Recurrent Kimura disease in an African American woman with concordant ultrasound imaging: A case report and literature review
Janet Choi, Jonathan Sterman, Hatice Zengin, Bijal Amin, Benedict Wu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
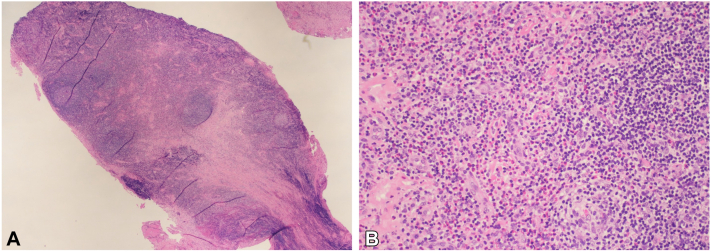 Figure 1
Figure 1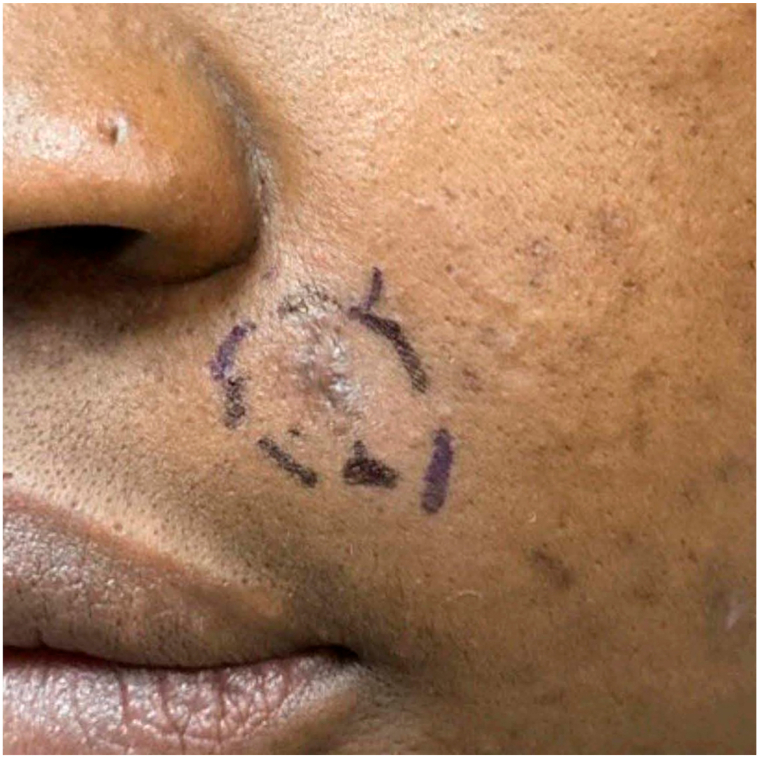 Figure 2
Figure 2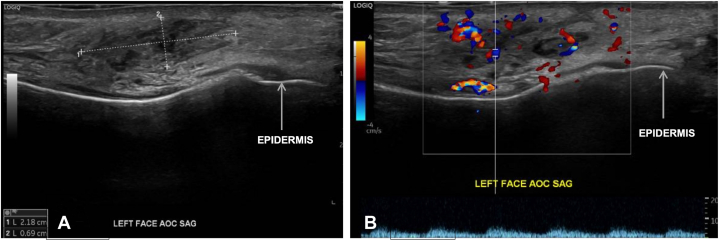 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Eosinophilic Disorders and Syndromes · Infectious Diseases and Mycology
Introduction
Kimura disease (KD) is a rare, benign condition characterized by hyperplastic lymphoid granuloma in the head and neck region, peripheral eosinophilia, and elevated serum immunoglobulin E levels. KD predominately occurs in young Asian men, but has been reported in 1 African American (AA) man.1 Diagnosing KD may be challenging as it can present similar to other lymphoid conditions such as Hodgkin’s disease, Langerhans cell histiocytosis, and reactive lymphadenopathy related to infections.2 Ultrasound can be diagnostic and assist with determination of nodule size and lymph node involvement. Herein, we present a case of KD in an AA woman with supportive ultrasound findings.
Case report
A 39-year-old AA woman with a history of morbid obesity and hypertension presented with a 3-cm mobile nodule on her left cheek, associated with intermittent left facial swelling. A 6-mm punch biopsy revealed blood vessels and fibromuscular tissue containing lymphoid aggregates associated with many eosinophils, suggesting KD (Fig 1, A and B).Fig 1. Histopathology of Kimura disease. Hematoxylin and eosin (H&E) staining. A, H&E, 2×: A section shows dense lymphoid aggregates. B, H&E, 20×: The lymphoid infiltrate is accompanied by numerous eosinophils.
Laboratory testing revealed elevated immunoglobulin E levels but normal eosinophil counts. 4 months later, the nodule reappeared at the exact location (Fig 2), and the excisional biopsy showed similar histopathologic findings.Fig 2. Kimura disease: Clinical image of a nodule on the left cheek after the punch biopsy but before the excisional biopsy.
Ultrasound of the affected area demonstrated heterogeneous soft tissue thickening (Fig 3, A) and regions of hypervascularity containing multiple, normal-sized lymph nodes (Fig 3, B), aligning with reported sonographic features of KD.3Fig 3. Kimura disease ultrasound. A, Heterogeneous 2.2 × 0.7 cm area of subcutaneous soft tissue thickening on the left face. B, Color Doppler imaging of left face identifying areas of hypervascularity and multiple, normal-sized lymph nodes. AOC, Area of concern; SAG, sagittal view.
Discussion
KD is a chronic inflammatory disorder typically manifesting as a painless subcutaneous nodule or soft tissue swelling in the head and neck region, often invading nearby lymph nodes or parotid glands. Ultrasound is a valuable initial diagnostic resource, commonly revealing hypoechoic, round nodes with partially defined margins, and associated regional lymphadenopathy with preserved fatty hilum.3^,^4 Color Doppler sonograms often show hilar vascularity. In contrast, malignant nodes frequently show capsular vascularity and loss of hilar architecture.3 Confirmation of KD is often done via histopathologic evaluation. Treatment options for KD include oral corticosteroids, antihistamines, biologics, cytotoxic therapy, excision, and radiation, although recurrence rates are high at 56.3%.1^,^5 Recurrence risks include systemic diseases such as hypertension and obesity, both of which were seen in our patient.6
We reviewed all reported cases of adult KD in the head and neck with descriptive sonographic findings over the past 5 years (Table I).Table IReported cases of adult Kimura disease with descriptive ultrasound findingsAuthor last name, yAge/sexRace/ethnicityPeripheral eosinophiliaIgE levelUltrasound findingsDiagnostic modalitiesTreatmentTreatment responseLocationMarginEchogenicityInternal vascularity on color DopplerLymph nodes with maintained fatty hilumAdjacent lymphadenopathyMaehara, 2019756/MAsian/JapanesePresentElevated at 14,834 IU/mL (N: N/A)Left parotid regionN/AReticular pattern of hypoechoic areasPresentN/APresentImaging,∗ histopathologySystemic medication†Reduction in size with normalization of peripheral eosinophilia but persistently elevated IgE levelsPrayuenyong, 2022822/MAsian/ThaiPresentN/ALeft parotid and periparotid regionsWell definedHypoechoicPresentN/APresentImaging,‡ histopathologySuperficial parotidectomyResolution without recurrenceSangwan, 2020422/MN/APresentN/ARight parotid regionIll-definedPredominantly hyperechoic with hypoechoic areas withinPresentPresentPresentImaging,∗ histopathologyPatient is planned for surgical excisionN/AShivakumar, 2021935/MN/APresentN/ARight parotid regionN/AHeterogenous gland with altered echotextureN/APresentPresentImaging,‡ histopathologySystemic medication†Mild reduction in sizeYang, 2022557/MAsian/ChinesePresentElevated at >2000 IU/mL (N: <100 IU/mL)Bilateral anterior and posterior earsN/AHeterogeneously hypoechoic-isoechoicN/AN/APresentHistopathologySystemic medication§Reduction in size with normalization of peripheral eosinophilia but persistently elevated IgE. Follow-up is ongoing.Yorita, 20231019/FN/APresentElevated at 424.5 IU/mL (N: <170 IU/mL)Right parotid regionN/AHomogenously hypoechoicN/AN/AN/A‖Imaging,∗^,^‡ histopathologyN/AN/APresent case39/FAfrican American/non-HispanicAbsentElevated at 124.0 IU/mL (N: <100 IU/mL)Left cheekIll-definedPredominately hypoechoic with central hyperechoic areas withinPresentPresentAbsentHistopathologyExcisionRecurrence after first punch biopsy. Lost to follow-up after excision.F, Female; IgE, immunoglobulin E; M, male; N, normal; N/A, not available.∗MRI.†Oral corticosteroid therapy.‡CT.§First with corticosteroid therapy (prednisone), then biologic therapy (omalizumab then dupilumab).ǁLymphadenopathy observed on physical examination but not mentioned for ultrasound.
Four of 6 identified cases had diagnostic ultrasounds and biopsies performed. Reported ultrasound features included hypoechoic lesions (n = 5), peripheral lymphadenopathy (n = 4), internal vascularity (n = 3), and preserved fatty hilum (n = 2). Our patient demonstrated all these findings except for peripheral lymphadenopathy, possibly due to a more localized degree of tissue involvement. Additional imaging techniques including magnetic resonance imaging (n = 3) and computed tomography (n = 3) were used to determine the extent of disease.
We present this case of recurrent KD in an AA woman to enrich the limited reports of KD in non-Asian patients and to show ultrasound imaging as a potentially valuable tool in diagnosis and disease surveillance. Of note, as KD may mimic features of Hodgkin’s disease, hematologic malignancies should be prioritized in the differential diagnosis in older patients.6 However, in cases where malignancy is less likely and histopathologic findings are equivocal, ultrasound may be a practical, noninvasive diagnostic method.
Data sharing and data availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the present study.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Born L.J.Turney K.Germanas J.Kimura disease: unusual presentation in an African American male JAAD Case Rep 492024111310.1016/j.jdcr.2024.04.02238873245 PMC 11167202 · doi ↗ · pubmed ↗
- 2Gupta A.Shareef M.Lade H.Ponnusamy S.R.Mahajan A.Kimura's disease: a diagnostic and therapeutic challenge Indian J Otolaryngol Head Neck Surg 71Suppl 1201985585910.1007/s 12070-019-01601-531742081 PMC 6848465 · doi ↗ · pubmed ↗
- 3Ahuja A.Ying M.Mok J.S.Anil C.M.Gray scale and power Doppler sonography in cases of Kimura disease AJNR Am J Neuroradiol 223200151351711237977 PMC 7976832 · pubmed ↗
- 4Sangwan A.Goyal A.Bhalla A.S.Kimura disease: a case series and systematic review of clinico-radiological features Curr Probl Diagn Radiol 511202213014210.1067/j.cpradiol.2020.10.00333250297 · doi ↗ · pubmed ↗
- 5Yang B.Yu H.Jia M.Successful treatment of dupilumab in Kimura disease independent of Ig E: a case report with literature review Front Immunol 132022108487910.3389/fimmu.2022.1084879 PMC 979498836591252 · doi ↗ · pubmed ↗
- 6Chen Q.L.Dwa S.Gong Z.C.Kimura's disease: risk factors of recurrence and prognosis Int J Clin Exp Med 8112015214142142026885085 PMC 4723930 · pubmed ↗
- 7Maehara T.Munemura R.Shimizu M.Tissue-infiltrating immune cells contribute to understanding the pathogenesis of Kimura disease: a case report Medicine (Baltimore)98502019 e 1830010.1097/MD.0000000000018300 PMC 692235631852109 · doi ↗ · pubmed ↗
- 8Prayuenyong P.Charoonratana V.Kirtsreesakul V.Kimura's disease presenting with intraparotid and neck nodes: a case report and review of literature Ear Nose Throat J 1041_suppl 2025326 S 330S 10.1177/0145561322114449536476131 · doi ↗ · pubmed ↗