Expanding the diagnostic spectrum of malignant otitis externa: a case report of proteus infection in a non-immunosuppressed patient
Fabián Darío Arias Rodríguez, Mercedes Larenas, Santiago Paredes, Guillermina Giuliano, Andrés López-Cortés, Juan S. Izquierdo-Condoy

TL;DR
A rare case of malignant otitis externa caused by Proteus mirabilis in a non-diabetic, immunocompetent patient is reported, highlighting the importance of considering atypical pathogens.
Contribution
This is one of the few documented cases of Proteus mirabilis causing MOE in a non-immunosuppressed individual.
Findings
Proteus mirabilis was identified as the causative agent in a non-diabetic, immunocompetent patient with MOE.
The patient responded to piperacillin/tazobactam therapy followed by oral ciprofloxacin.
The case underscores the need for microbiological confirmation and tailored antibiotic treatment in atypical MOE cases.
Abstract
Malignant otitis externa (MOE) is a severe and potentially life-threatening infection of the external auditory canal, most frequently caused by Pseudomonas aeruginosa. Although typically seen in immunocompromised individuals—especially those with diabetes mellitus—up to 45% of cases have been reported in non-diabetic patients, highlighting the importance of recognizing atypical presentations. Rare pathogens, such as Proteus mirabilis, have been identified in only a few documented cases. Early diagnosis and prompt intervention are essential to prevent serious complications, including osteomyelitis and intracranial extension. This report describes a really uncommon case of malignant otitis externa caused by P. mirabilis in a non-diabetic, immunocompetent patient. A 53-year-old male with no relevant medical history presented with a four-month history of left-sided otorrhea, otalgia, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
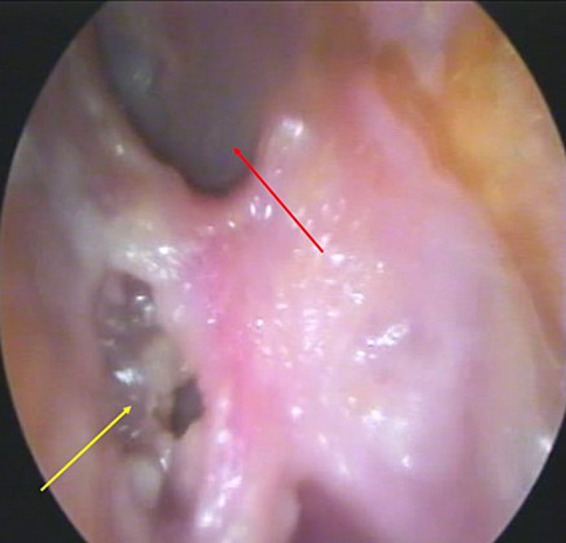 Figure 1
Figure 1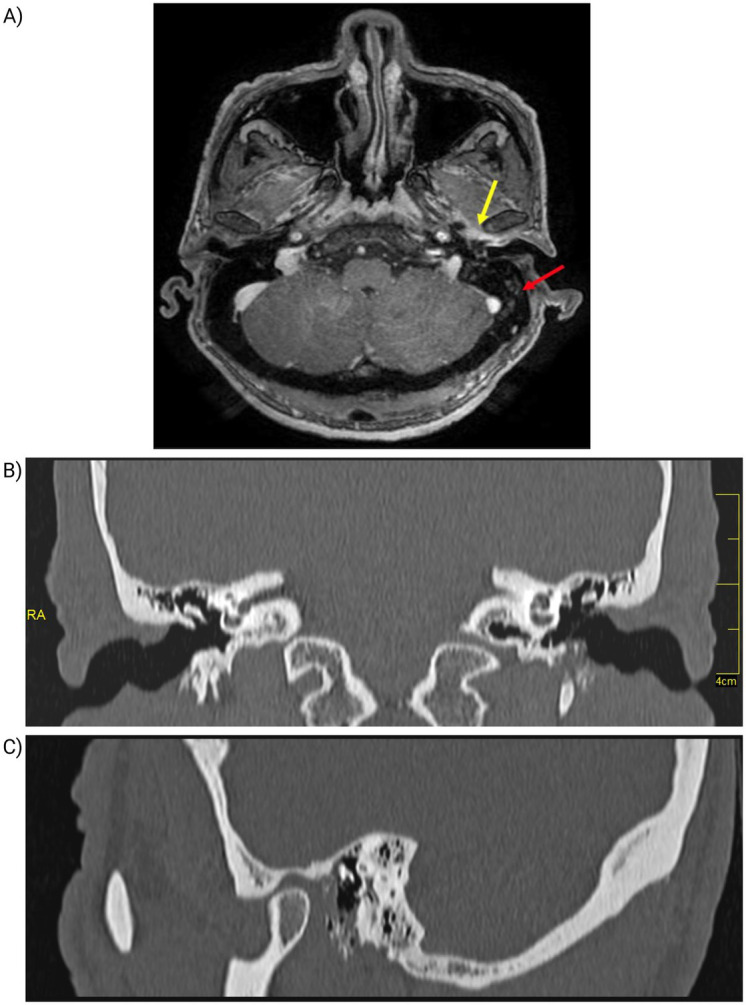 Figure 2
Figure 2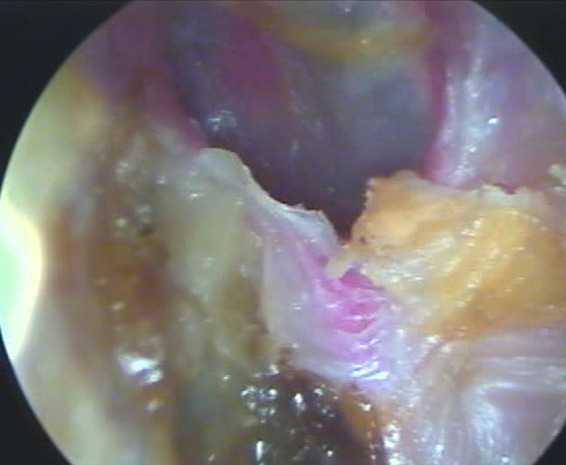 Figure 3
Figure 3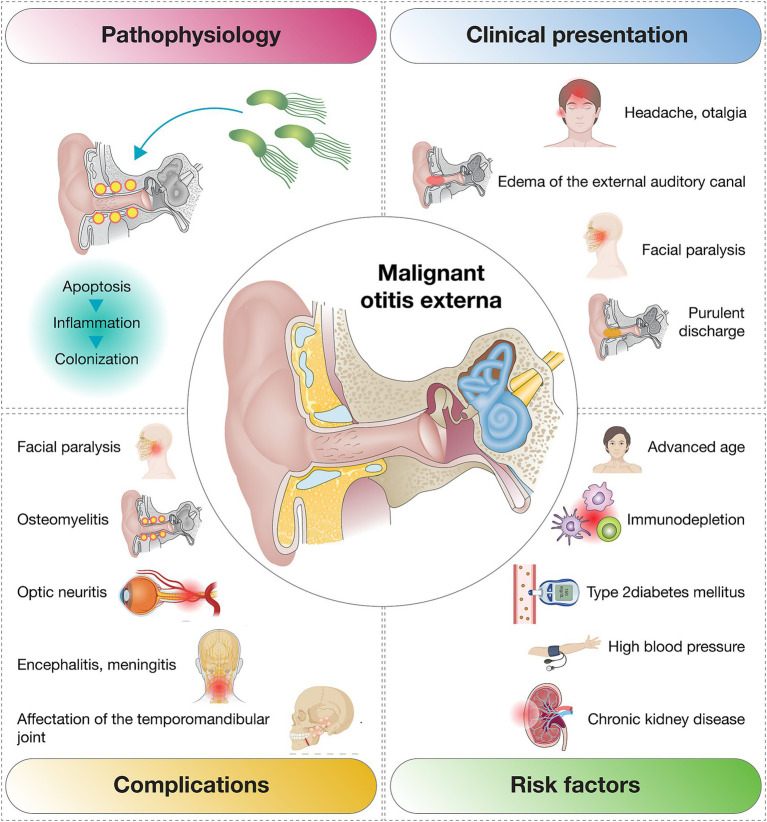 Figure 4
Figure 4| Parameter | Result | Reference value |
|---|---|---|
| Complete blood count | ||
| Hematocrit | 42.9% | M: 42–52%, W: 37–47% |
| Hemoglobin | 14.7 g/dL | M: 14–16, W: 12–14 mg/dL |
| Platelets | 315,000 cells/μl | 150,000–450,000 cells/uL |
| Leukocytes | 20,050 cells/μl | 3,600–10,500 cells/uL |
| Neutrophils | 17,240 cells/μl | 1,500–8,500 cells/μl |
| Lymphocytes | 2,205 cells/μl | 1,000–4,500 cells/μl |
| Biochemistry and serology | ||
| Glucose | 91 mg/dl | 70–110 mg/dL |
| Creatinine | 0.98 mg/dL | 0,70–1,30 mg/dL |
| C-reactive protein | 2.4 | 0,0 – 2,0 |
| VDRL (Syphilis Test) | Non-reactive | |
| HIV | Non-reactive | |
| Blood culture | Negative | |
| Otic secretion culture | ||
| Observation | Scant leukocytes and erythrocytes | |
| Bacterial culture | ||
| Fungal culture | Negative | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEar Surgery and Otitis Media · Sinusitis and nasal conditions · Streptococcal Infections and Treatments
Introduction
1
Malignant otitis externa (MOE) is a severe and potentially life-threatening infection of the external auditory canal that extends beyond the cutaneous lining, beginning as cellulitis and potentially progressing to chondritis, periostitis, or osteomyelitis. The condition is most commonly caused by Pseudomonas aeruginosa and can spread to adjacent soft tissues or even intracranial structures in advanced stages (1, 2). Although MOE is rare, its incidence has increased in at-risk populations—particularly among immunocompromised individuals—with diabetes mellitus reported in approximately 55–95% of cases (2–4).
The clinical presentation of MOE includes intense otalgia, headache, purulent discharge, and edema of the external auditory canal. Facial paralysis, often involving the facial nerve, is a frequent complication and underscores the importance of early diagnosis and timely treatment to prevent progression to severe outcomes such as osteomyelitis and meningitis (5, 6).
Recent studies have reported a rising incidence of MOE in non-diabetic individuals, accounting for 5 to 15% of all cases. For instance, Sideris et al. (7) found that approximately 11% of EOM cases occurred in patients without diabetes, highlighting other possible risk factors such as immunosuppression or foreign body exposure (7, 8). Other large-scale epidemiological studies from the United States and Taiwan have documented even higher proportions, with up to 45% of MOE cases occurring in non-diabetic patients, although diabetes remains strongly associated with MOE (OR = 7.50; 95% CI: 6.22–9.03) (3, 9).
Proteus mirabilis, a Gram-negative bacillus commonly associated with urinary tract and wound infections, is an infrequent but noteworthy pathogen in MOE. Compared to Pseudomonas aeruginosa, it has been less documented in this context. A study by Arsovic et al. (10) identified Proteus mirabilis in only one out of 30 positive cultures from MOE patients, underscoring its rarity and emerging clinical significance (11).
This report describes a really uncommon case of malignant otitis externa caused by Proteus mirabilis in a non-diabetic patient.
Case presentation
2
A 53-year-old male presented with a progressive four-month history of left-sided otorrhea, otalgia, and retro- and preauricular pain. He had no significant past medical history, including no diagnosis of diabetes mellitus. Prior treatment with amoxicillin/clavulanic acid had yielded no clinical improvement.
Physical examination revealed signs of cutaneous infection and bone erosion involving the anteroinferior and inferior walls of the external auditory canal (EAC). Otoendoscopy showed abundant yellowish, foul-smelling otorrhea (Figure 1). Based on these findings, the patient was admitted with a presumptive diagnosis of MOE for further evaluation and intravenous therapy.
Otoendoscopy of the left ear. Showing bone erosion in the inferior wall of the external auditory canal (yellow arrow) with purulent otorrhea and an intact tympanic membrane (red arrow).
Initial laboratory investigations revealed leukocytosis of 20,050 cells/μL (reference: 3,600–10,500/μL) with 86% neutrophils, a normal blood glucose level of 91 mg/dL (reference: 70–110 mg/dL), and elevated C-reactive protein (CRP) at 2.4 mg/dL (reference: 0.0–2.0 mg/dL). Serological tests for VDRL and HIV were non-reactive, and blood cultures were negative. Culture of the ear secretion identified Proteus mirabilis, resistant to ampicillin, ampicillin/sulbactam, cefazolin, and TMP-SMX but sensitive to azithromycin, cefotaxime, ciprofloxacin, imipenem, meropenem, and piperacillin/tazobactam. Fungal culture was negative (Table 1).
On the third day of hospitalization, magnetic resonance imaging (MRI) was performed, revealing mastoid cell occupation on the left side, with signal intensity alterations along the lower border of the EAC. A 13 mm × 9 mm fluid-filled lesion in the inner third of the EAC demonstrated peripheral enhancement following gadolinium administration (Figure 2A). As part of the diagnostic workup, a computed tomography (CT) scan was also obtained, confirming soft tissue density in the anteroinferior wall of the EAC, with associated bone erosion—consistent with damage to the underlying bony structures of the anteroinferior EAC wall (Figures 2B,C).
Imaging findings of the left ear. (A) Magnetic resonance imaging (MRI) of the left ear. Demonstrating opacification of the mastoid air cells (red arrow) and altered signal intensity at the inferior margin of the external auditory canal (yellow arrow). (B,C) Computed Tomography of the Left Ear. (B) Coronal CT scan shows bone erosion in the anteroinferior and inferior walls of the external auditory canal (red arrow). (C) CT scan shows soft tissue density with bone involvement (yellow arrow).
Based on culture sensitivity results, intravenous piperacillin/tazobactam (4.5 g every 6 h) was initiated, along with analgesics and anti-inflammatory agents including dexamethasone, diclofenac, and paracetamol. Multiple aspirations of purulent material were performed during hospitalization, revealing granulation tissue and necrotic debris, which were debrided.
After 7 days of treatment, leukocyte counts declined to 11,700 cells/μL, with normalization of neutrophil levels. Liver and metabolic function tests remained within normal ranges. The patient continued intravenous piperacillin/tazobactam throughout his 17-day hospital stay, showing consistent clinical improvement. At discharge (day 17), he was transitioned to oral ciprofloxacin (500 mg every 12 h) and omeprazole (20 mg daily) to complete a three-month antibiotic regimen. Outpatient follow-up was scheduled biweekly for the first 2 months and monthly thereafter for a total of 6 months.
At the three-month follow-up, the patient demonstrated substantial clinical improvement. Repeat otoendoscopy showed near-complete resolution of the infection (Figure 3). Long-term monitoring remains ongoing to ensure full recovery and prevent recurrence. This case report was prepared in accordance with the CARE (CAse REport) guidelines to ensure transparency and completeness in clinical case reporting.
Follow-up otoendoscopy of the left ear. The image shows a dry ear without purulent discharge, cerumen production, and an intact tympanic membrane.
Discussion
3
MOE is a severe infection of the external auditory canal that primarily affects elderly and immunocompromised individuals, with diabetes mellitus being the most common underlying condition associated with its development (7). This case emphasizes the importance of early diagnosis and appropriate treatment, even in atypical presentations. Notably, the patient in this report had no underlying comorbidities, such as diabetes mellitus or other immunosuppressive states (2, 12, 13) (Figure 4).
Overview of the most frequent clinical presentations, complications, and risk factors associated with malignant otitis externa.
In this case, the clinical presentation included otalgia and otorrhea in the absence of systemic symptoms, aside from leukocytosis noted on admission. This highlights the need for high clinical suspicion and timely diagnostic intervention to prevent the aggressive progression often seen in MOE (14). The patient presented with persistent, severe otalgia, purulent otorrhea, inflammation of the external auditory canal, and bone necrosis, as confirmed by otoscopic and imaging findings. Both CT and MRI were performed to confirm the diagnosis and assess the extent of bony involvement. Additional diagnostic modalities, such as bone scintigraphy, can also be considered to evaluate skull base involvement when needed (15).
Moreover, inflammatory biomarkers such as the erythrocyte sedimentation rate (ESR) may serve as useful adjuncts in the diagnosis and monitoring of MOE (16). Although ESR was not measured in this case, its inclusion is supported by literature, particularly in patients with suspected systemic inflammatory responses or advanced disease. Future case series and clinical guidelines should consider incorporating ESR as part of the standard diagnostic workup for MOE.
The clinical and radiological features in this case met the major and minor diagnostic criteria proposed by Cohen and Friedman in 1987, reaffirming the enduring relevance of these criteria, especially in resource-limited settings (15).
Given the initial clinical and imaging findings, carcinoma of the external auditory canal was considered as a differential diagnosis. This was based on the lesion’s appearance and imaging characteristics, which raised suspicion for a malignant process. Although no biopsy was performed, the absence of suspicious masses on imaging, the lack of progressive lesion growth, and the favorable response to targeted antibiotic therapy supported a non-neoplastic etiology. Culture of the ear discharge revealed a predominant inflammatory process with no evidence of malignancy, thereby excluding carcinoma and redirecting management toward MOE (10, 15).
The clinical manifestations observed in this case align with those reported by Arsovic et al. (10), who identified otalgia (76%), otorrhea (79%), external auditory canal edema (45%), and granulation tissue (31%) as the primary symptoms among 30 MOE patients. Such consistency underscores the importance of recognizing these hallmark symptoms in clinical practice.
Identification of the causative pathogen is critical for achieving favorable outcomes in MOE. While Pseudomonas aeruginosa is implicated in over 95% of cases, Aspergillus accounts for a smaller proportion (11). However, rare pathogens like Proteus mirabilis have been documented in isolated cases. For instance, Arsovic et al. (10) reported P. mirabilis in only one out of 30 MOE cases, a finding corroborated by AlSharhan et al. (17), who identified P. mirabilis as the causative agent in just one of 28 patients with otogenic skull base osteomyelitis. The identification of P. mirabilis in this patient highlights the need to consider uncommon pathogens in MOE, particularly in atypical presentations or non-immunosuppressed patients.
Antimicrobial resistance presents an increasing challenge in the management of MOE, underscoring the necessity of obtaining cultures and antibiotic susceptibility testing to guide treatment (18). In this case, the P. mirabilis was resistant to several agents, including ampicillin (a resistance rate reported in 10–20% of isolates), but was sensitivity to piperacillin-tazobactam, ciprofloxacin, and other agents, allowing targeted treatment. Multidisciplinary management, involving otorhinolaryngologists and infectious disease specialists, proved instrumental in achieving a favorable outcome (19). Intravenous piperacillin-tazobactam combined with serial aspiration of purulent discharge successfully controlled the infection, consistent with literature advocating aggressive antibiotic therapy to prevent complications such as sepsis or temporal bone osteomyelitis (17, 20). Additional interventions, such as surgical debridement or hyperbaric oxygen therapy, are typically reserved for refractory cases or poor responses to medical treatment (21–23).
This case broadens the diagnostic and therapeutic understanding of MOE, particularly in non-immunosuppressed patients. It underscores the importance of continuing education for healthcare professionals to improve awareness of MOE, including its risk factors, clinical presentation, and management strategies in atypical scenarios. Enhanced awareness could improve early diagnosis, guide tailored treatment, and ultimately lead to better outcomes for affected patients.
Conclusion
4
This case report describes an exceptionally rare instance of MEO caused by P. mirabilis in a non-immunocompromised patient, broadening the understanding of the clinical spectrum and etiological diversity of this condition. It underscores the need to consider atypical pathogens in cases where traditional risk factors, such as diabetes mellitus or immunosuppression, are absent.
The favorable outcome in this patient highlights the pivotal role of early diagnosis, thorough microbiological evaluation, and tailored antibiotic therapy in the successful management of MEO. The infection was effectively controlled through the use of broad-spectrum antibiotics, selected based on culture and sensitivity testing, combined with supportive interventions such as serial aspiration of purulent secretions. This case emphasizes the importance of a comprehensive and individualized approach to managing this potentially life-threatening condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sando I Harada T Okano Y Saito R Caparosa RJ. Temporal bone histopathology of necrotizing external otitis. A case report. Ann Otol Rhinol Laryngol. (1981) 90:109–15. doi: 10.1177/0003489481090002037224508 · doi ↗ · pubmed ↗
- 2Treviño González JL Reyes Suárez LL Hernández de León JE. Malignant otitis externa: an updated review. Am J Otolaryngol. (2021) 42:102894. doi: 10.1016/j.amjoto.2020.10289433429178 · doi ↗ · pubmed ↗
- 3Yang T-H Xirasagar S Cheng Y-F Wu C-S Kao Y-W Shia B-C. Malignant otitis externa is associated with diabetes: a population-based case-control study. Ann Otol Rhinol Laryngol. (2020) 129:585–90. doi: 10.1177/000348941990113931976744 · doi ↗ · pubmed ↗
- 4Hodgson SH Sinclair VJ Arwyn-Jones J Oh K Nucken K Perenyei M. Characteristics, management and outcome of a large necrotising otitis externa case series: need for standardised case definition. J Laryngol Otol. (2022) 136:604–10. doi: 10.1017/S 002221512100462 X 35042578 PMC 9257435 · doi ↗ · pubmed ↗
- 5Di Lullo AM Russo C Piroli P Petti A Capriglione P Cantone E. Malignant otitis external: our experience and literature review. Am J Case Rep. (2020) 21:e 925060. doi: 10.12659/AJCR.92506032808601 PMC 7458700 · doi ↗ · pubmed ↗
- 6Mahdyoun P Pulcini C Gahide I Raffaelli C Savoldelli C Castillo L. Necrotizing otitis externa: a systematic review. Otol Neurotol. (2013) 34:620–9. doi: 10.1097/MAO.0b 013e 3182804 aee 23598690 · doi ↗ · pubmed ↗
- 7Sideris G Latzonis J Avgeri C Malamas V Delides A Nikolopoulos T. A different era for malignant otitis externa: the non-diabetic and non-immunocompromised patients. J Int Adv Otol. (2022) 18:20–4. doi: 10.5152/iao.2022.2131335193841 PMC 9449702 · doi ↗ · pubmed ↗
- 8Glikson E Sagiv D Wolf M Shapira Y. Necrotizing otitis externa: diagnosis, treatment, and outcome in a case series. Diagn Microbiol Infect Dis. (2017) 87:74–8. doi: 10.1016/j.diagmicrobio.2016.10.01727806892 · doi ↗ · pubmed ↗