Endoscopic resection of an extraluminal esophageal duplication cyst
Shaimaa Elkholy, Mohamed El-Sherbiny, Hussein Hassan Okasha, Abeer Abdallatef, Hany Haggag, Mohamed Abdel Zaher, Karim Essam

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
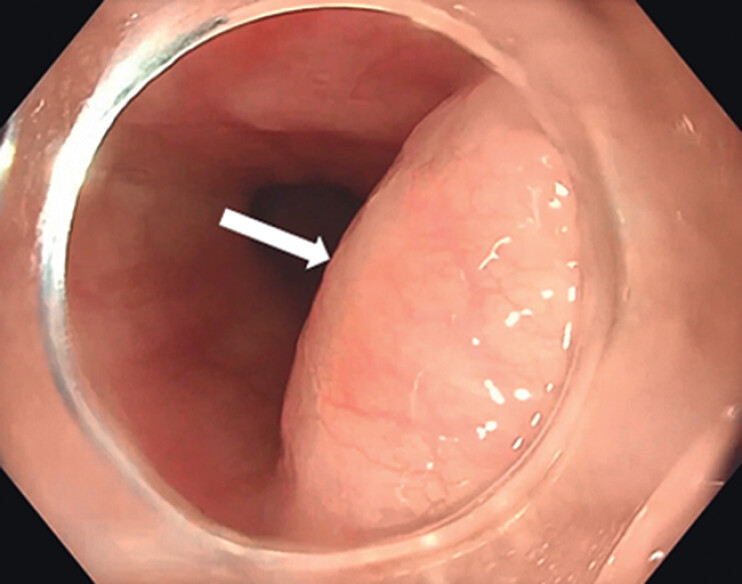 Fig. 1
Fig. 1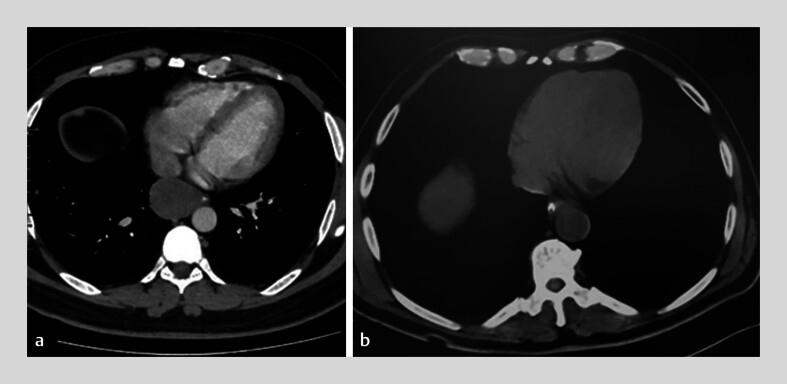 Fig. 2
Fig. 2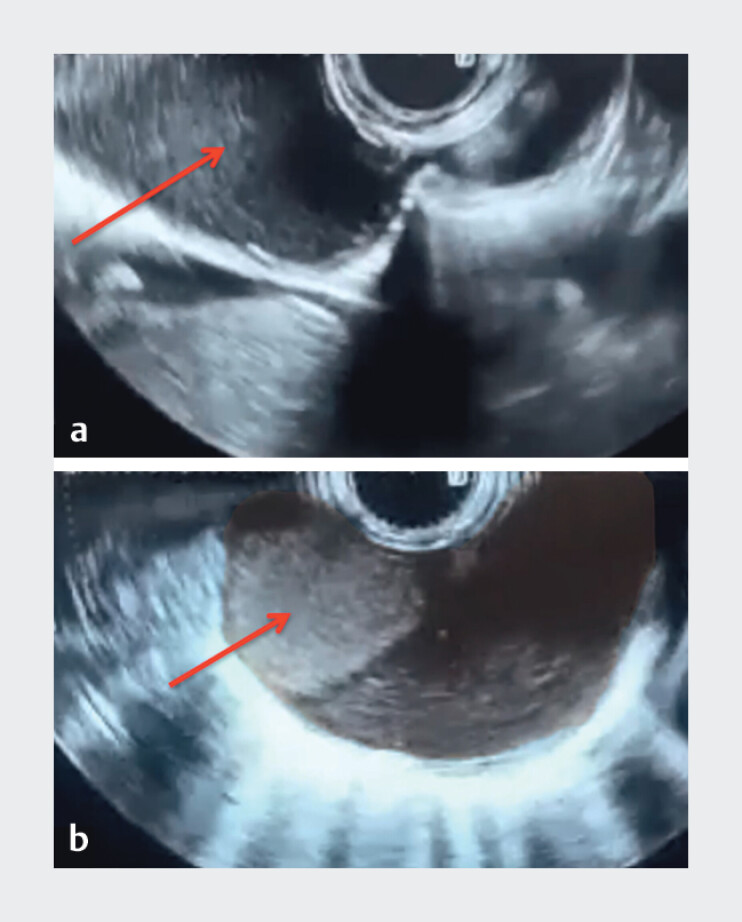 Fig. 3
Fig. 3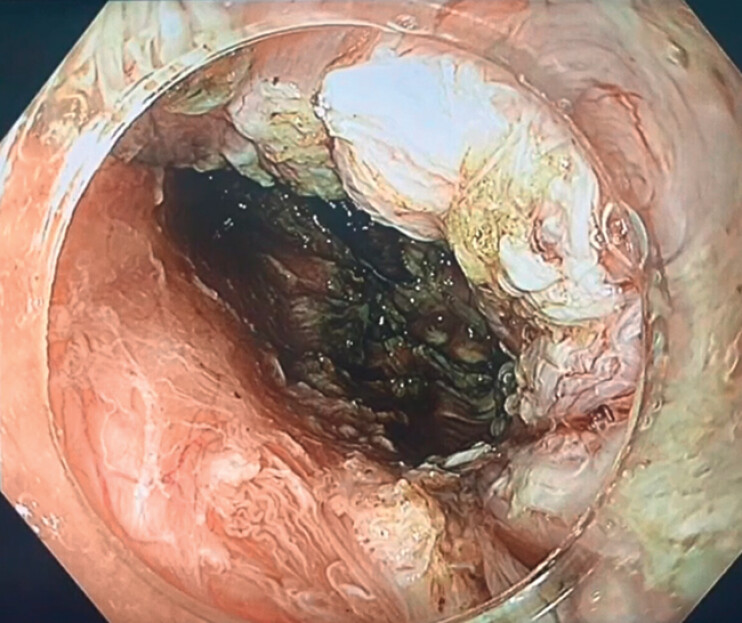 Fig. 4
Fig. 4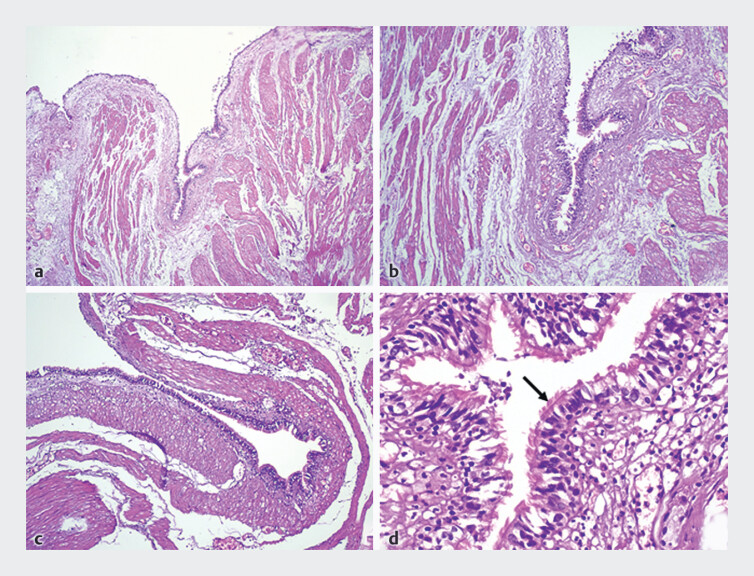 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Esophageal and GI Pathology
Esophageal duplication cysts are rare congenital anomalies, occasionally presenting in adults with dysphagia 1 . A 32-year-old man presented with progressive dysphagia. Upper endoscopy revealed a subepithelial bulge in the distal esophagus ( Fig. 1 ). A computed tomography (CT) scan showed a well-defined, homogeneous soft-tissue mass causing extrinsic compression of the esophageal lumen. The lesion was initially interpreted radiologically as an esophageal leiomyoma ( Fig. 2 a ). Endoscopic ultrasound demonstrated a well-defined cystic lesion (25 × 47 mm) at 35 cm from the dental arch, with posterior acoustic enhancement, no mural nodules or vascularity, and multiple wall layers containing echogenic content, suggestive of a duplication cyst 1 2 ( Fig. 3 ).
Upper endoscopy showing a subepithelial bulge (white arrow) in the lower esophagus.
a Axial contrast-enhanced computed tomography (CT) scan showing a well-defined, homogeneous soft-tissue mass causing extrinsic compression of the esophageal lumen. The lesion was initially interpreted radiologically as an esophageal leiomyoma. Subsequent endoscopic and histopathological evaluations confirmed the diagnosis of an esophageal duplication cyst. b Follow-up CT scan demonstrating complete resection of the cyst with resolution of the esophageal compression.
a Endoscopic ultrasound (EUS) image demonstrating a well-defined extraluminal cystic lesion (red arrow) causing a bulge in the lower esophageal wall. b EUS with color Doppler revealing a cystic lesion with posterior acoustic enhancement and absence of internal vascularity. The red arrow highlights a soft tissue component with a horizontal upper margin and no Doppler flow, suggestive of echogenic fluid layering in the dependent portion – likely representing sludge or proteinaceous material.
After multidisciplinary team consultation, submucosal tunnel endoscopic resection (STER) was selected as the preferred minimally invasive approach 3 . A submucosal tunnel was created following submucosal injection and mucosal incision. As dissection progressed, the cyst was seen bulging into the tunnel lumen ( Video 1 ). Shortly thereafter, the cyst was unintentionally punctured, releasing mucoid contents. Suction was applied, and the cyst wall was completely dissected and removed ( Fig. 4 ). The procedure used an Olympus X1 endoscope (GIF-H1500; Olympus Corp., Tokyo, Japan), a HybridKnife (ERBE, Tübingen, Germany), an ITknife (Olympus Corp., Tokyo, Japan), and an ERBE Vio 3 (Endocut Q 3,3,3; precise SECT coagulation 4.5).
Demonstration of submucosal tunnel endoscopic resection for a symptomatic esophageal duplication cyst in a 32-year-old man and six-month follow-up endoscopy.Video 1
Endoscopic view of the submucosal tunnel bed following complete resection of the cyst.
Histopathology confirmed an esophageal duplication cyst lined with pseudostratified ciliated columnar epithelium and surrounded by smooth muscle layers – consistent with an enteric-type duplication cyst 1 ( Fig. 5 ). Follow-up CT showed complete cyst resection ( Fig. 2 b ), and an upper endoscopy after six months revealed a scar at the previous entry site with complete resolution of the esophageal bulge ( Video 1 ).
Histopathological examination revealing a cyst wall lined by pseudostratified ciliated columnar epithelium (arrow), overlying a thin fibrous stroma and surrounded by smooth muscle fibers that merge with the muscularis propria. Hematoxylin and eosin (H&E) stain – Original magnifications: ×40, ×40, ×100, and ×400 (respectively).
This case demonstrates the utility of STER as a safe and effective organ-preserving approach for managing benign subepithelial esophageal lesions such as duplication cysts 2 3 4 and underscores the evolving capabilities of endoscopic resection in addressing even extraluminal pathology.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wahi JE Safdie FM Esophageal duplication cysts: a clinical practice review Mediastinum 20237110.21037/med-22-3336926292 PMC 10011867 · doi ↗ · pubmed ↗
- 2Sha H Jiang ZD Esophageal bronchogenic cyst treated with submucosal tunneling endoscopic resection: two case reports J Med Case Reports 20241813910.1186/s 13256-024-04453-y PMC 1098605338561839 · doi ↗ · pubmed ↗
- 3Chavan R Nabi Z Sud S Advanced endoscopic techniques for esophageal duplication cyst treatment: beyond surgery Video GIE 2025101710.1016/j.vgie.2025.03.00140496485 PMC 12146150 · doi ↗ · pubmed ↗
- 4Li Y Zhang Y Zhang J Esophageal bronchogenic cyst treated with submucosal tunneling endoscopic resection: two case reports World J Clin Cases 2020835335910.12998/wjcc.v 8.i 2.35332047785 PMC 7000942 · doi ↗ · pubmed ↗