Diagnosis of reactive lymphoid hyperplasia of the bile duct observed on peroral video cholangioscopy
Nami Miyamoto, Masaya Iwamuro, Kiyoaki Ochi, Yosuke Saragai, Tsuneyoshi Ogawa, Toru Ueki

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
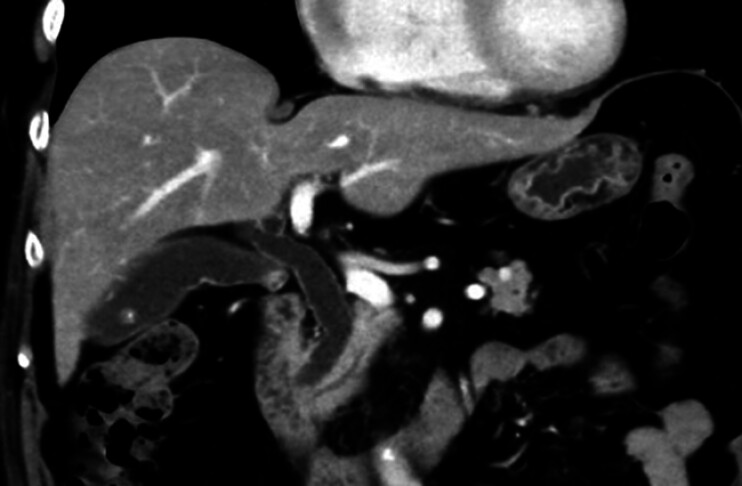 Fig. 1
Fig. 1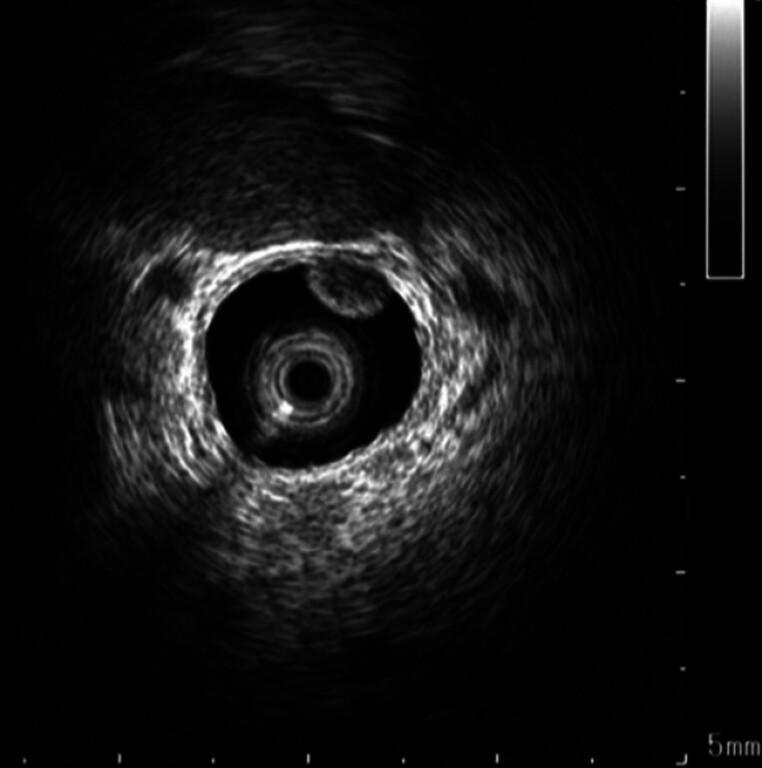 Fig. 2
Fig. 2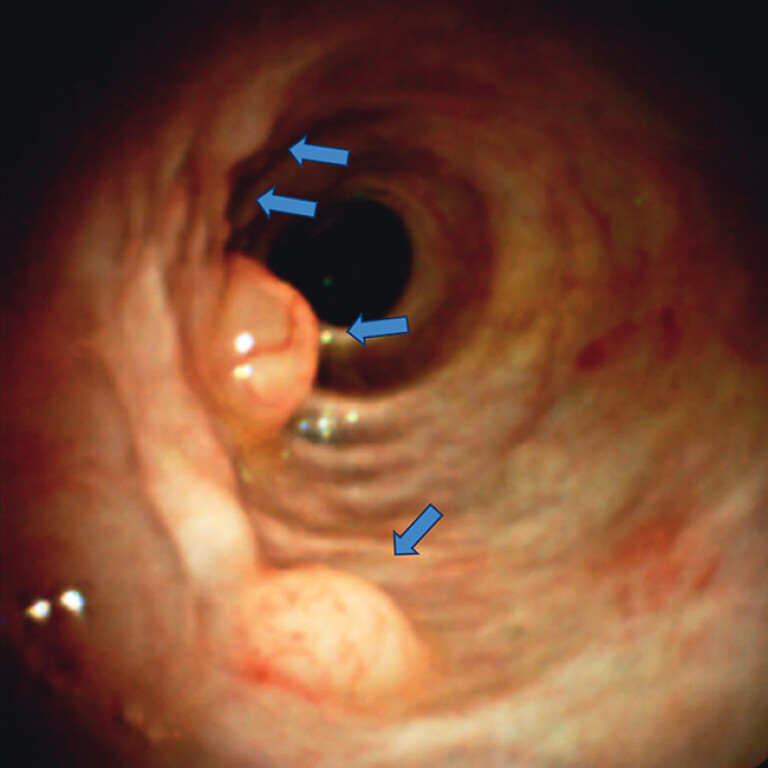 Fig. 3
Fig. 3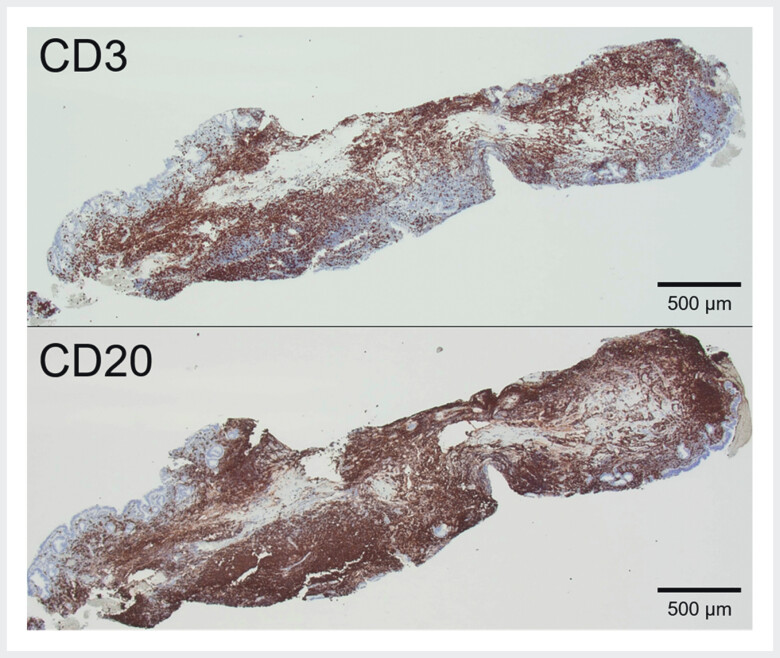 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Gastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment
A 74-year-old Japanese woman presented with epigastric discomfort and elevated gamma-glutamyl transpeptidase levels (76 U/L). Abdominal ultrasonography revealed gallstones and bile duct wall thickening, prompting referral to our hospital. Contrast-enhanced computed tomography confirmed common bile duct dilation and wall thickening ( Fig. 1 ), while magnetic resonance imaging revealed right hepatic duct dilation. Endoscopic ultrasonography detected hyperechoic areas in the common bile duct and gallbladder, suggesting stones or debris. Endoscopic retrograde cholangiopancreatography confirmed choledocholithiasis, and stones were removed. Intraductal ultrasound identified multiple hypoechoic, subepithelial lesion-like protrusions with hyperechoic margins in the right hepatic duct ( Fig. 2 ). Peroral cholangioscopy under carbon dioxide (CO 2 ) insufflation revealed multiple subepithelial lesions with dilated surface vasculature ( Fig. 3 , Video 1 ). Furthermore, forceps biopsy demonstrated intact mucosa with lymphoid hyperplasia, without neoplastic changes. Subsequent immunohistochemical staining detected mixed CD20 and CD3 expression, prompting a diagnosis of reactive lymphoid hyperplasia (RLH) ( Fig. 4 ). No specific treatment was pursued for the biliary RLH. Laparoscopic cholecystectomy was performed to address symptomatic gallstones; however, RLH was absent in the resected gallbladder.
Contrast-enhanced computed tomography showed common bile duct dilation and mild wall thickening.
Intraductal ultrasound showed multiple hypoechoic, subepithelial lesion-like protrusions with hyperechoic margins in the right hepatic duct.
Peroral cholangioscopy revealed multiple subepithelial lesions (arrows) with dilated vasculature on the surface.
Immunohistochemistry staining showed a clear distinction between CD3, which is positive in T-cell lymphoma, whereas CD20 is positive in B-cell lymphoma, leading to the exclusion of malignant lymphomas other than follicular lymphoma.
Peroral cholangioscopy under carbon dioxide insufflation. Reactive lymphoid hyperplasia appeared as multiple subepithelial lesions with dilated surface vasculature on cholangioscopy.Video 1
Biliary RLH is rare and is believed to be associated with inflammatory conditions such as cholelithiasis and cholangitis, as well as malignancies. To our knowledge, only three cases of biliary RLH have been reported 1 2 3 . Among them, peroral cholangioscopy was performed in two cases using saline irrigation, revealing villous and granular lesions in one case 1 and a polypoid lesion in the other 3 . In contrast, our case exhibited submucosal tumor-like protrusions with dilated vasculature, a finding that is distinct from those previously reported. CO 2 replacement may have contributed to clearer visualization of the polypoid lesion, consistent with previous studies that indicated superior imaging performance with CO 2 compared with saline irrigation 4 . This case highlights the utility of peroral cholangioscopy with direct biopsy for diagnosing challenging biliary lesions.
Endoscopy_UCTN_Code_CCL_1AZ_2AM
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Matsumoto K Kato H Okada H Lymphoid hyperplasia of the bile duct observed on peroral video cholangioscopy Clin Gastroenterol Hepatol 201614 e 127e 12810.1016/j.cgh.2016.05.00127165467 · doi ↗ · pubmed ↗
- 2Miyamoto K Matsumoto K Matsubara Klymphoid hyperplasia of the gallbladder extending to the bile duct Intern Med 2023621293129810.2169/internalmedicine.0365-2236130889 PMC 10208782 · doi ↗ · pubmed ↗
- 3Muro S Kato H Fushimi HA case of polypoid lesions of the common bile duct observed on peroral video cholangioscopy Dig Liver Dis 20164845310.1016/j.dld.2015.12.01026775095 · doi ↗ · pubmed ↗
- 4Toru U Mizuno M Ota S Carbon dioxide insufflation is useful for obtaining clear images of the bile duct during peroral cholangioscopy (with video)Gastrointest Endosc 2010711046105120438891 10.1016/j.gie.2010.01.015 · doi ↗ · pubmed ↗