Impact of response to electrical cardioversion before catheter ablation for persistent atrial fibrillation: a propensity score-matched analysis
Márton Boga, Zoltán Salló, Gábor Orbán, Ferenc Komlósi, Anna Padisák, Patrik Tóth, Péter Perge, Vivien Klaudia Nagy, Edit Tanai, István Osztheimer, Béla Merkely, László Gellér, Nándor Szegedi

TL;DR
This study shows that patients with persistent atrial fibrillation who maintain a normal heart rhythm after electrical cardioversion before ablation have better long-term outcomes.
Contribution
The study introduces pre-procedural electrical cardioversion response as a novel predictor of ablation success in persistent atrial fibrillation.
Findings
ECV-AF group had significantly lower freedom from atrial tachyarrhythmia at 36 months compared to ECV-SR group.
Persistent AF recurrence was more common in the ECV-AF group, while paroxysmal AF was more common in the ECV-SR group.
ECV response predicted better outcomes even after adjusting for multiple variables and across subgroups like PVI-only procedures.
Abstract
We hypothesize that sinus rhythm (SR) maintenance in persistent atrial fibrillation (AF) patients taking anti-arrhythmic drugs (AADs) after pre-procedural electrical cardioversion (ECV) could predict outcomes after catheter ablation procedures. 219 persistent AF patients on AADs underwent ECV 1–6 months before ablation. Patients were categorized into two groups according to their response to ECV: patients in whom SR was restored and maintained until the ablation procedure (ECV-SR group), and patients with AF recurrence before the procedure (ECV-AF group). Then, 1:1 propensity score matching was used to create study groups (94–94 patients). The efficacy outcomes of the present study were freedom from atrial tachyarrhythmia on/off AADs following a single ablation procedure and recurrence of persistent AF. The median follow-up duration was 42 (20–73) months. Freedom from atrial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
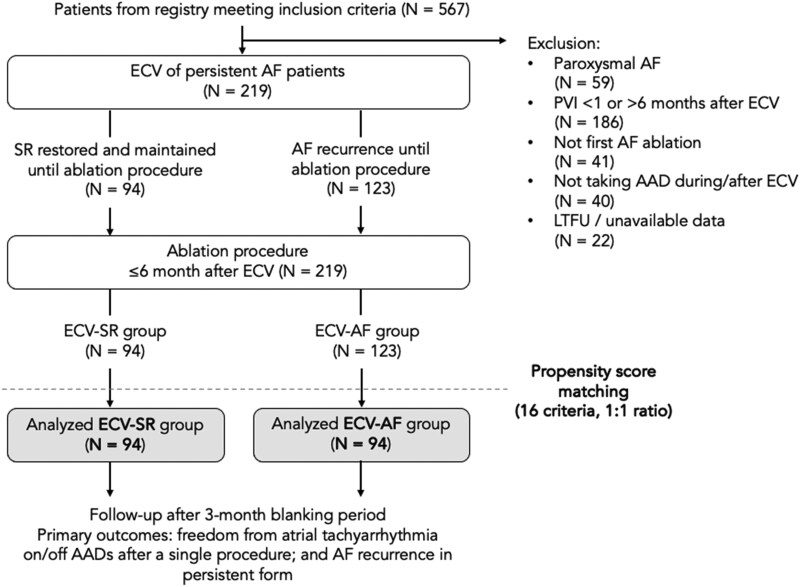 Figure 1
Figure 1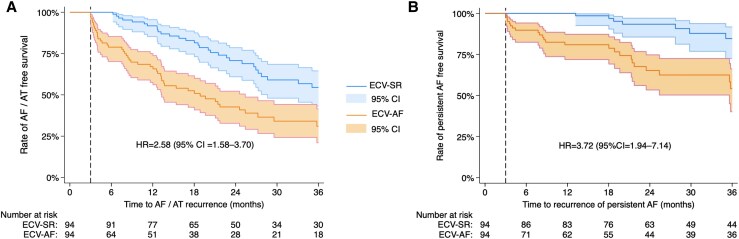 Figure 2
Figure 2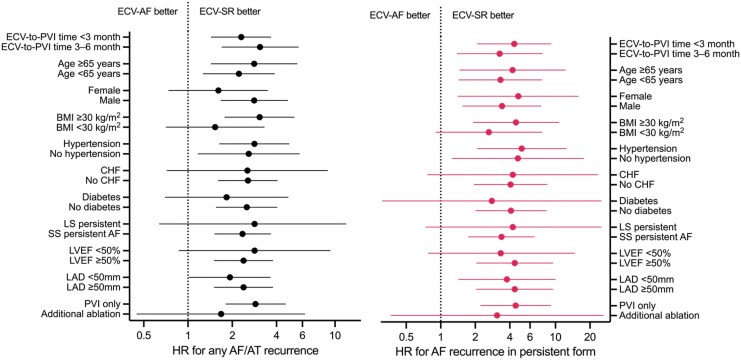 Figure 3
Figure 3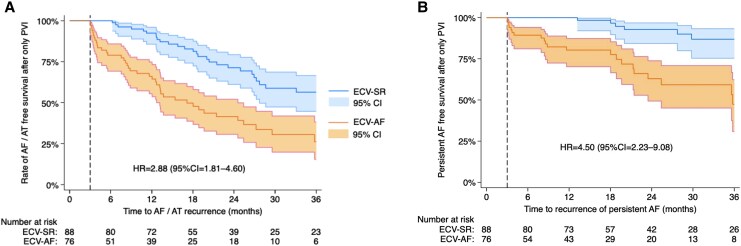 Figure 4
Figure 4| ECV-SR | ECV-AF |
| |
|---|---|---|---|
|
|
| ||
| Age, years | 63.5 (55–69) | 62.5 (54–68) | 0.827 |
| Female sex, | 23 (24.5) | 28 (29.8) | 0.442 |
| BMI, kg/m2 | 29.3 (27.3–32.1) | 29.4 (26.1–33) | 0.901 |
| Time since AF diagnosis, years | 1.5 (0.6–5) | 1 (0.5–3) | 0.343 |
| AF pattern | 0.455 | ||
| Persistent, | 88 (93.6) | 84 (83.4) | |
| Long-standing persistent, | 6 (6.4) | 10 (10.6) | |
| Hypertension, | 56 (59.6) | 65 (69.1) | 0.243 |
| CHF, | 12 (12.8) | 10 (10.6) | 0.832 |
| CAD, | 9 (9.6) | 14 (14.9) | 0.405 |
| VHD, | 6 (6.4) | 6 (6.4) | 1 |
| Stroke/TIA, | 7 (7.4) | 3 (3.2) | 0.219 |
| Diabetes, | 14 (14.9) | 20 (21.3) | 0.362 |
| PAD, | 2 (2.1) | 1 (1.1) | 1 |
| Hypertyreosis, | 0 (0) | 0 (0) | 1 |
| Left atrial diameter, mm | 49 (45.5–52) | 49 (43.5–52) | 0.531 |
| Right atrial diameter, mm | 45.5 (41.5–49) | 46 (39–51.5) | 0.687 |
| E wave velocity, cm/s | 80 (63–98) | 93 (77–100) |
|
| LAA flow velocity, cm/s | 39 (26–52) | 30.5 (26–40) | 0.093 |
| LVEF, % | 55 (53–60) | 55 (53–60) | 0.811 |
| LAVI, mL/m2 | 46.1 (34.7–59.0) | 46.2 (36.3–58.3) | 0.981 |
| CHA2DS2-VA score, | 0.568 | ||
| 0 | 22 (23) | 14 (15) | |
| 1 | 26 (28) | 32 (34) | |
| 2 | 24 (26) | 24 (26) | |
| 3 | 15 (16) | 14 (15) | |
| 4 | 7 (7) | 5 (5) | |
| 5 | 0 (0) | 4 (4) | |
| 6 | 0 (0) | 1 (1) | |
| Type of AAD before ablation | |||
| Amiodarone, | 78 (83) | 83 (88) | 0.460 |
| Propafenone, | 8 (8) | 7 (7) | |
| Sotalol, | 8 (8) | 4 (4) | |
| ECV-to-PVI time, days | 99.5 (71–130) | 102 (69–134) | 0.873 |
| Date of ablation procedure, year | 2018 (2016–2021) | 2017 (2015–2020) | 0.087 |
| Procedure time, min | 80 (70–110) | 90 (70–110) | 0.575 |
| Left atrial dwell time, min | 56.5 (43–75.5) | 57 (42–70) | 0.397 |
| Additional ablation, | 6 (6.4) | 18 (19.1) |
|
| Posterior wall box lesion | 3 (3.2) | 9 (9.6) | |
| Mitral isthmus line | 2 (2.1) | 7 (7.4) | |
| CTI line | 3 (3.2) | 4 (4.3) | |
| CFAE ablation | 0 (0) | 0 (0) | |
| Follow-up duration, months | 42 (22–71) | 41 (17–75) | 0.507 |
| ECV-SR | ECV-AF | RR (95% CI) | |
|---|---|---|---|
|
|
| ||
| Recurrence of AF in persistent form | 12 (40) | 27 (57.5) | 2.25 (1.24–4.17) |
| Recurrence of AF in paroxysmal form | 16 (53.3) | 15 (31.9) | 0.94 (0.50–1.77) |
| Recurrence of AT/AFL | 2 (6.7) | 5 (10.6) | 2.5 (0.58–11.0) |
| Endpoint of AF/AT recurrence | Endpoint of AF recurrence in persistent form | |||
|---|---|---|---|---|
| HR (95% CI) |
| HR (95% CI) |
| |
| VHD | 1.86 (0.82–4.21) | 0.139 | 1.98 (0.58–6.75) | 0.275 |
| Diabetes | 1.67 (0.98–2.83) | 0.058 | 0.61 (0.27–1.40) | 0.242 |
| Long-standing persistent AF | 1.49 (0.67–3.34) | 0.329 | 1.42 (0.40–5.02) | 0.591 |
| LVEF (%) | 0.99 (0.96–1.22) | 0.459 | 0.94 (0.90–0.98) | 0.008 |
| Additional ablation | 0.63 (0.33–1.22) | 0.171 | 0.40 (0.16–1.01) | 0.052 |
| ECV-AF | 2.68 (1.71–4.20) | <0.001 | 6.15 (2.90–13.01) | <0.001 |
- —New National Excellence Program
- —Ministry for Culture and Innovation
- —National Research, Development and Innovation Fund10.13039/501100012550
- —Semmelweis University10.13039/501100002332
- —Gedeon Richter's Talentum Foundation10.13039/501100011903
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac Arrhythmias and Treatments · Cardiac electrophysiology and arrhythmias
Introduction
Atrial fibrillation (AF) is a progressive disease with a natural course characterized by increasing arrhythmia burden and progression from a paroxysmal to persistent form.^1^ This progression is associated with elevated risks for adverse outcomes such as ischaemic stroke, hospitalization for heart failure, or death.^2–4^ Concurrently, the likelihood of maintaining sinus rhythm (SR) diminishes, creating a vicious circle of worsening disease and therapeutic efficacy. Therefore, while pulmonary vein isolation (PVI) is proven effective for the treatment of persistent AF (PeAF),^5^ outcomes fall significantly short of those achieved in paroxysmal AF (PAF).^6^ Efforts to study substrate modification or extrapulmonary trigger ablation techniques in addition to PVI in PeAF patients have yielded mixed results.^7–12^ The latest guidelines classify the usefulness of such ablation strategies as an area of uncertainty,^6^ while according to survey results reported in the same document, one-third of operators routinely perform these techniques in PeAF ablation.^13^ However, it has to be recognized that AF patterns offer minimal insight into underlying mechanisms, such as the PV or extrapulmonary origin of triggers, and structural or electrical substrate remodelling. Consequently, their utility for patient selection is limited, potentially explaining the conflicting results observed in clinical trials with additional ablation techniques in all PeAF patients. There is limited guidance on identifying which patients should undergo PeAF ablation as first-line therapy or who would benefit from additional ablation beyond PVI.^5,6^ According to the recent EHRA survey, 40% of physicians consider the effectiveness of prior electrical cardioversion (ECV) when selecting candidates for ablation^13^; however, the small number of observational studies on this topic produced conflicting results about its utility in predicting the efficacy of procedures.^14–16^ We hypothesize that SR maintenance in patients taking anti-arrhythmic drugs (AADs) after pre-procedural ECV reflects the state of atrial electrical remodelling and therefore could be one of the strongest predictors of rhythm outcomes after ablation procedures. Hence, the goal of this study was to evaluate whether the response to ECV in PeAF patients could predict outcomes after catheter ablation.
Methods
Patient population
This retrospective propensity score matched (PSM) cohort study is based on data from an institutional registry containing prospectively collected information on consecutive procedures and follow-up of patients undergoing catheter ablation for AF at the Heart and Vascular Center of Semmelweis University, Budapest, Hungary. Inclusion criteria were catheter ablation 1–6 months after previous ECV between 2015 and 2022, and persistent AF at the time of ECV, defined as an AF episode lasting >7 days. Exclusion criteria were paroxysmal AF, repeat ablation, no AAD-effect during ECV/no AAD continuation until procedure, and follow-up < 6 months or unavailable data. Details of patient selection and creation of study groups is presented in the study flowchart (Figure 1). After applying inclusion and exclusion criteria, patients were categorized into two groups according to response to ECV: (i) patients in whom SR was restored and maintained until the ablation procedure (ECV-SR group, n = 94), and (ii) patients who have had AF recurrence and presented in AF at the procedure (ECV-AF, n = 123). Then, analysed study groups (both n = 94) were created by 1:1 PSM to account for potential confounding by baseline characteristics. All patients provided written informed consent for the storage and use of their data for research purposes. Ethical approval was obtained from the Semmelweis University Regional Research Ethics Committee (SE RKEB 25/2025).
Study flowchart. AAD, anti-arrhythmic drug; AF, atrial fibrillation; ECV, electrical cardioversion; LTFU, loss to follow-up; PVI, pulmonary vein isolation; SR, sinus rhythm.
Outcomes
The primary outcomes of the present study were (i) freedom from AF and/or atrial tachycardia (AT) on/off AADs following a single ablation procedure, and (ii) recurrence of (or progression to) PeAF during follow-up, after a 3-month blanking period. Secondary outcomes included procedural complications; repeated catheter ablation; pulmonary vein (PV) reconnections at repeat procedures; and progression to permanent AF defined as AV-node ablation with pacemaker implantation, or PeAF accompanied by discontinuation of AADs and no further attempts at ECV or catheter ablation.
Electrical cardioversion
All patients underwent transesophageal echocardiography (TEE) prior to ECV to rule out left atrial thrombus. Synchronized direct current shock was delivered under propofol anaesthesia, with an initial energy of 200 J. If SR was not restored, or AF restarted immediately, shocks with 360 J were applied. The procedure was discontinued after a maximum of three unsuccessful attempts with 360 J. Upon awakening, patients were assessed for neurological signs, and they were monitored for 6 h during which the potential recurrences were documented.
Catheter ablation procedures
All patients took either amiodarone, propafenone, or sotalol before the procedures. Either TEE or contrast-enhanced left atrial computed tomography was used to exclude thrombi. Catheter ablation was performed under conscious sedation. After accessing the femoral vein, double transseptal puncture was applied under fluoroscopy guidance. An electroanatomical mapping system (either CARTO, Biosense Webster Inc., Diamond Bar, CA, USA; or ENSITE, Abbott Laboratories, Abbott Park, Illinois, USA) and a multi-polar mapping catheter were used to create an anatomical left atrial map. Wide, antral radiofrequency PVI was carried out with a point-by-point technique using a steerable sheath and a contact-force sensing ablation catheter. Once the initial circle was completed, the mapping catheter was used to check for gaps in the ablation line. Additional applications were delivered at these sites until complete PVI was achieved, confirmed by entrance and exit blocks in all PVs. Adjunctive ablation targeting empirical non-PV triggers (superior vena cava, vein of Marshall) and substrate modification (posterior wall isolation, other linear lesions) was performed rarely in selected cases. The decision to perform adjunctive ablation was made at the discretion of the operating physician, based on patient-related factors and intra-procedural findings, such as failure to terminate AF by PVI, or emergence of macroreentrant atrial tachycardias. Systematic voltage mapping or trigger induction protocols were not performed during procedures. Patients in AF at the end of the procedure were cardioverted to SR.
Follow-up period
A 3-month blanking period was applied after the catheter ablation procedure, during which rhythm outcomes were not assessed. Atrial tachyarrhythmia recurrence (AF or AT/flutter of at least 30 s) was monitored in all patients by standard of care follow-up, with 12-lead electrocardiograms and 24 h Holter monitoring at 3-month visits in the first year and annually thereafter, or sooner in case of arrhythmia symptoms. The decision to discontinue AADs was left to the discretion of the treating physician. In the case of recurrence of atrial arrhythmias, AADs were reinitiated, and as a first step, patients were scheduled for ECV 4 weeks after the documentation of recurrence. If AF persisted until the scheduled visit, the cardioversion was performed and the recurrence was categorized as PeAF. The option for repeated ablation was evaluated by shared decision-making with the patient. During repeat procedures, PV reconnections were assessed, and PVs were reisolated. If AF persisted despite continued attempts at rhythm control, treating physicians could opt to discontinue AADs and pursue rate control including atrioventricular node ablation with pacemaker implantation. In such cases, the study endpoint of permanent AF was reached. The minimum duration of follow-up required to be included in this study was 6 month.
Data collection
Patient characteristics (demographic information, disease history, medications, and TEE measurements), procedural and follow-up data were prospectively evaluated and collected in the institutional registry. These data were augmented by retrospective collection of missing information about patient characteristics and rhythm outcomes from electronic health records, and by contacting patients. Events of arrhythmia recurrence (both pre- and post-ablation) were registered in the case of atrial arrhythmia recorded by a 12-lead electrocardiogram, Holter monitoring, or cardiac implantable electronic devices. In the case of recorded recurrence, the type of atrial arrhythmia was categorized as paroxysmal AF, AT/AFL, or persistent AF (duration > 7 days). The progression of AF from paroxysmal to persistent (in the case of initial PAF recurrence) and from persistent to permanent form was also registered during data collection. The correct entry of study endpoints was monitored by a separate researcher blinded to study group allocation.
Statistical methods
To create comparison groups, propensity scores were estimated with logistic regression based on the following 16 covariates: age, sex, CHA_2_DS_2_-VA score, left ventricular ejection fraction (LVEF), left atrial diameter (LAD), long-standing PeAF, hypertension, diabetes, chronic heart failure (CHF), valvular heart disease (VHD), coronary artery disease (CAD), stroke/transient ischaemic attack (TIA), additional ablation beyond PVI, time from ECV to ablation, year of ablation, and follow-up duration. Then patients were matched 1:1 using nearest neighbour PSM without replacements. The characteristics of the unmatched groups were compared with χ^2^-test or Fisher’s exact test in the case of binary variables, and the Mann–Whitney ranksum test in the case of non-parametric continuous or ordinal data. Characteristics of PSM groups were compared in a pairwise manner with McNemar’s test for binary data and the Wilcoxon signed-rank test for non-parametric continuous or ordinal data. Kaplan–Meier curves were generated to visualize cumulative incidence outcomes with 95% confidence intervals (CI). The log-rank test was used to compare freedom from AF between the matched groups. Multi-variable Cox proportional hazard regression was performed to eliminate remaining confounding effects and to assess the effect of other covariates in the outcome. Clinically relevant predictors (P < 0.25) or variables differing across matched groups were included in initial models. Then, a stepwise backward elimination method was used to exclude variables that did not influence the fit of the model. Schoenfeld’s residual test was performed to assess the proportional hazard assumption. Multiple imputation with 20 imputed datasets was used for missing values of LVEF (22% missing) and LAD (23% missing). Estimates were combined across datasets for the calculation of propensity scores and hazard ratios. Variables with missing values exceeding 25% were excluded from regression models. Subgroup analysis was performed to assess effect-modifications on the primary outcomes. P-values are reported for the primary outcomes and for comparison of baseline characteristics with the alpha level for significance set at 0.05. Statistical analyses were conducted using Stata (StataCorp LLC, College Station, TX, USA, release 18) and GraphPad Prism 10 (GraphPad Softwares Inc., San Diego, CA, USA) software.
Results
Characteristics of study groups
Characteristics of the unmatched population are presented in Supplementary material online, Table S1. After PSM, baseline characteristics were similar across study groups (Table 1), with a significant difference being the higher frequency of additional ablation beyond PVI in the ECV-AF group (19.1% vs. 6.4%, P = 0.023). In ECV-AF patients, SR could not be restored or AF immediately returned after ECV in 16 patients, and 7 had AF recurrence during the observation period after restoring SR. AF was documented in 38 patients between ECV and catheter ablation, while in 33 it was registered at the start of the procedure.
Outcomes
The median duration of follow-up was 42 (20–73) month in the overall cohort. The rate of freedom from AF/AT on/off AADs at 12 months was 91.7% in the ECV-SR group and 67% in the ECV-AF group; while at 36 months the rate was 51.2% and 31.4%, respectively (crude HR = 2.58, 95% CI = 1.58–3.70, P < 0.001; Figure 2A). The most frequent type of atrial arrhythmia recurrence was paroxysmal AF in the ECV-SR group and persistent AF in the ECV-AF group (Table 2). After multi-variable adjustment, ECV-AF (HR = 2.68, 95% CI = 1.71–4.20) was the only significant predictor of AF/AT recurrence following ablation (Table 3).
Kaplan–Meier curves with 95% CI for the rate of AF/AT free survival (A) and the rate of persistent AF-free survival (B) after a single procedure in the ECV-SR and ECV-AF groups. Dashed lines indicate the end of the 3-month blanking period. AF, atrial fibrillation; AT, atrial tachycardia; CI, confidence interval; HR, hazard ratio.
The incidence rate for the recurrence of—or progression to—persistent AF was 7.5/100 patient-years (95% CI = 4.5–12.5) in the ECV-SR group and 22.8/100 patient-years (95% CI = 16.0–32.4) in the ECV-AF group. Freedom from persistent AF at 12 months was 100% and 80.6%; while at 36 months it was 84.3% and 54%, respectively (crude HR = 3.72, 95% CI = 1.94–7.14, P < 0.001; Figure 2B). In the multi-variable model (Table 2), significant predictors were AF recurrence after ECV (HR = 6.15, 95% CI = 2.90–13.01) and LVEF (measured in %, HR = 0.94, 95% CI = 0.90–0.98). Furthermore, additional ablation was at the threshold of significance associated with PeAF free survival (HR = 0.40, 95% CI = 0.16–1.01). Proportional hazard assumptions were met for all Cox-regression models (Schoenfeld test P > 0.9).
Differences in the risk of the primary outcomes were similar in analysis of subgroups according to ECV-to-PVI time, age, sex, BMI, hypertension, CHF, diabetes, AF pattern, ablation strategy, LVEF, and LAD categories (Figure 3). Kaplan–Meier curves for the PVI-only subgroup are presented in Figure 4. The curves show a similar extent of separation as the main analysis, with HR = 2.88 (95% CI = 1.81–4.60) for AF/AT recurrence, and HR = 4.50 (95% CI = 2.23–9.08) for recurrence of persistent AF.
Hazard ratios for the effect of ECV response on the primary outcomes according to subgroups of patient characteristics and clinical parameters. AF, atrial fibrillation; AT, atrial tachycardia; BMI, body-mass index; CHF, chronic heart failure; HR, hazard ratio; LAD, left atrial diameter; LS, long-standing; LVEF, left ventricular ejection fraction; ECV, electrical cardioversion; PVI, pulmonary vein isolation; SS, short standing (duration < 1 year).
Kaplan–Meier curves with 95% CI for the rate of AF/AT free survival (A) and the rate of persistent AF-free survival (B) after a single procedure in the PVI-only group. Dashed lines indicate the end of the 3-month blanking period. AF, atrial fibrillation; AT, atrial tachycardia; CI, confidence interval; HR, hazard ratio.
No major complication occurred as a result of ablation procedures. There were three cases of groin hematoma in the ECV-SR group not needing surgical repair. Repeated ablation was performed in 19 and 25 patients in the two groups (20% vs. 27%, RR = 1.32; 95% CI = 0.79–2.22), respectively. During repeat procedures, 52/75 (69.3%) PVs were found to be reconnected in ECV-SR patients and 56/93 (60.2%) in ECV-AF patients (RR = 0.77, 95% CI = 0.50–1.164). After multiple procedures, AF-free survival was similarly lower in the ECV-AF group, although the difference is somewhat less pronounced (HR = 1.83, 95% CI = 1.16–2.90, supplementary material online, Figure S1). The rate of progression to permanent AF was 4.3% in the ECV-SR group and 10.6% in the ECV-AF group over the total follow-up (RR = 2.5, 95% CI =0.86–7.34).
Discussion
The main observation of this study is that patients with PeAF on AADs, who maintain SR after ECV prior to ablation, have favourable rhythm outcomes after catheter ablation. Conversely, subjects with AF recurrence until the procedure have a significantly worse prognosis. The clinical relevance of this finding lies in the use of post-ECV SR maintenance as a simple and practical guide for identifying persistent AF patients in whom a PVI-only strategy may not be sufficient.
Existing literature on this topic includes a small number of retrospective observational studies. Kamada et al. categorized PeAF patients into two groups: those in whom SR was successfully restored by ECV (161 patients) and those in whom it was not (34 patients).^15^ They reported higher freedom from AF off AADs in the SR group. A recent study by Limite et al., the most comparable to ours, included 58 patients maintaining SR until the ablation procedure (at least 4 weeks from ECV), and 89 who reverted to AF after ECV.^16^ They report no difference in AF-free survival between groups. However, among patients presenting in SR at the procedure, PVI alone resulted in better freedom from AF than PVI + additional ablation. These patients also exhibited less frequent and less extensive low-voltage areas. Compared to these investigations, the novelty and strength of the present study are the following: (i) greater number of patients, (ii) propensity score-matched analysis, (iii) more rigorously defined patient selection criteria by exclusion of patients off AADs and ECV outside of 1–6-month pre-ablation time-window, and (iv) evaluation of endpoints also reflecting progression of AF.
Some other studies investigated similar research questions. One study observed that pre-ablation ECV shock energy and the number of shocks required to restore SR were higher in PeAF patients who experienced recurrences after ablation.^17^ Another investigation compared PeAF patients who maintained SR for at least 1 month after ECV with patients in whom ECV was not performed, and reported similar 12-month freedom from atrial tachyarrhythmia in the two groups, but concluded that the extent of ablation required to terminate AF during procedures is lower in the SR group.^14^ In an analysis of a long-standing PeAF population divided based on whether SR restoration with AADs and ECV was accomplished or not, lower rates of recurrence was observed in the SR group. Additionally, observational studies have highlighted the prognostic value of pre-procedural pharmacologic cardioversion with a similar effect as ECV.^18^ It can be concluded that the atrial rhythm before and during ablation procedures is an important predictor of procedural efficacy,^19^ and AF management strategies including AADs and ECV before the procedure can increase the accuracy and standardize this risk stratification approach.
The anticipated benefit of catheter ablation is a major factor influencing patient selection decisions.^20–25^ However, accurately predicting this benefit remains a significant challenge. Risk scores such as the APPLE score and CAAP-AF score, designed to predict AF recurrence after ablation, have demonstrated poor performance.^26,27^ Publications aimed at studying patient selection strategies for PVI or for additive substrate ablation are scarce. In the DECAAF II trial, pre-ablation MRI guided fibrosis ablation combined with PVI showed no significant difference in atrial arrhythmia recurrence compared to PVI alone in PeAF patients.^12^ This suggests that pre-ablation MRI is not effective at selecting patients to undergo additional ablation beyond PVI. It may be possible that the much more accessible strategy of rhythm monitoring following ECV could guide the selection of patients to undergo additional ablation beyond PVI, which is investigated in the ongoing PACIFIC trial (NCT05264831).^28^
According to a recent EHRA survey asking physicians which factors they consider during patient selection, more than 80% take into account left atrial size, age, severity of AF symptoms, coexistence of heart failure, and the presence of obesity; whereas only 42% consider previous response to ECV.^13^ According to the results of our study, the response to ECV is a strong predictor of the long-term efficacy of ablation of PeAF when keeping all other variables (including age and left atrial size) constant. Such a risk stratification approach could have a wide range of clinical applications to tailor treatment strategies to individual patients. If the decision is to ablate ECV-AF patients, it might be reasonable to consider more extensive ablation techniques beyond PVI. This also has implications for procedural planning, as these patients might be more suitable for an approach with systematic substrate mapping, and substrate modification (when appropriate) rather than a single-shot PVI-only procedure. Other potential clinical applications might include informing the timing of ablation, which ideally should be performed in ECV-AF patients as early as possible before further atrial remodelling develops. ECV response could also help in guiding post-procedural management. In this cohort, 25% of ECV-AF patients had an early recurrence in the first 4–5 months after ablation, while the early recurrence rate in ECV-SR patients was 0%. This suggests that the selection of patients for short-term post-procedural AAD therapy based on ECV response might be effective to reduce the number of early cardioversions and arrhythmia-related hospitalizations. Finally, this approach could support shared decision-making and effective communication with the patient about the expected benefits of the procedure.
Limitations of this study need to be mentioned. Due to its retrospective nature, ablation techniques and follow-up methods were not standardized during the study period, and unmeasured confounders may have impacted the results. To mitigate confounding and bias, stringent inclusion and exclusion criteria, PSM, and multi-variable regression methods were employed. This retrospective study does not identify the exact mechanisms underlying AF recurrences after ECV as substrate mapping or trigger induction and localization were not part of procedural protocols.
Conclusion
The recurrence rates of atrial arrhythmias were higher in ECV-AF than in ECV-SR patients. Results from this propensity score-matched cohort suggest that the response to pre-procedural ECV may serve as a valuable marker for identifying persistent AF patients in whom a PVI-only strategy is sufficient.
Lead author biography
Dr Márton Boga received his medical degree at Semmelweis University in 2024 and completed the Clinical Science Scholars Programme at Harvard Medical School. Dr Boga is involved in clinical research as a PhD candidate under the supervision of Dr Nándor Szegedi at the Heart and Vascular Center, Budapest, Hungary. Their research focuses on cardiac electrophysiology, with a particular interest in catheter ablation techniques for atrial fibrillation. Outside of medicine, he is an avid ice hockey player and passionate windsurfer.
Supplementary Material
oeaf084_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blum S, Meyre P, Aeschbacher S, Berger S, Auberson C, Briel M, Osswald S, Conen D. Incidence and predictors of atrial fibrillation progression: a systematic review and meta-analysis. Heart Rhythm 2019;16:502–510.30366160 10.1016/j.hrthm.2018.10.022 · doi ↗ · pubmed ↗
- 2Steinberg BA, Hellkamp AS, Lokhnygina Y, Patel MR, Breithardt G, Hankey GJ, Becker RC, Singer DE, Halperin JL, Hacke W, Nessel CC, Berkowitz SD, Mahaffey KW, Fox KAA, Califf RM, Piccini JP. Higher risk of death and stroke in patients with persistent vs. Paroxysmal atrial fibrillation: results from the ROCKET-AF trial. Eur Heart J 2015;36:288–296.25209598 10.1093/eurheartj/ehu 359PMC 4313363 · doi ↗ · pubmed ↗
- 3Link MS, Giugliano RP, Ruff CT, Scirica BM, Huikuri H, Oto A, Crompton AE, Murphy SA, Lanz H, Mercuri MF, Antman EM, Braunwald E. Stroke and mortality risk in patients with Various patterns of atrial fibrillation. Circ Arrhythm Electrophysiol 2017;10:e 004267.28077507 10.1161/CIRCEP.116.004267 · doi ↗ · pubmed ↗
- 4Chew DS, Li Z, Steinberg BA, O'Brien EC, Pritchard J, Bunch TJ, Mark DB, Patel MR, Nabutovsky Y, Greiner MA, Piccini JP. Arrhythmic burden and the risk of cardiovascular outcomes in patients with paroxysmal atrial fibrillation and cardiac implanted electronic devices. Circ Arrhythm Electrophysiol 2022;15:e 010304.35089799 10.1161/CIRCEP.121.010304 · doi ↗ · pubmed ↗
- 5Van Gelder IC, Rienstra M, Bunting KV, Casado-Arroyo R, Caso V, Crijns HJGM, De Potter TJR, Dwight J, Guasti L, Hanke T, Jaarsma T, Lettino M, Løchen M-L, Lumbers RT, Maesen B, Mølgaard I, Rosano GMC, Sanders P, Schnabel RB, Suwalski P, Svennberg E, Tamargo J, Tica O, Traykov V, Tzeis S, Kotecha D, Dagres N, Rocca B, Ahsan S, Ameri P, Arbelo E, Bauer A, Borger MA, Buccheri S, Casadei B, Chioncel O, Dobrev D, Fauchier L, Gigante B, Glikson M, Hijazi Z, Hin · doi ↗ · pubmed ↗
- 6Tzeis S, Gerstenfeld EP, Kalman J, Saad EB, Sepehri Shamloo A, Andrade JG, Barbhaiya CR, Baykaner T, Boveda S, Calkins H. 2024 European heart rhythm association/heart rhythm society/Asia Pacific heart rhythm society/Latin American heart rhythm society expert consensus statement on catheter and surgical ablation of atrial fibrillation. EP Europace 2024;26:27–28.
- 7Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, Macle L, Morillo CA, Haverkamp W, Weerasooriya R, Albenque J-P, Nardi S, Menardi E, Novak P, Sanders P. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med 2015;372:1812–1822.25946280 10.1056/NEJ Moa 1408288 · doi ↗ · pubmed ↗
- 8Huo Y, Gaspar T, Schönbauer R, Wójcik M, Fiedler L, Roithinger FX, Martinek M, Pürerfellner H, Kirstein B, Richter U, Ulbrich S, Mayer J, Krahnefeld O, Agdirlioglu T, Zedda A, Piorkowski J, Piorkowski C. Low-voltage myocardium-guided ablation trial of persistent atrial fibrillation. NEJM Evid 2022;1:EVI Doa 2200141.38319851 10.1056/EVI Doa 2200141 · doi ↗ · pubmed ↗