Correction: Targeting TRPM3 as a potential therapeutic approach for autosomal dominant polycystic kidney disease
Hüseyin Gül, Jamie A. Davies

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
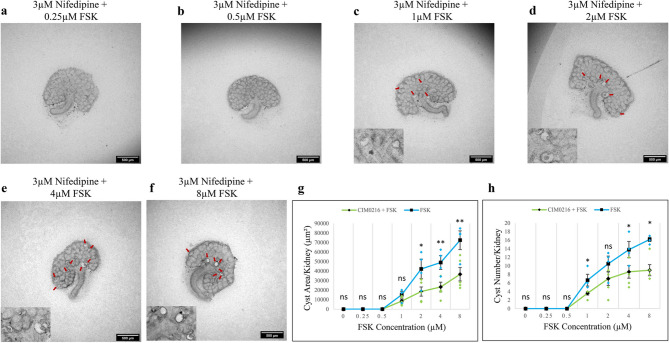 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and Kidney Cyst Diseases · Biomedical Research and Pathophysiology
Correction to: Scientific Reports 10.1038/s41598-025-89200-z, published online 08 February 2025
The original version of this Article contained an error in Figure 7, panels g and h, where the labels mistakenly repeated those from Figure 6. The original Figure 7 and accompanying legend appear below.
Fig. 7. Nifedipine attenuated FSK-driven cyst formation. Cultured E12.5 kidneys were treated with 3 µM nifedipine and varying concentrations of FSK. Cyst formation was imaged and quantified after 2 days of culture. (a–f) Brightfield images of E12.5 kidney rudiments treated with 3 µM nifedipine and 3 µM nifedipine with 0.25 µM, 0.5 µM, 1 µM, 2 µM, 4 µM and 8 µM FSK. (g,h) Quantification of cystic areas and cyst numbers in E12.5 kidney rudiments after 2 days of 3 µM nifedipine with varying concentrations of FSK (green line) and FSK alone (blue line). Cysts were indicated by red arrows. In (g) and (h), data are means of at least 3 kidneys. Error bars indicate standard errors of the mean. p-values were calculated using unpaired t-tests. *p < 0.05, **p < 0.008, ns; not significant. The FSK data presented are reproduced from Fig. 1.
The original Article has been corrected.