Work-Related Musculoskeletal Disorders and Quality of Life in Nursing Personnel Across Northwestern Greece
Nikolaos Sontis, Anastasios Korompilias, Aimilios Pakos, Ioannis Gkiatas, Ioannis D Gelalis

TL;DR
This study found that nearly half of nursing staff in northwestern Greece suffer from work-related musculoskeletal disorders, mainly in the lower back, which significantly lowers their physical quality of life.
Contribution
The study identifies specific nursing tasks and job factors that predict musculoskeletal disorders and their impact on physical quality of life.
Findings
49.5% of nursing personnel had work-related musculoskeletal disorders, with the lumbar spine most affected.
Moving patients and lifting heavy objects were strongly linked to musculoskeletal disorders.
Physical quality of life was significantly lower for those with disorders and for those with more years of experience.
Abstract
Introduction: Work-related musculoskeletal disorders (WrMSDs) among nursing personnel have been recognized as one of the most frequent musculoskeletal injuries. The aim of the present study was to estimate the incidence of WrMSDs in a sample of nursing personnel, identify predictors of WrMSDs, and examine their effects on quality of life (QoL). Methodology: A cross-sectional design was adopted, and participants were full-time nursing personnel at five hospitals in northwestern Greece. Data included demographics, the RAND Short Form health survey (RAND SF-36) to measure the physical (Physical Component Score, PCS) and mental (Mental Component Score, MCS) components of QoL, and the Nordic Musculoskeletal Questionnaire (NMQ) to assess WrMSDs. Data were analyzed descriptively to summarize main outcome measures, and linear models were used to estimate the effect of WrMSDs on QoL. Results:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
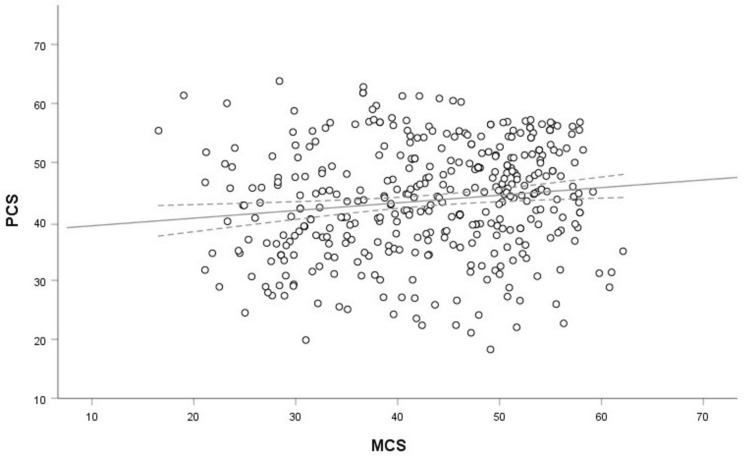 Figure 1
Figure 1| Variable | Values |
| Age, years | 47.2 (±8.0) |
| Weight, kg | 71.5 (±12.5) |
| Height, m | 1.67 (±0.07) |
| BMI, m·kg-2 | 25.7 (±3.9) |
| PCS | 43.5 (±9.2) |
| MCS | 43.1 (±9.8) |
| Gender | |
| Male | 52 (12.9%) |
| Female | 350 (87.1%) |
| Current position | |
| Nursing supervisor/assistant supervisor | 33 (8.2%) |
| Nurse | 218 (54.2%) |
| Nursing assistant | 143 (35.6%) |
| Midwife | 8 (2.0%) |
| Body type | |
| Lean | 4 (1.0%) |
| Normal | 268 (66.7%) |
| Overweight | 130 (32.3%) |
| Nursing seniority, years | |
| <5 | 36 (9.0%) |
| 5-9 | 24 (6.0%) |
| 10-14 | 35 (8.7%) |
| 15-20 | 58 (14.4%) |
| 20-24 | 81 (20.1%) |
| >25 | 168 (41.8%) |
| Diagnosis of WrMSD | |
| No | 203 (50.5%) |
| Yes | 199 (49.5%) |
| Anatomical site | n | % |
| Head and cervical spine | 140 | 34.8% |
| Shoulder | 97 | 24.1% |
| Humerus | 19 | 4.7% |
| Elbow | 37 | 9.2% |
| Forearm | 22 | 5.5% |
| Wrist | 96 | 23.9% |
| Hand | 43 | 10.7% |
| Lumbar spine | 223 | 55.5% |
| Hip | 50 | 12.4% |
| Knee | 89 | 22.1% |
| Gastrocnemius | 20 | 5.0% |
| Ankle joint | 52 | 12.9% |
| Foot | 26 | 6.5% |
| Variables | WrMSD (no, n=203) | WrMSD (yes, n=199) | Statistics | df | p-value |
| Hospital | |||||
| UHI | 83 (40.1%) | 124 (59.9%) | χ2=18.714 | 4 | <0.001 |
| GHI | 27 (58.7%) | 19 (41.3%) | |||
| GHP | 19 (61.3%) | 12 (38.7%) | |||
| GHA | 50 (63.3%) | 29 (36.7%) | |||
| GHF | 24 (61.5%) | 15 (38.5%) | |||
| Gender | |||||
| Male | 31 (59.6%) | 21 (40.4%) | χ2=1.986 | 1 | 0.159 |
| Female | 172 (49.1%) | 178 (50.9%) | |||
| Current position | |||||
| Nursing supervisor/assistant supervisor | 14 (42.4%) | 19 (57.6%) | χ2=2.235 | 3 | 0.525 |
| Nurse | 117 (53.7%) | 110 (46.3%) | |||
| Assistant nurse | 68 (47.6%) | 75 (52.4%) | |||
| Midwife | 4 (50.0%) | 4 (50.0%) | |||
| Nursing seniority | |||||
| <5 years | 29 (80.6%) | 7 (19.4%) | χ2=22.87 | 5 | <0.001 |
| 5-9 years | 14 (58.3%) | 10 (41.7%) | |||
| 10-14 years | 22 (62.9%) | 13 (37.1%) | |||
| 15-19 years | 31 (53.4%) | 27 (46.6%) | |||
| 20-24 years | 39 (48.1%) | 42 (51.9%) | |||
| 25+ years | 68 (40.5%) | 100 (59.5%) | |||
| BMI classification | |||||
| Normal | 98 (55.4%) | 79 (44.6%) | χ2=3.106 | 2 | 0.212 |
| Overweight | 79 (47.3%) | 88 (52.7%) | |||
| Obese | 26 (44.8%) | 32 (55.2%) |
| Variable | WrMSD (no, n=203) | WrMSD (yes, n=199) | Statistics | df | p-value |
| Patient transport via stretchers | |||||
| No | 137 (49.8%) | 138 (50.2%) | χ2=0.161 | 1 | 0.689 |
| Yes | 66 (52.0%) | 61 (48.0%) | |||
| Moving patients | |||||
| No | 92 (59.4%) | 63 (40.6%) | χ2=7.917 | 1 | 0.005 |
| Yes | 111 (44.9%) | 136 (55.1%) | |||
| Transporting material with a wheelbarrow | |||||
| No | 61 (62.2%) | 37 (37.8%) | χ2=7.154 | 1 | 0.007 |
| Yes | 142 (46.7%) | 162 (53.3%) | |||
| Transporting material w/o a wheelbarrow | |||||
| No | 69 (61.1%) | 44 (38.9%) | χ2=7.018 | 1 | 0.008 |
| Yes | 134 (46.4%) | 155 (53.6%) | |||
| Sorting material on high shelves | |||||
| No | 23 (65.7%) | 12 (34.3%) | χ2=3.551 | 1 | 0.060 |
| Yes | 180 (49.0%) | 187 (51.0%) | |||
| Sorting material on low shelves | |||||
| No | 23 (62.2%) | 14 (37.8%) | χ2=2.218 | 1 | 0.136 |
| Yes | 180 (49.3%) | 185 (50.7%) | |||
| Changing patient clothes | |||||
| No | 73 (56.6%) | 56 (43.4%) | χ2=2.820 | 1 | 0.093 |
| Yes | 130 (47.3%) | 143 (52.4%) | |||
| Bathing patients | |||||
| No | 114 (52.5%) | 103 (47.5%) | χ2=0.783 | 1 | 0.376 |
| Yes | 89 (48.1%) | 96 (51.9%) | |||
| Sedentary work (i.e., prolonged sitting) | |||||
| No | 79 (59.4%) | 54 (40.6%) | χ2=6.299 | 1 | 0.012 |
| Yes | 124 (46.1%) | 145 (53.9%) | |||
| Preparing patient regimes | |||||
| No | 57 (50.4%) | 56 (49.6%) | χ2=<0.001 | 1 | 0.989 |
| Yes | 146 (50.5%) | 143 (49.5%) | |||
| Executing patient regimes | |||||
| No | 55 (50.0%) | 55 (50.0%) | χ2=0.015 | 1 | 0.903 |
| Yes | 148 (50.7%) | 144 (49.3%) | |||
| Lifting/carrying objects from the ground | |||||
| No | 72 (64.9%) | 39 (35.1%) | χ2=12.662 | 1 | <0.001 |
| Yes | 131 (45.0%) | 160 (55.0%) | |||
| Lifting/carrying patients | |||||
| No | 78 (59.5%) | 53 (40.5%) | χ2=6.359 | 1 | 0.012 |
| Yes | 125 (46.1%) | 146 (53.9%) |
| Variable | WrMSD (no, n=203) | WrMSD (yes, n=199) | Statistics | df | p-value |
| Workplace spacing | |||||
| Spacious | 9 (60.0%) | 6 (40.0%) | χ2=0.763 | 3 | 0.858 |
| Adequate | 70 (50.7%) | 68 (49.3%) | |||
| Limited | 96 (50.5%) | 94 (49.5%) | |||
| Inadequate | 28 (47.5%) | 31 (52.5%) | |||
| Workplace distances | |||||
| Short | 37 (62.7%) | 22 (37.3%) | χ2=4.219 | 2 | 0.121 |
| Average | 116 (48.9%) | 121 (51.1%) | |||
| Long | 50 (47.2%) | 56 (52.8%) | |||
| Degree/intensity of prolonged standing | |||||
| High | 138 46.9%) | 156 (53.1%) | χ2=5.563 | 2 | 0.062 |
| Average | 58 (60.4%) | 38 (39.6%) | |||
| Low | 7 (58.3%) | 5 (41.7%) | |||
| Degree/intensity of prolonged walking | |||||
| High | 81 (51.6%) | 76 (48.4%) | χ2=1.930 | 2 | 0.381 |
| Average | 68 (54.0%) | 58 (46.0%) | |||
| Low | 54 (45.4%) | 65 (54.6%) | |||
| Prolonged inappropriate body position | |||||
| High | 83 (48.0%) | 90 (52.0%) | χ2=3.536 | 2 | 0.171 |
| Average | 71 (48.3%) | 76 (51.7%) | |||
| Low | 49 (59.8%) | 33 (40.2%) | |||
| Prolonged awkward body position | |||||
| High | 50 (41.3%) | 71 (58.7%) | χ2=5.856 | 2 | 0.053 |
| Average | 78 (54.9%) | 64 (45.1%) | |||
| Low | 75 (54.0%) | 64 (46.0%) | |||
| Prolonged bending | |||||
| High | 54 (45.4%) | 65 (54.6%) | χ2=1.994 | 2 | 0.369 |
| Average | 77 (51.3%) | 73 (48.7%) | |||
| Low | 72 (54.1%) | 61 (45.9%) | |||
| Prolonged hyperextension | |||||
| High | 35 (39.3%) | 54 (60.7%) | χ2=5.721 | 2 | 0.053 |
| Average | 66 (54.1%) | 56 (49.5%) | |||
| Low | 102 (53.4%) | 89 (46.6%) | |||
| Degree/intensity of heavy object lifting | |||||
| High | 38 (35.8%) | 68 (64.2%) | χ2=12.374 | 2 | 0.002 |
| Average | 68 (56.2%) | 53 (43.8%) | |||
| Low | 97 (55.4%) | 78 (44.6%) | |||
| Degree/intensity of moving heavy objects | |||||
| High | 46 (41.8%) | 64 (58.2%) | χ2=4.985 | 2 | 0.083 |
| Average | 64 (56.1%) | 50 (43.9%) | |||
| Low | 93 (52.2%) | 85 (47.8%) | |||
| Degree/intensity of moving patients from the bed | |||||
| High | 66 (42.9%) | 88 (57.1%) | χ2=5.895 | 2 | 0.052 |
| Average | 59 (56.2%) | 46 (43.8%) | |||
| Low | 78 (54.5%) | 65 (45.5%) | |||
| Degree/intensity of moving patients from/onto the stretcher | |||||
| High | 48 (42.5%) | 65 (57.5%) | χ2=6.160 | 2 | 0.046 |
| Average | 65 (59.1%) | 45 (40.9%) | |||
| Low | 90 (50.3%) | 89 (49.7%) | |||
| Degree/intensity of prolonged sitting | |||||
| High | 11 (40.7%) | 16 (59.3%) | χ2=1.442 | 2 | 0.486 |
| Average | 62 (53.4%) | 54 (46.6%) | |||
| Low | 130 (50.2%) | 129 (49.8%) | |||
| Duration of break | |||||
| No break | 37 (59.5%) | 47 (40.5%) | FE=10.141 | 5 | 0.071 |
| v≤5 min | 28 (48.3%) | 30 (51.7%) | |||
| 5-10 min | 73 (56.2%) | 57 (43.8%) | |||
| 10-15 min | 40 (47.1%) | 45 (52.9%) | |||
| 15-20 min | 16 (45.7%) | 19 (54.3%) | |||
| 20-30 min | 9 (90.0%) | 1 (10.0%) |
| Effect | Estimate | p-value |
| Intercept | 49.0 (46.0; 52.0) | <0.001 |
| WrMSD diagnosisyes | -5.7 (-7.4; -4.1) | <0.001 |
| Working experience5-9years | -1.3 (-5.6; 3.0) | 0.559 |
| Working experience10-14years | -2.5 (-6.3; 1.4) | 0.209 |
| Working experience15-19years | -3.2 (-6.6; 0.3) | 0.075 |
| Working experience20-24years | -5.9 (-9.1; -2.6) | <0.001 |
| Working experience>25years | -6.6 (-9.7; -3.5) | <0.001 |
| Positionmidwife | 2.5 (-3.5; 8.5) | 0.417 |
| Positionnurse | 3.1 (1.3; 4.9) | <0.001 |
| Positionsupervisor/ass. supervisor | 4.1 (0.9; 7.3) | 0.012 |
| F | 12.57 | <0.001 |
| RSE | 8.2 | n/a |
| R2 | 20.6 | n/a |
| Effect | Estimate | p-value |
| Intercept | 43.2 (41.0; 45.4) | <0.001 |
| Break duration5min | 1.3 (-2.0; 4.7) | 0.436 |
| Break duration10min | 0.6 (-2.1; 3.3) | 0.674 |
| Break duration15min | 1.3 (-1.7; 4.2) | 0.389 |
| Break duration20min | 4.3 (0.4; 8.2) | 0.032 |
| Break duration30min | 3.1 (-3.4; 9.5) | 0.351 |
| HospitalGHI | -2.1 (-5.2; 1.1) | 0.193 |
| HospitalGHA | -2.0 (-4.6; 0.6) | 0.133 |
| HospitalGHP | -0.7 [-4.4; 3.0] | 0.716 |
| HospitalGHF | -5.8 (-9.2; -2.3) | <0.001 |
| F | 3.189 | 0.038 |
| RSE | 9.7 | n/a |
| R2 | 4.0 | n/a |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Occupational health in dentistry · Ergonomics and Musculoskeletal Disorders
Introduction
Work-related musculoskeletal disorders (WrMSDs) have been recognized as one of the most frequent musculoskeletal injuries [1,2], and nursing personnel are characterized as a high-risk group for developing WrMSDs [3-5]. In addition, WrMSDs are considered one of the leading causes of occupational diseases and are associated with the development of chronic pain among healthcare professionals [6].
The anatomical site with the highest prevalence of WrMSDs among registered nurses is the spine, more specifically the lumbar (~60%) and cervical (~53%) spine, as well as the shoulder level (47%) [3,7]. In clinical practice, nursing personnel are frequently required to perform tasks that involve excessive flexion and rotation, such as moving and/or lifting objects above shoulder level and handling patients by moving, pulling, or pushing them to and from beds or other locations [8,9]. The reported high frequency of WrMSDs among nursing personnel can lead to workforce reductions, an increased number of sick days per year, and professional burnout [10-12]. In addition, WrMSDs negatively affect life outside the workplace by deteriorating quality of life (QoL) [13,14], although others report no impact [15].
The nature of WrMSDs is multifactorial. Obesity, age, years of employment, work tasks, number of weekly working hours, excessive night shifts, stress levels, job satisfaction, and exercise habits are considered risk factors for developing WrMSDs [2]. Unraveling the incidence of WrMSDs and its relationship with underlying factors among nursing personnel is a key step for health policy administrators to design and implement effective interventions for healthcare professionals [16]. Therefore, the aims of the present study were to document the incidence of WrMSDs in a sample of nursing personnel at five hospitals in a large region in northwestern Greece, identify demographic and other predictors, and examine their effect on QoL. We hypothesized that the incidence would be high (40-60%) and similar to previously reported data, and that diagnosis would be associated with reduced QoL.
Materials and methods
The study was approved by the Institutional Review Board of the University Hospital of Ioannina (UHI). Participants were fully informed of the voluntary nature of study participation. All data were anonymous and could be accessed only by the research team.
Nursing staff working in public hospitals of Epirus, namely, UHI, General Hospital of Ioannina "G. Hatzikosta" (GHI), General Hospital of Preveza (GHP), General Hospital of Arta (GHA), and General Hospital of Filiaton Thesprotia (GHF), were included in the study. Inclusion criteria for the purposes of the present study were a valid license to practice nursing and current employment at one of the sampled hospitals. Exclusion criteria were pregnancy, chronic conditions that may affect the musculoskeletal system (e.g., autoimmune diseases, arthritis), and recent (within the last six months) major injury that affected the musculoskeletal system (e.g., ruptured meniscus).
These hospitals were selected because they receive a large number of patients daily and employ a competent sample of nursing staff of varying educational levels and a wide range of professional experience.
A total of 500 questionnaires were distributed to randomly selected members of the nursing staff across a wide range of departments and clinics (departments of pathology, surgery, pediatrics, emergency departments, and intensive care units), as well as to staff of different educational levels. Questionnaires were distributed during the morning shift due to the higher number of employees working during that period. Of the 500 questionnaires distributed, 402 were returned completed, resulting in an overall response rate of 80.4%.
Data collection
Data collection took place from January 2024 to December 2024, using a structured questionnaire comprising three sections (Appendices). The first section gathered sociodemographic information, including personal and anatomical characteristics, work sector, hospital workplace, years of experience in the current position, and workplace environment.
The second section incorporated the Nordic Musculoskeletal Questionnaire (NMQ), developed by Kuorinka et al. [17], a validated self-administered screening tool designed to assess the prevalence of musculoskeletal disorders within a population. In the present study, the NMQ was used to analyze the relationship between the workplace environment and WrMSDs. The questionnaire has been translated, culturally adapted, and validated for use in Greek [18]. While it has been previously administered to residents of rural Crete [19], it has not yet been used among nursing staff in Epirus. The NMQ is freely available for research and educational use; thus, no specific permission for non-commercial application was obtained.
The third section included the RAND Short Form-36 version 1, which is a publicly available tool for non-commercial use and does not require licensing or permission. The instrument and scoring instructions are freely distributed by the RAND Corporation and are widely used in academic research to assess the overall QoL [20]. The RAND SF-36 consists of 36 Likert-type items evaluating participants’ ability to perform daily activities. These 36 items are grouped into eight underlying dimensions (bodily function, physical role, emotional role, mental health, physical pain, general health, vitality, and social functioning). Responses are scored on a scale from 0 to 100, with higher scores indicating better QoL. Two-component summary scores differentiate between physical health (Physical Component Score, PCS) and mental health (Mental Component Score, MCS). The RAND SF-36 has demonstrated reliability and validity in previous research [21].
Statistical analysis
Data were originally collected using a custom-made Excel spreadsheet form (Microsoft Corporation, Redmond, Washington). All statistical analyses were performed within the environment of the open programming language R (version 4.2.1, R Foundation for Statistical Computing, Vienna, Austria). Study outcomes were the diagnosis of WrMSDs (by a certified MD) within the last six months, the PCS score regarding physical QoL, and the MCS score regarding mental QoL. Continuous variables are presented as mean ± SD, whereas categorical variables are presented as frequencies and percentages. Chi-square tests were used to evaluate the association between the incidence of WrMSD medical diagnosis and categorical predictors. The Pearson correlation coefficient was used to examine the association between PCS score and MCS score. The magnitude of the correlation was evaluated using the thresholds proposed by Cohen [22]: trivial <0.1, small (0.11-0.30), moderate (0.31-0.50), large (0.51-0.70), very large (0.71-0.90), and almost perfect (>0.90).
General linear models were used to estimate the effect of WrMSD medical diagnosis on QoL after adjustment for demographic and workplace characteristics. A “top-down” approach was used, where all possible predictors were initially considered, and variables that did not reach statistical significance were removed in an iterative procedure [23]. The final model reported was chosen based on model parsimony and interpretability. For all analyses, the level of statistical significance was set at p = 0.05.
Results
There were a total of 402 participants, and the majority were female (87.1%, n = 350). Approximately 90% were currently employed as a nurse or nursing assistant, and around 42% were senior staff with more than 25 years of working experience. The incidence of WrMSD in our study sample was 49.5% (n = 199), as shown in Table 1.
The most frequent anatomical site for developing musculoskeletal complaints is the lumbar spine (55.5%), followed by the head and cervical spine (34.8%), shoulder (24.1%), wrist (23.9%), and knee joint (22.1%) (Table 2).
The association of potential demographic predictors of the WrMSD diagnosis is presented in Table 3. The incidence of WrMSD diagnosis had a strong association with the factor hospital as well as with nursing seniority.
Table 3: Association between WrMSD diagnosis and demographic characteristicsp-value = level of significance for the corresponding chi-square test. All p-values <0.05 are considered statistically significant. Values are given as n (%) per factor level.UHI: University Hospital of Ioannina, GHI: General Hospital of Ioannina "G. Hatzikosta", GHP: General Hospital of Preveza, GHA: General Hospital of Arta, GHF: General Hospital of Filiaton Thesprotia, BMI: body mass index, WrMSD: work-related musculoskeletal disorders, χ2: chi-squared, df: degrees of freedom.
The incidence of WrMSD diagnosis had a strong association with several nursing tasks, including moving patients, transporting materials with and without a wheelbarrow, prolonged sedentary activity, lifting or carrying objects, and lifting or carrying patients (Table 4).
Table 4: Association between WrMSD diagnosis and nursing tasksp-value = level of significance for the corresponding chi-square test. All p-values <0.05 are considered statistically significant. Values are given as n (%) per factor level.WrMSD: work-related musculoskeletal disorder, χ2: chi-squared, df: degrees of freedom.
The incidence of WrMSD diagnosis had no association with most workplace characteristics; the only strong association was observed between the incidence of WrMSD diagnosis and the degree or intensity of heavy object lifting during nursing tasks (Table 5).
Table 5: Association between WrMSD diagnosis and work place characteristicsp-value = level of significance for the corresponding test. All p-values <0.05 are considered statistically significant. Values are given as n (%) per factor level.WrMSD: work-related musculoskeletal disorder, χ2: chi-squared, df: degrees of freedom, FE: Fisher’s exact test.
There was a statistically significant, positive but small correlation between the physical (PCS) and mental (MCS) dimensions of QoL (r = 0.14, 95% CI (0.04, 0.24), p = 0.005). Thus, PCS and MCS are largely unrelated variables (Figure 1).
Scatterplot showing the association between PCS and MCSOpen circles indicate the corresponding PCS and MCS raw data for each participant. Black solid line indicates regression line with 95% confidence intervals (dotted lines).PCS: Physical Component Score, MCS: Mental Component Score.
WrMSD diagnosis, nursing seniority, and position were statistically significant predictors of PCS (Table 6). On the contrary, hospital, gender, educational background, BMI classification, and break duration had no impact on PCS. More specifically, nursing personnel with a WrMSD diagnosis had −5.7 (−7.4; −4.1) lower PCS on average compared to nursing personnel without a WrMSD diagnosis (p < 0.001). Participants with 20-24 and >25 years of working experience had −5.9 (−9.1; −2.6) and −6.6 (−9.7; −3.5), respectively, lower PCS on average compared to nursing personnel with <5 years of working experience (p < 0.001). Finally, nurse and nursing supervisors/assistant supervisors had 3.1 (1.3; 4.9) and 4.1 (0.9; 7.3) respectively higher PCS on average compared to nursing assistants (p < 0.001).
Predictors of the mental dimension of QoL (MCS) are presented in Table 7. Hospital and break duration were statistically significant predictors of MCS. On the contrary, WrMSD diagnosis, nursing seniority, position, gender, educational background, and BMI classification had no impact on MCS. Participants with a break duration of 20 min had 4.3 (0.4; 8.2) higher MCS on average compared to nursing personnel with no break (p = 0.032). Finally, participants from GHF had −5.8 (−9.2; −2.3) lower MCS on average compared to participants from UHI (p < 0.001).
Discussion
The presented study documented the incidence of WrMSDs in a sample of nursing personnel across five hospitals in a large region in Northwestern Greece, identified demographic and other predictors of WrMSDs, and examined the effect of WrMSDs on QoL. Our research hypothesis was that the incidence of WrMSDs would be high (40-60%) and similar to previously reported data, and that the diagnosis of WrMSDs would be associated with reduced QoL.
The incidence of WrMSD in our study sample was 49.5% (n = 199). Previous studies suggest that the prevalence of WMSDs among nurses can range from 30% to over 70%, depending on specific job roles, hospital settings, and geographical locations [2-5]; thus, our results lie within approximately the median incidence reported in the literature. For example, on the high end of the incidence rate, Tinubu et al. [24] reported a prevalence of 78% among Nigerian nurses, while Yan et al. [25] observed a prevalence of 77.4% among Chinese nurses. On the low end of the incidence rate, Clari et al. [4], in a multicenter cross-sectional study, showed that 48.3% of operating room nurses reported one or more episodes of upper limb pain.
Furthermore, our results indicated that the most frequent anatomical site for developing musculoskeletal complaints was the lumbar spine (55.5%), followed by the head and cervical spine (34.8%), shoulder (24.1%), wrist (23.9%), and knee joint (22.1%). Our data are in line with previous reports [2,3,8,15,26,27]. Most of these studies employed the Nordic Musculoskeletal Questionnaire, which further enhances the validity of our results.
We observed that working seniority was the demographic variable with the strongest association with WrMSD diagnosis. In addition, the incidence of WrMSD diagnosis had a strong association with several nursing tasks (moving patients, transporting materials with and without wheelbarrows, prolonged sedentary activity, lifting/carrying objects, and lifting/carrying patients); however, we did not observe any association with most of the workplace characteristics. The only strong association was between the incidence of WrMSD diagnosis and the degree or intensity of heavy object lifting nursing tasks. These results are supported by previous meta-analytical findings indicating that the physical demands of the nursing profession (i.e., bending and twisting), as well as the physical demands of nurse-patient interaction (i.e., turning, dressing, bathing, seating, transferring patients), are considered risk factors for the development of WrMSD [2,7].
WrMSD diagnosis, nursing seniority, and position were statistically significant predictors of PCS. Previous studies report mixed findings on the effect of WrMSD on QoL [13-15], while the effect of seniority has not been examined thoroughly [24]. In addition, both nursing personnel and nursing supervisors or assistant supervisors reported significantly better QoL compared to assistant nurses, although current position was not associated with WrMSD diagnosis. These results may further indicate the unique effects of the above variables on QoL and that factors unrelated to WrMSD are responsible for the lower QoL in nursing assistants and more senior personnel. Regarding MCS, the only statistically significant predictors were hospital and break duration, while WrMSD had no impact on MCS. It appears that a sufficient amount of break time during the nursing shift is necessary for alleviating work-related stress [13-15]. It is worth noting that the participants of the present study reported PCS and MCS scores that are considered relatively low compared to the adult population worldwide [28].
The main limitation of the present study is that data regarding the occurrence of WrMSD were based on self-reported information provided by the study participants, and no actual objective testing was conducted to confirm the diagnosis. Thus, WrMSD caused by non-work-related factors cannot be eliminated. In addition, the study may be subject to selection bias, as individuals experiencing musculoskeletal symptoms, particularly those perceived to be work-related, might have been more motivated to participate. Distributing the questionnaire primarily during morning shifts may have excluded night shift workers or those with irregular schedules, who may differ in exposure or risk. These factors may limit the generalizability of the findings. A further limitation is that the Nordic Musculoskeletal Questionnaire does not assess comorbidities or coexisting health conditions, which may influence the reported symptoms and act as potential confounders. Future research should consider integrating broader health assessment tools to better account for these factors. Finally, while we investigated five hospitals in Northwestern Greece, approximately 50% of the participants were employed in the largest hospital of the area (UHI). While this may introduce some bias in the reported results, it also increases the ecological validity of the results in the sense that most hospitals in smaller cities around Greece are considered understaffed in nursing and medical personnel.
Conclusions
In conclusion, almost half of the participants had been diagnosed with WrMSD, with the lumbar spine being the most frequently affected site. Several nursing tasks were significantly associated with the occurrence of WrMSD. The physical component of QoL was negatively affected by the presence of WrMSD, as well as by nursing seniority and job position. On the contrary, WrMSD had no impact on the mental component of QoL. These findings suggest that interventions aimed at reducing the incidence of WrMSDs may contribute to improvements in PCS among nursing personnel. However, targeted strategies beyond WrMSD prevention are necessary to enhance MCS in this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Work-related musculoskeletal symptoms among employees with different tasks: Ahlia university case study Physiother Quart Tantawy S 5964302022
- 2Work-related musculoskeletal disorders among nurses: systematic review J Ergon Ellapen TJ Narsigan S 1642014
- 3Work-related musculoskeletal disorders among registered general nurses: a case of a large central hospital in Harare, Zimbabwe BMC Res Notes Chiwaridzo M Makotore V Dambi JM Munambah N Mhlanga M 3151120182977645210.1186/s 13104-018-3412-8PMC 5960155 · doi ↗ · pubmed ↗
- 4Upper limb work-related musculoskeletal disorders in operating room nurses: a multicenter cross-sectional study Int J Environ Res Public Health Clari M Garzaro G Di Maso M 16201910.3390/ijerph 16162844 PMC 672041531395811 · doi ↗ · pubmed ↗
- 5Investigating prevalence of musculoskeletal disorders among Iranian nurses: a systematic review and meta-analysis Clin Epidemiol Glob Health Saberipour B Ghanbar SI Zarea K Gheibizadeh M Zahedian M 51351872019
- 6The effect of occupational exposure to ergonomic risk factors on osteoarthritis of hip or knee and selected other musculoskeletal diseases: a systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury Environ Int Hulshof CT Pega F Neupane S 10634915020213354691910.1016/j.envint.2020.106349 · doi ↗ · pubmed ↗
- 7Prevalence of work-related musculoskeletal disorders among nurses: a meta-analysis Iran J Public Health Sun W Yin L Zhang T Zhang H Zhang R Cai W 4634755220233712489710.18502/ijph.v 52i 3.12130 PMC 10135498 · doi ↗ · pubmed ↗
- 8Musculoskeletal disorders and working conditions among Iranian nursing personnel Int J Occup Saf Ergon Arsalani N Fallahi-Khoshknab M Josephson M Lagerström M 6716802020142551380210.1080/10803548.2014.11077073 · doi ↗ · pubmed ↗