaluated. All statistical analyses were conducted using EZR, a software package for R that enhances standard R commands by incorporating statistical functions commonly used in biostatistics [16].
Case 1
Background
A 78-year-old man initially presented with OH and was subsequently diagnosed with PD. Despite adjustments in his regimen, including L-Dopa, midodrine (8 mg), droxidopa (600 mg), and fludrocortisone (0.05 mg), the patient continued to experience frequent episodes of loss of consciousness and difficulty standing (Table 1, Case 1).
Intervention
The patient was advised to use an abdominal belt; however, he discontinued its use due to difficulties managing urination while wearing it. Although the patient did not report discomfort, pressure, or breathing difficulties while wearing the belt, he found it challenging to lower his underwear, leading to discontinuation the following day.
BP Changes
Twenty-four-hour BP monitoring without the abdominal belt revealed minimal BP changes, with no significant differences observed between daytime and nighttime values (Figure 2, Case 1, Table 1). The change in blood pressure before and after lunch was modest, with a systolic blood pressure (SBP) drop of 23 mmHg before the intervention and 27 mmHg after. Diastolic blood pressure (DBP) changes were also small (5 mmHg before, 9 mmHg after). No clear trend was observed in response to the intervention (Table 2).
Changes in 24-hour blood pressure before and after using the abdominal beltColored areas indicate the periods when the abdominal belt is removed and when the patient sleeps at night.
Case-Specific Discussion
This case highlights that practical issues, such as urination difficulties, can limit the sustained use of abdominal belts for OH management in patients with PD, even in the absence of discomfort.
Case 2
Background
An 81-year-old man was diagnosed with PD and dementia. The disease initially manifested with left-sided muscle stiffness, followed by cognitive decline, hallucinations, daytime somnolence, and hypotension. Despite treatment with L-Dopa and midodrine (6 mg), hypotension and episodes of loss of consciousness persisted (Table 1, Case 2).
Intervention
The use of the abdominal belt led to an improvement in daytime consciousness. The patient reported no discomfort, pressure, or breathing difficulties, and the belt was well tolerated.
BP Changes
Although statistically significant BP changes were not observed, there was a tendency for both SBP and DBP to increase during daytime periods with belt use. BP fluctuations persisted throughout monitoring (Figure 2, Case 2, Table 1). The change in blood pressure before and after lunch was pronounced, with a pre-intervention SBP drop of 91 mmHg and DBP drop of 25 mmHg, indicating clear postprandial hypotension (PPH). These drops were substantially reduced after the intervention (ΔSBP = 34 mmHg, ΔDBP = 5 mmHg), suggesting a notable stabilizing effect of the abdominal band (Table 2).
Case-Specific Discussion
Despite ongoing BP variability, the subjective improvement in daytime consciousness suggests that abdominal belt use may offer clinical benefits beyond simple BP elevation.
Case 3
Background
An 83-year-old man diagnosed with PD developed Parkinsonian symptoms four years earlier and was recently diagnosed with OH and daytime somnolence. His treatment included L-Dopa, midodrine (4 mg), and droxidopa (600 mg), but he frequently lost consciousness during meals (Table 1, Case 3).
Intervention
An abdominal belt was introduced, reducing but not completely eliminating episodes of loss of consciousness. While the patient reported no discomfort or breathing difficulties, the time required to apply the belt limited its use to times when he left his room.
BP Changes
Daytime SBP and DBP significantly increased during belt use. Nighttime SBP significantly decreased after the belt was removed before bedtime (Figure 2, Case 3; Table 1). The change in blood pressure before and after lunch was mild, with no difference in SBP drop between the pre- and post-intervention periods (14 mmHg). DBP changes were also small (10 mmHg before, 6 mmHg after), and no clear intervention effect was observed (Table 2).
Case-Specific Discussion
This case demonstrates that abdominal belt use can effectively stabilize daytime BP and reduce orthostatic symptoms, although practical barriers to frequent use remain.
Case 4
Background
A 74-year-old woman with a nine-year history of PD developed a shuffling gait and later OH secondary to BP fluctuations. Despite treatment with L-Dopa and droxidopa (600 mg), she continued to experience severe dizziness upon standing (Table 1, Case 4).
Intervention
Introduction of an abdominal belt improved symptoms. The patient tolerated the belt well, reporting no discomfort, pressure, or breathing difficulties.
BP Changes
Daytime SBP increased during belt use, and nighttime DBP tended to decrease after belt removal. Although no statistically significant differences were observed, BP values appeared more stable during daytime periods (Figure 2, Case 4; Table 3). The change in blood pressure before and after lunch was inconsistent. SBP dropped by 34 mmHg before the intervention, but the drop increased to 43 mmHg after. DBP also showed a greater decrease post-intervention (from 20 mmHg to 25 mmHg), suggesting no benefit from the abdominal band (Table 2).
Case-Specific Discussion
This case suggests that consistent use of an abdominal belt can alleviate OH symptoms without discomfort, particularly in patients who are able to tolerate continuous use.
Discussion
OH is a well-recognized non-motor feature of PD, known to impair quality of life and increase the risks of falls, cognitive dysfunction, and mortality.
The results of this study suggest that in Case 1, where the abdominal belt was not used, there was minimal improvement in symptoms. Although some changes were observed in the coefficient of variation, there was little change in the average BP or daily BP fluctuations over time. Although some degree of blood pressure fluctuation was noted, the overall pattern remained similar before and after the intervention. This case may reflect a relatively stable postprandial hemodynamic response, with limited susceptibility to PPH or limited responsiveness to the abdominal band.
In Case 2, the post-midday BP drop was attenuated, which corresponded with reported symptom improvement. However, there was minimal change in the coefficient of variation or average BP. Notably, this patient was underweight, which may be a distinguishing factor from the others. This case demonstrated the most prominent PPH and a substantial reduction in post-lunch BP drop following the intervention. The abdominal band appeared to be highly effective, suggesting that patients with strong autonomic responses or higher vulnerability may particularly benefit from this intervention.
In Case 3, BP tended to increase significantly with the use of the abdominal belt. Both upper and lower ranges increased, and the mean values of SBP and DBP during the day showed a significant increase. However, there was no significant change in the coefficient of variation. Overall BP variability was minimal, and no apparent effect of the intervention was noted. The PPH itself was mild, potentially limiting the detectability of any treatment effect.
In Case 4, SBP increased overall during the day when the abdominal belt was used, with a significant increase in mean values. Similar to Case 3, there was no significant change in the coefficient of variation. A paradoxical increase in BP drop was observed after the intervention. This may be attributable to intrinsic factors such as autonomic dysfunction, posture-related changes, or activity levels. Additional supportive strategies may be necessary for such cases.
Our analysis of pre- and postprandial blood pressure revealed a substantial reduction in ΔSBP and ΔDBP in Case 2 after abdominal belt use, indicating a possible mitigating effect on PPH. However, only two of the four cases demonstrated statistically significant improvements in daytime BP, highlighting the need to distinguish statistical significance from clinical relevance when interpreting these findings. Although this trend was not observed uniformly across all cases, the data suggest that abdominal compression may benefit selected patients with pronounced PPH patterns. This finding is clinically relevant given the high prevalence and morbidity associated with PPH in PD.
When examining these cases collectively, the findings suggest that the use of an abdominal belt in patients with PD and OH may help alleviate symptoms by increasing daytime BP. This aligns with the results of previous studies showing that external compression garments can relieve orthostatic symptoms by enhancing venous return and increasing central blood volume [15].
Our study also highlights the diurnal BP fluctuations in patients with PD. In clinical practice, patients often report experiencing daytime consciousness disturbances, and our findings specifically confirm that post-lunch BP decreases are particularly significant. Although the abdominal belt was effective in preventing severe hypotensive episodes, it did not completely eliminate postprandial hypotension. This is consistent with the results of previous studies showing that postprandial hypotension is less responsive to conventional treatments and may require a multifaceted approach, including dietary modifications, pharmacological interventions, and physical countermeasures [17,18].
We suggest that while the use of an abdominal belt may contribute to an increase in BP, it is unlikely to suppress fluctuations entirely. Variations in the extent and pattern of BP changes were observed among patients. Potential contributing factors to these differences include disease progression, severity of autonomic dysfunction, and body composition. Autonomic impairment in PD plays a critical role in BP dysregulation, underscoring the need for targeted interventions [14]. The importance of autonomic dysfunction in BP variability across neurodegenerative diseases is well-documented [3,8].
The use of abdominal belts was found to have a measurable effect in improving symptoms of OH. However, recent studies have also emphasized the impact of BP stabilization on non-motor symptoms, such as fatigue and cognitive function in PD. Maintaining a stable BP may contribute to improved cognitive function and reduced fatigue [19]. Additionally, recent research has indicated a potential link between effective OH management and overall quality of life in patients with PD [20].
This series has some limitations. First, its small sample size restricts the generalizability of the findings. Future research should focus on larger patient populations to validate these results. We also included only one control case, and the exclusion of confounding factors and potential placebo effects was not sufficient to determine the extent of improvement attributed solely to the abdominal belts. Indeed, the potential contribution of placebo effects is important considering the subjective nature of several reported outcomes. Additionally, this study only assessed short-term effects; further research is needed to evaluate long-term outcomes and patient adherence to abdominal belt use. Second, there is a lack of objective monitoring of belt usage in the reported cases. Although patients were instructed to wear the belt from 07:00 to 22:00, adherence was self-reported and may be subject to recall or reporting bias. Future studies incorporating prolonged ABPM could provide deeper insights into the sustained benefits of abdominal compression therapy. Third, as this was a case series of patients selected from a single institution, selection bias may have influenced the outcomes. Further research with larger, more diverse populations is needed to validate these findings and establish clearer patient selection criteria.
Despite these limitations, our study underscores the potential role of abdominal belts as an adjunct treatment for OH in PD. Given that current clinical guidelines do not explicitly recommend abdominal belts, our findings suggest that incorporating them into standard treatment strategies may be beneficial [17,18,20]. Future studies should incorporate validated symptom scales to assess clinical benefit, quantify actual device compliance, and define thresholds for clinically meaningful BP changes. In addition, effect size reporting and long-term follow-up data will be critical for evaluating therapeutic sustainability.
Conclusions
This study indicates that the use of an abdominal belt in patients with PD and OH may help alleviate symptoms related to daytime hypotension by increasing BP. However, while the abdominal belt was found to contribute to increasing BP levels, it had limited impact on reducing fluctuations. Overall, these results could be a promising indication of the efficacy of non-pharmacological management methods in such cases.
Nevertheless, these findings should be considered preliminary, as they are based on a small case series without a control group. Furthermore, this symptomatic benefit was derived from patients’ self-reports, and no validated symptom assessment tools were employed in this study. Further research is required to develop standardized guidelines for the integration of abdominal belts into the treatment of OH in PD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of Parkinson’s disease Lancet Neurol de Lau L Breteler M 525535520061671392410.1016/S 1474-4422(06)70471-9 · doi ↗ · pubmed ↗
- 2Slowing of neurodegeneration in Parkinson’s disease and Huntington’s disease: future therapeutic perspectives Lancet Schapira AHV Olanow CW Greenamyre JT Bezard E 54555538420142495467610.1016/S 0140-6736(14)61010-2 · doi ↗ · pubmed ↗
- 3Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome Auton Neurosci Freeman R Wieling W Axelrod FB 464816120112139307010.1016/j.autneu.2011.02.004 · doi ↗ · pubmed ↗
- 4Orthostatic hypotension as an early finding in Parkinson's disease Clin Auton Res Goldstein DS 46541620061647749510.1007/s 10286-006-0317-8 · doi ↗ · pubmed ↗
- 5Prevalence of orthostatic hypotension in Parkinson's disease: a systematic review and meta-analysis Parkinsonism Relat Disord Velseboer DC de Haan RJ Wieling W Goldstein DS de Bie RM 7247291720112157157010.1016/j.parkreldis.2011.04.016PMC 5199613 · doi ↗ · pubmed ↗
- 6Autonomic dysfunction in Parkinson disease Handb Clin Neurol Kaufmann H Goldstein DS 25927811720132409513110.1016/B 978-0-444-53491-0.00021-3 · doi ↗ · pubmed ↗
- 7Treatment of autonomic dysfunction in Parkinson disease and other synucleinopathies Mov Disord Palma JA Kaufmann H 3723903320182950845510.1002/mds.27344 PMC 5844369 · doi ↗ · pubmed ↗
- 8Neurogenic orthostatic hypotension: a pathophysiological approach Circulation Goldstein DS Sharabi Y 13914611920091912467310.1161/CIRCULATIONAHA.108.805887 PMC 4182314 · doi ↗ · pubmed ↗