Antenatal Diagnosis of a True Knot of the Umbilical Cord: A Rare Case With a Successful Surgical Outcome
Sarmistha Gupta, Rajalakshmi Srinivasan

TL;DR
A rare case of a true umbilical cord knot was diagnosed before birth, leading to a successful surgical delivery and a healthy baby.
Contribution
This case report presents a rare antenatal diagnosis of a true umbilical cord knot with a successful outcome.
Findings
Antenatal diagnosis of a true umbilical cord knot was made at 35 weeks' gestation.
Emergency cesarean section led to the delivery of a healthy neonate.
Color Doppler ultrasound and maternal vigilance aided in the early detection.
Abstract
True knots of the umbilical cord (TKUCs) are rare and can compromise fetal well-being. Their diagnosis is typically made at delivery, with antenatal identification remaining rare. This case report describes an antenatal diagnosis of a TKUC at 35 weeks’ gestation in a 28-year-old third gravida with two previous miscarriages. The patient presented with reduced amniotic fluid and absent fetal movements. Ultrasound imaging raised suspicion of a TKUC, prompting an emergency cesarean section. A healthy neonate was delivered. This case highlights the potential role of color Doppler ultrasound and maternal vigilance in identifying TKUCs before delivery. Despite diagnostic challenges, heightened clinical awareness and timely intervention can contribute to favorable perinatal outcomes. Future research should aim to improve diagnostic accuracy and develop effective risk-stratification tools.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
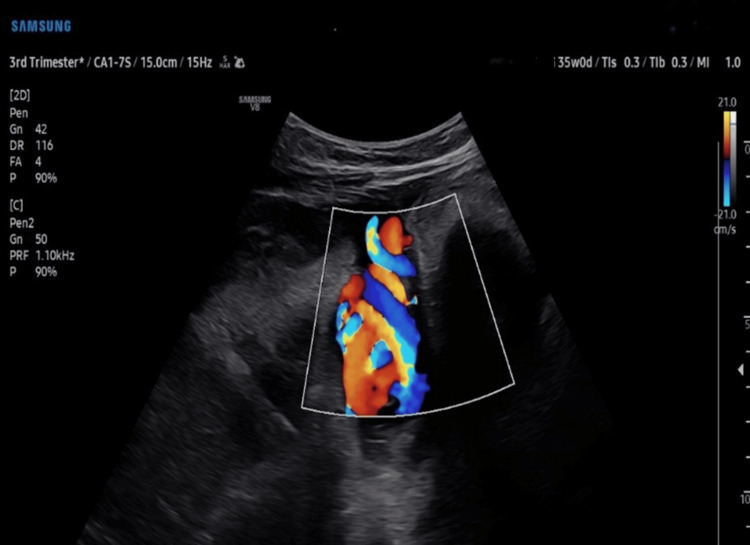 Figure 1
Figure 1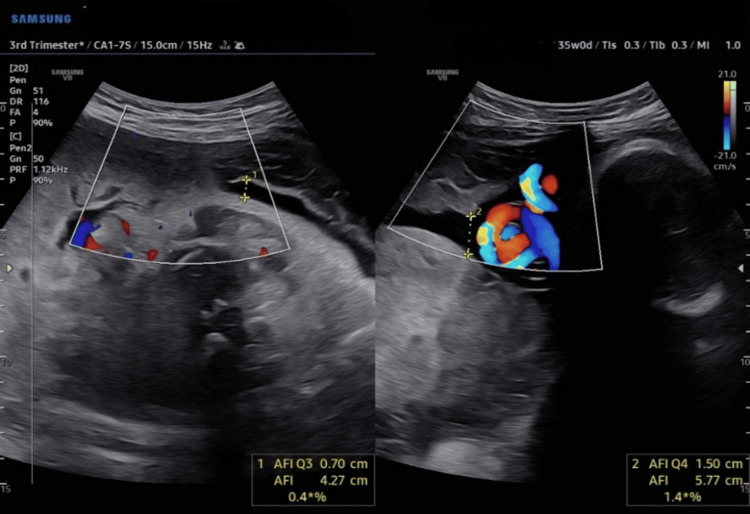 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Anomalies and Fetal Surgery · Tumors and Oncological Cases · Congenital Diaphragmatic Hernia Studies
Introduction
True knots of the umbilical cord (TKUCs) are a rare but clinically significant obstetric event, occurring in approximately 0.3% to 2.1% of pregnancies [1,2]. While many knots remain asymptomatic and go undetected, tight knots can compromise fetal circulation, leading to complications like hypoxia, intrauterine growth restriction, or stillbirth, with perinatal mortality increasing up to fourfold [2-4]. True knots are believed to form between 9 and 12 weeks of gestation [2,5], likely influenced by increased fetal mobility and abundant amniotic fluid during early pregnancy.
Antenatal identification of TKUC continues to pose a significant diagnostic challenge, despite advances in imaging technology, primarily due to the dynamic nature of the cord and the limited sensitivity of conventional ultrasound, with detection rate reported as low as 12% [2,3]. Nonetheless, early diagnosis is crucial, as it enables timely and potentially life-saving obstetric interventions aimed at reducing perinatal morbidity and mortality.
Advanced imaging modalities such as color Doppler, power Doppler, and 3D sonography have improved the antenatal detection of TKUCs [3,6]. However, false positives in these techniques may arise due to misinterpretation of cord configurations or other abnormalities that mimic malformations, most of which do not require intervention [1,6]. False knots, more accurately termed "nodus spurious vasculosis," represent benign vascular redundancies of umbilical vessels and do not pose clinical risk [6]. These can mimic true knots on ultrasound, but advanced modalities like color Doppler and 3D imaging allow for clear differentiation based on characteristic findings [6].
TKUCs are associated with several maternal and fetal risk factors, including advanced maternal age, multiparity, polyhydramnios, long umbilical cords, and small-for-gestational-age (SGA) fetuses [2]. Several studies have identified male fetal sex as the most significant risk factor [4,7,8], likely attributed to the generally longer umbilical cords observed in male fetuses [7,8].
This case report presents a rare incidence of antenatal diagnosis of a TKUC, confirmed intraoperatively. The case underscores current diagnostic tools' limitations, imaging's potential role, and the need for heightened clinical awareness in high-risk pregnancies. These gaps underscore the need for prospective studies evaluating the diagnostic accuracy of imaging techniques, development of standardized management protocols, and further exploration into the natural history and clinical impact of TKUC when diagnosed antenatally. By sharing this experience, we aim to contribute to the limited body of literature addressing antenatal identification of TKUC and highlight its implications for clinical management and fetal outcomes.
Case presentation
Presentation and clinical history
A 28-year-old, third gravida with a history of two previous abortions was receiving routine antenatal care. Due to her obstetric history, a cervical cerclage was placed during the first trimester. She underwent regular radiological scans throughout her pregnancy. At 33 weeks of gestation, a radiological scan identified reduced amniotic fluid but showed no disparity in fetal growth. The patient was afebrile, with a pulse rate of 78 beats per minute and a blood pressure of 110/76 mmHg. Fetal heart sounds (FHS) were noted to be 142 beats per minute. Obstetric Doppler findings were within normal limits. The patient continued to be monitored at the OB/GYN clinic for amniotic fluid levels.
Investigations and diagnosis
At 35 weeks of gestation, the patient was referred to radiology to reassess the amniotic fluid index (AFI), following a clinical suspicion of reduced fluid levels. The radiological scan revealed a borderline AFI of 5.7. Notably, the scan also identified a loop of the umbilical cord around the fetal neck and a true knot in the umbilical cord (as shown in Figures 1, 2). The obstetrician was immediately informed, and the patient who reported reduced fetal movements was advised to monitor fetal movements closely.
A true knot in the umbilical cord
A true knot in the umbilical cord adjacent to the fetal head and AFI of 5.77 cmAFI: amniotic fluid index.
Treatment plan and surgical intervention
Two days later, the patient presented with an absence of fetal movements for the past six hours. Cardiotocography (CTG) revealed suspicious findings, raising concerns about fetal well-being. An emergency lower segment cesarean section (LSCS) was performed with concurrent removal of the cervical stitch. Intraoperatively, a tight true knot in the umbilical cord was confirmed, consistent with the antenatal ultrasound diagnosis (as shown in Figure 3). A male baby weighing 2.29 kg was delivered in stable condition with Apgar scores of 9 at 1 minute and 9 at 5 minutes. The neonate was roomed in with the mother, and breastfeeding was initiated within the first hour.
Intraoperative image showing surgical removal of the umbilical cord with a true knot and a long umbilical cord
Postoperative course
The postoperative period was uneventful. Recovery was normal, with the patient passing flatus and urinating normally on the first postoperative day. Bowel movements resumed after 34 hours. Bleeding per vagina (lochia) remained within normal limits. She was discharged 48 hours after delivery.
Follow-up
Follow-up after one week revealed that the skin incision had healed externally and the mother was breastfeeding normally. However, complete healing of the LSCS scar was achieved after several weeks.
Discussion
Incidence and clinical relevance
TKUCs occur in approximately 0.3%-2.1% of pregnancies [1,3,5], with clinical outcomes ranging from benign to life-threatening. While a diagnosis of many cases is incidental and results in favorable outcomes [9], others are associated with serious complications such as intrauterine growth restriction (IUGR), fetal hypoxia, neurological impairment, and stillbirth [5]. Several studies have linked TKUCs to adverse outcomes like fetal demise [1,3,8]. These divergent findings underscore the influence of critical variables, including the degree of knot tightness [6], co-existing cords [10,11] or placental abnormalities [8], and other maternal-fetal conditions.
Several risk factors are associated with the formation of TKUC, including advanced gestational age, polyhydramnios, male fetus, long umbilical cord, multiparity, and a history of pregnancy loss [3,4,9,10]. Among which fetal male sex has been most consistently identified in the literature as a significant predisposing factor [1-8]. Our case highlights the significance of such contextual factors. The patient exhibited multiple risk factors for TKUCs, including multiparity, advanced gestation, and a male fetus; however, a borderline AFI of 5.7 was also noted, although it is not commonly among the typical risk factors like polyhydramnios, which has been associated with increased fetal mobility and knot formation. Subsequently, fetal movement cessation and CTG findings warranted an emergency cesarean delivery.
Pathophysiology
Increased fetal movement during early pregnancy is believed to contribute to the formation of TKUCs by promoting the looping of the cord [6]. However, adverse outcomes are more likely to manifest in the third trimester, when the natural decline in amniotic fluid volume limits cord mobility, increasing the risk of knot tightening [3]. One plausible, though unproven, hypothesis suggests that a TKUC may itself contribute to reduced amniotic fluid levels. A tightly formed knot can impair umbilical blood flow [3,5], potentially leading to decreased fetal renal perfusion and diminished urine output, an essential component of amniotic fluid volume regulation.
The umbilical cord serves as a vital conduit for oxygen, nutrients, and fetal circulation. The presence of a knot can impede venous return and compromise the delivery of oxygenated blood to the fetus, as reported by Waldron et al [8]. Partial obstruction of blood flow may lead to complications such as IUGR, while complete or acute compression can result in sudden fetal distress or even fetal demise [5].
Diagnostic limitations and imaging advances
Diagnosis of TKUC remains a significant clinical challenge; however, advances in imaging modalities such as 3D and 4D sonography, as well as color and power Doppler imaging, have improved detection rates [3,5]. A study conducted by Carter et al, has explored the potential of electronic fetal monitoring (EFM) parameters in detecting TKUC; however, the findings demonstrated limited correlation [7], rendering the diagnostic utility of EFM inconclusive.
Although 3D sonography, Color Doppler, and power Doppler have been suggested as potentially useful [3,6]; they are not definitive. These imaging techniques can sometimes yield false-positive results [1,6], and routine ultrasound often fails to detect many knots, increasing the risk of fetal complications. Given the limitations of current diagnostic tools and the potential for unnecessary interventions due to misinterpretation, there is a clear need for more accurate and validated imaging techniques to improve antenatal detection of TKUC.
Clinical management and follow-up considerations
Many authors have highlighted the absence of standardized guidelines for managing pregnancies complicated by TKUC [2,5,6,10], leading to variability in clinical practices. However, antenatal diagnosis of TKUC has been associated with improved fetal outcomes [2]. In our case, a multidisciplinary approach that included close fetal surveillance and early recognition of the TKUC facilitated timely intervention and resulted in a favorable neonatal outcome.
Risk stratification for pregnancies complicated by TKUCs should incorporate factors such as decreased amniotic fluid, multiple gestation, excessive cord length, male sex, multiparity, among others. When these risk factors are identified, a tailored monitoring plan may be necessary. Furthermore, educating patients on daily fetal movement counting may facilitate timely reporting of changes, as was observed in our case.
Postnatal evaluation of both the neonate and the mother is essential, particularly following TKUC-associated complications. Follow-up should include monitoring for any signs of neonatal hypoxia and other related complications. Additionally, counselling for the mother is important to address the potential implications for future pregnancies and provide appropriate guidance.
Although the information provided is based on incidental findings, our experience underscores the unpredictability of TKUCs, and the challenges associated with their antenatal diagnosis. While often benign, their presence carries uncertain perinatal risks. Detection alone should not alter the planned obstetric approach but warrants careful monitoring and preparedness. Although there are no standardized protocols for managing TKUCs, individualized care involving detailed patient counseling, daily fetal movement monitoring, and fetal surveillance is essential. Delivery is typically considered if signs of fetal compromise arise or if the pregnancy reaches term, rather than based on the presence of a true knot alone [6].
Clinical implications
This case reinforces the clinical complexity and potential severity of TKUC. While not all knots result in adverse outcomes, tight TKUCs, especially in the presence of coexisting risk factors, pose a significant threat to fetal well-being. Early identification through advanced imaging, such as 3D power sonography, is essential. Further research, particularly prospective studies and meta-analyses, is essential to identify effective diagnostic strategies and to establish evidence-based screening and management protocols for TKUC.
Maternal follow-up should focus on recovery from delivery and assessment of any obstetric complications associated with TKUC, such as placental insufficiency or abnormal uterine perfusion. Postpartum counselling regarding future pregnancy risks and the potential recurrence of TKUC can provide valuable guidance for affected mothers.
Conclusions
This case highlights the critical role of advanced imaging and vigilant fetal monitoring in the antenatal detection of a TKUC, which directly contributed to a favorable perinatal outcome. Clinicians should maintain a high index of suspicion in high-risk pregnancies and utilize advanced Doppler imaging for early recognition. This case reinforces the importance of antenatal education, particularly regarding fetal movement monitoring. Encouraging patients to report reduced fetal activity can lead to early intervention, potentially improving neonatal outcomes. Future research should focus on establishing standardized diagnostic criteria and assessing the efficacy of advanced imaging techniques in TKUC detection and management
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A misdiagnosed case of a 150-cm umbilical cord coiled twice around the fetal neck with a true cord knot: a rare Syrian case report SAGE Open Med Case Rep Hanna M Martini N Deeb Y Mahmoud W Issa SY 205031311202310.1177/2050313 X 231164858 PMC 1007461437032995 · doi ↗ · pubmed ↗
- 2Adverse perinatal outcomes of true knot of the umbilical cord: a case series and review of literature Cureus Agarwal I Singh S 014202210.7759/cureus.26992 PMC 938540835989783 · doi ↗ · pubmed ↗
- 3True knot of the umbilical cord and associated adverse perinatal outcomes: a case series Cureus Gaikwad V Yalla S Salvi P 015202310.7759/cureus.35377 PMC 1003981636987486 · doi ↗ · pubmed ↗
- 4True double umbilical cord knot BMJ Case Rep Laranjo M Neves BM Peixinho C 15202210.1136/bcr-2022-251388 PMC 937950735953150 · doi ↗ · pubmed ↗
- 5Umbilical cord knots: is the number related to fetal risk?Medicina (Kaunas) Stabile G Carlucci S De Bonis L Sorrentino F Nappi L Ricci G 58202210.3390/medicina 58060703 PMC 922995835743964 · doi ↗ · pubmed ↗
- 6Current perspectives of prenatal sonographic diagnosis and clinical management challenges of true knot of the umbilical cord Int J Womens Health Sherer DM Amoabeng O Dryer AM Dalloul M 2212331220203227377810.2147/IJWH.S 192260 PMC 7115211 · doi ↗ · pubmed ↗
- 7True knot at the time of delivery: electronic fetal monitoring characteristics and neonatal outcomes J Perinatol Carter EB Chu CS Thompson Z Tuuli MG Macones GA Cahill AG 162016243820183032332310.1038/s 41372-018-0250-4PMC 6279587 · doi ↗ · pubmed ↗
- 8Double and single true knot of an umbilical cord: a case report Cureus Waldron JE Muir SM Hubbard J 015202310.7759/cureus.36393 PMC 1011574737090371 · doi ↗ · pubmed ↗