The hidden danger behind a normal endoscopy: successful endoscopic full-thickness resection guided by endoscopic ultrasound
Rui Zhong, Yufang Wang, Kui Zhao

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1 Fig. 2
Fig. 2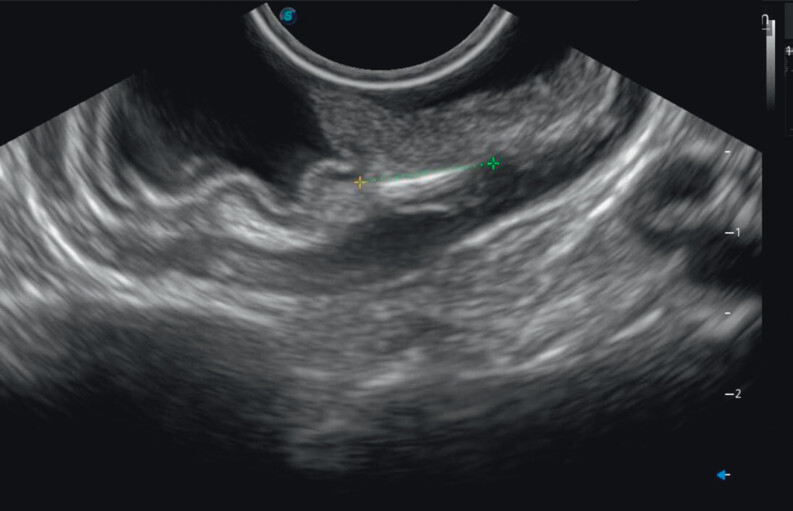 Fig. 3
Fig. 3 Fig. 4
Fig. 4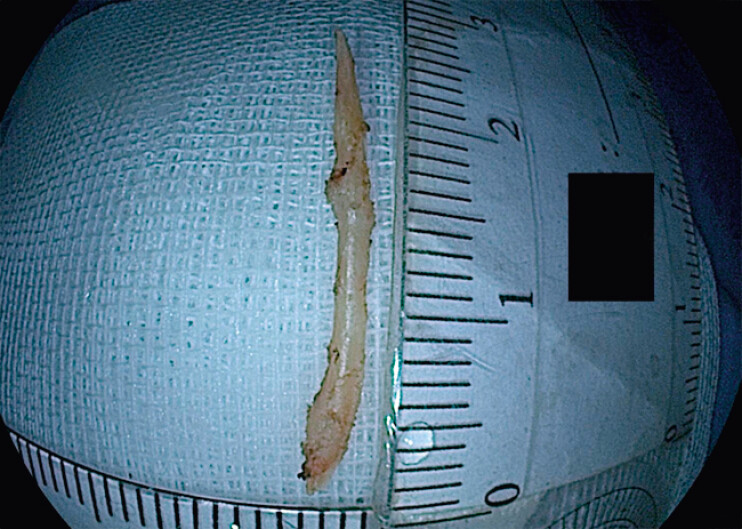 Fig. 5
Fig. 5- —Project of “CMC Talents” Peak Plan of Chengdu Medical College
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Metastasis and carcinoma case studies · Gastrointestinal Tumor Research and Treatment
A 38-year-old man underwent abdominal computed tomography (CT) during routine health screening, which revealed a linear hyperdense structure near the lesser curvature of the gastric antrum ( Fig. 1 ). He recalled ingesting a fish bone 2 months earlier but experienced no significant discomfort at the time and did not seek medical attention. Initial upper endoscopy showed no mucosal abnormalities ( Fig. 2 ). Endoscopic ultrasound (EUS) localized the foreign body within the deep muscularis propria ( Fig. 3 ). EUS-guided methylene blue injection and titanium clip placement were performed to guide endoscopic submucosal dissection, exposing the muscularis layer. Despite adequate dissection, the fish bone remained invisible, likely due to chronic inflammation and fibrosis resulting in transmural incorporation and concealment ( Fig. 4 ). Real-time EUS was re-employed for precise re-localization, followed by a deeper incision. The foreign body was tightly adherent to the gastric wall and could not be removed with forceps. A snare was used to anchor and provide countertraction, while a mucosal incision knife facilitated meticulous dissection of the fibrotic base. This coordinated traction–dissection approach enabled successful full-thickness endoscopic resection, retrieving a 3-cm fish bone ( Fig. 5 ). The defect was closed with titanium clips ( Video 1 ). This case highlights that fish bone ingestion warrants careful evaluation even where endoscopy findings are normal; additional imaging such as CT and the dynamic benefits of EUS play crucial roles.
Abdominal computed tomogram showing a linear hyperdense foreign body adjacent to the lesser curvature of the gastric antrum.
Initial upper endoscopic image showing no visible mucosal abnormalities.
Endoscopic ultrasonogram identifying the location and depth of the fish bone within the muscularis propria.
Chronic inflammation and fibrosis suggesting transmural incorporation of the fish bone into the gastric wall.
Retrieved fish bone, measuring approximately 3 cm in length.
Successful endoscopic full-thickness resection, guided by endoscopic ultrasound, of a fish bone undetected by endoscopy.Video 1
Endoscopy_UCTN_Code_TTT_1AO_2AL