Rescue therapy for recurrent cholangitis secondary to main duct intraductal papillary mucinous neoplasm with pancreatobiliary fistula using an esophageal fully covered metal stent
Anne Kimberly Lim-Fernandez, Samuel Jun Ming Lim, Christopher Jen Lock Khor, Damien Meng Yew Tan

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
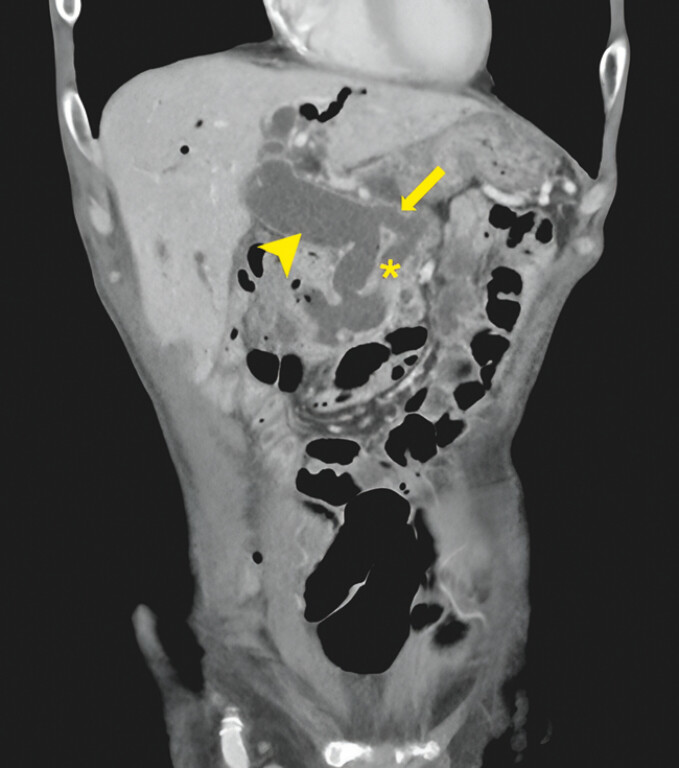 Fig. 1
Fig. 1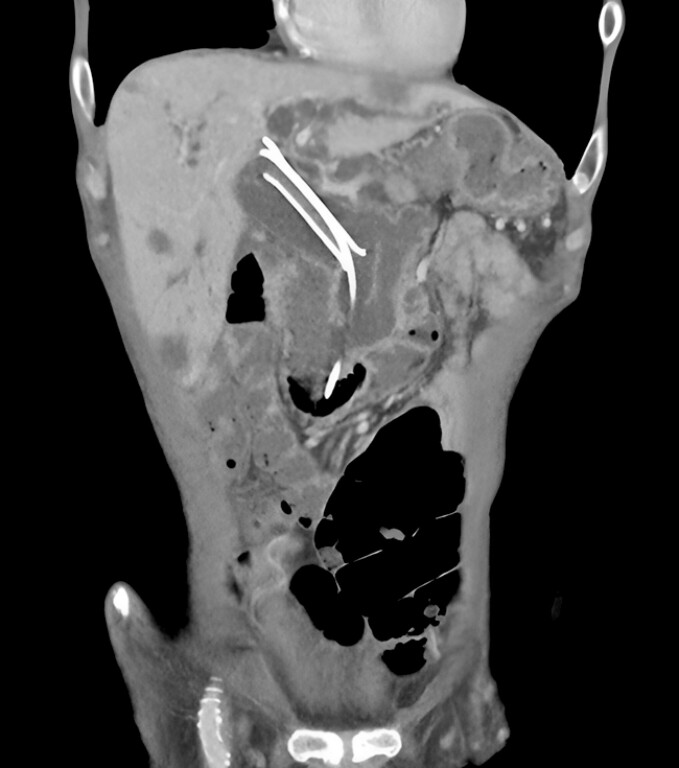 Fig. 2
Fig. 2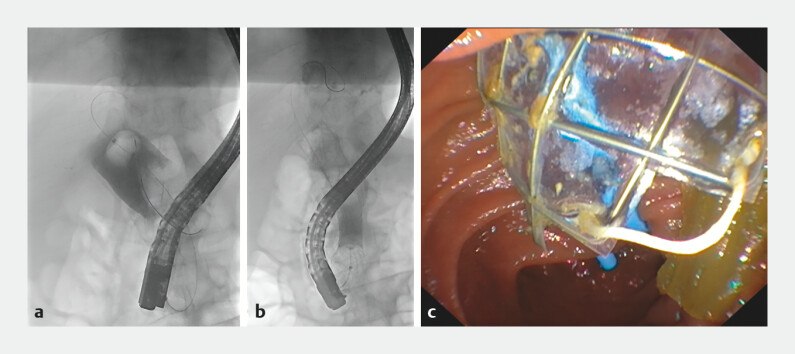 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Esophageal and GI Pathology · Gallbladder and Bile Duct Disorders
Main duct intraductal papillary mucinous neoplasms (MD-IPMNs) of the pancreas may be complicated by fistula formation 1 and biliary obstruction from excessive mucin 2 . Fistulation occurs in 6.6% of patients, involving organs like the common bile duct (CBD) 3 .
We present a 78-year-old man diagnosed with MD-IPMN who declined surgery and defaulted follow-up. Four years later, he presented with cholangitis. A computed tomography (CT) scan showed a 61 × 29-mm pancreatic mass with liver metastases and a 25-mm dilated CBD with fistulation between the main pancreatic duct and the mid-CBD ( Fig. 1 ). The patient underwent endoscopic retrograde cholangiopancreatography (ERCP) and insertion of a 10 × 60-mm biliary fully covered self-expanding metal stent (FCSEMS) (WallFlex; Boston Scientific, Marlborough, Massachusetts, USA) and a 7-Fr × 12-cm double-pigtail stent (Zimmon; Cook Medical, Bloomington, Indiana, USA) within the FCSEMS.
Main duct intraductal papillary mucinous neoplasm with pancreatobiliary fistula. Dilated common bile duct (arrowhead), dilated main pancreatic duct (asterisk), pancreatobiliary fistula (arrow).
He had initial clinical improvement but developed recurrent cholangitis two weeks later. A repeat CT scan showed proximal migration of the biliary FCSEMS ( Fig. 2 ). The use of an 18 × 97-mm through-the-scope esophageal FCSEMS (Agile; Boston Scientific) for repeat biliary stenting was considered because of its larger diameter. Informed consent was obtained from the patient after the off-label use with procedural risks, including perforation, was explained. Repeat ERCP was performed to remove the migrated biliary FCSEMS and double-pigtail stent, followed by balloon sweeps to remove excessive mucin within the 30-mm dilated CBD ( Video 1 ). The esophageal FCSEMS was successfully deployed in the CBD to close the pancreatobiliary fistula. A 7-Fr × 12-cm double-pigtail stent was then placed within the FCSEMS to prevent stent migration ( Fig. 3 ). The procedure lasted 45 minutes with no post-procedure complications. The patient recovered well and opted for the best supportive care.
Proximal migration of biliary fully covered self-expanding metal stent (FCSEMS).
Removal of migrated biliary fully covered self-expanding metal stent, extraction of large amount of mucin from a dilated common bile duct, followed by insertion of a through-the-scope esophageal fully covered self-expanding metal stent in the common bile duct.Video 1
a Dilated common bile duct with a 20-mm extraction balloon and excessive mucin within. b Occlusion cholangiogram after deployment of esophageal FCSEMS. c Endoscopic view of esophageal FCSEMS and biliary double-pigtail stent after placement.
Off-label use of esophageal FCSEMS may be considered for biliary stenting of a severely dilated CBD as smaller stents may be prone to migration.
Endoscopy_UCTN_Code_TTT_1AS_2AJ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shishido Y Mitsuoka E Ito R Fistula formation into other organs secondary to intraductal papillary mucinous neoplasm of the pancreas: A case report and literature review Medicine (Baltimore)2023102 e 3428810.1097/MD.0000000000034288 PMC 1032859737417614 · doi ↗ · pubmed ↗
- 2Patel A Lambiase L Decarli A Management of the mucin filled bile duct. A complication of intraductal papillary mucinous tumor of the pancreas JOP 2005625525915883476 · pubmed ↗
- 3Kobayashi G Fujita N Noda Y Intraductal papillary mucinous neoplasms of the pancreas showing fistula formation into other organs J Gastroenterol 2010451080108920549253 10.1007/s 00535-010-0263-z · doi ↗ · pubmed ↗