Diospyrobezoar (Persimmon Bezoar)-Induced Intestinal Obstruction in an Older Patient: A Case Report
Masato Habuka, Moeri Yamagiwa, Masataka Yonezawa, Asa Ogawa, Suguru Yamamoto

TL;DR
An older man developed intestinal blockage from eating too many persimmons, requiring surgery despite initial treatments.
Contribution
This case report highlights diospyrobezoar-induced intestinal obstruction in an elderly patient without typical risk factors.
Findings
A 93-year-old man with no prior gastric surgery or diabetes developed intestinal obstruction from a diospyrobezoar.
The bezoar was composed of over 98% tannin and required surgical removal after failed non-surgical treatments.
The case emphasizes the need for early diagnosis and patient education to prevent severe complications.
Abstract
Diospyrobezoar is a bezoar caused by excessive persimmon (Diospyros kaki) consumption, typically occurring in individuals with risk factors such as a history of gastric surgery, diabetes, or advanced age. We report the case of a 93-year-old man who presented with anorexia, nausea, and vomiting. Computed tomography revealed a bezoar-induced obstruction in the proximal jejunum. Despite initial management with Coca-Cola (The Coca-Cola Company, Atlanta, Georgia, United States) lavage and endoscopic fragmentation, surgical intervention was required because of persistent symptoms and intestinal ulceration. A 5 × 5-cm mass composed of >98% tannin was removed, confirming the presence of a diospyrobezoar. Further history assessment revealed that the patient consumed two persimmons daily. The patient recovered uneventfully after surgery and was discharged with dietary guidance. The present case…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
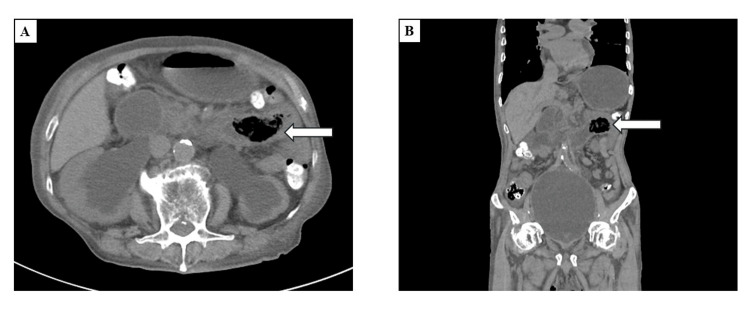 Figure 1
Figure 1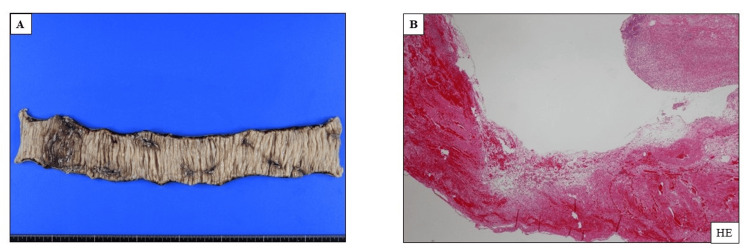 Figure 2
Figure 2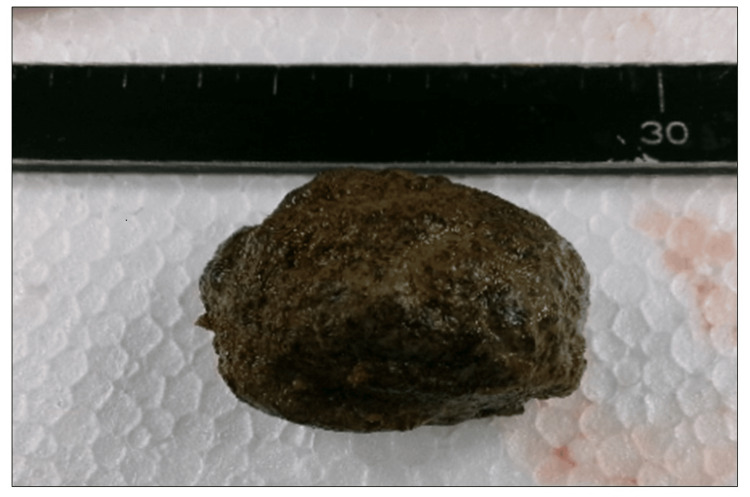 Figure 3
Figure 3| Variable | Patient Value | Reference Range |
| Blood count | ||
| White blood cells, /µL | 9,700 | 3,300-8,600 |
| Hemoglobin, g/dL | 10.3 | 13.7-16.0 |
| Platelets ×104/µL | 21.1 | 15.8-34.0 |
| Blood Gas Analysis | ||
| pH | 7.3 | 7.35-7.40 |
| Bicarbonate, mEq/L | 20.0 | 21.0-28.0 |
| Anion gap, mEq/L | 17.4 | 10.0-20.0 |
| Serum Chemistry | ||
| TP, g/dL | 7.4 | 6.6-8.1 |
| Albumin, g/dL | 3.2 | 4.1-5.1 |
| BUN, mg/dL | 93 | 8-20 |
| Cr, mg/dL | 4.48 | 0.65-1.0 |
| Na, mEq/L | 141 | 138-145 |
| K, mEq/L | 4.1 | 3.6-4.8 |
| Cl, mEq/L | 107 | 101-108 |
| Ca, mg/dL | 7.9 | 8-8.10.1 |
| P, mg/dL | 5.9 | 2.7-4.6 |
| AST, U/L | 19 | 13-30 |
| ALT, U/L | 8 | 10-42 |
| γGTP, U/L | 12 | 13-64 |
| ALP, U/L | 106 | 38-133 |
| LDH, U/L | 332 | 124-222 |
| T-Bil, mg/dL | 0.4 | 0.4-1.5 |
| CK, U/L | 276 | 59-248 |
| CRP, mg/dL | 1.13 | 0.00-0.1 |
| Variables | Funamizu et al. (2015) [ | Ha et al. (2007) [ | de Toledo et al. (2012) [ | Ohya et al. (2023) [ | Zheng et al. (2014) [ | Present Case |
| Age (years), sex | 67, F | 73, M | 66, M | 93, F | 27, M | 93, M |
| Duration of excessive persimmon ingestion | Regular intake of persimmon | Not mentioned | 6 days | Regular intake of persimmon | 2 weeks | Regular intake of persimmon |
| Underlying disease | Previous surgery for esophageal cyst and cesarean section | Hypereosinophilic syndrome and prednisolone use; previous Coca-Cola lavage for gastric diospyrobezoar | Diabetes mellitus; previous gastrectomy and vagotomy | Dementia; previous gastrectomy and cholecystectomy | Not mentioned | Hypertension; prostatic hypertrophy |
| Clinical symptoms | Abdominal distention and pain; Vomiting | Vomiting after 1 month of Coca-Cola lavage | Abdominal pain with signs of peritoneal irritation; Nausea | Nausea; Anorexia | Abdominal distention and pain; Nausea | Anorexia; Nausea; Vomiting |
| Diagnostic procedures | Radiograph CT | Radiograph Ultrasound | Radiograph | CT Gastroenterography Laparoscopy | Radiograph CT Endoscopy | CT Endoscopy |
| Treatment | Ileus tube Laparotomy | Laparotomy | Laparotomy | Ileus tube Laparotomy | Ileus tube; Coca-Cola lavage; Endoscopic fragmentation | Ileus tube; Coca-Cola lavage; Endoscopic fragmentation; Laparotomy |
| Diospyrobezoar size | 7 cm × 4 cm | Size not mentioned; Three diospyrobezoar pieces were identified | 5 cm × 12 cm | 4 cm × 5 cm | 5 cm × 6 cm | 5 cm × 5 cm |
| Diospyrobezoar component analysis | Yes | Yes | Not mentioned | Yes | Not mentioned | Yes |
| Outcome | Recovery | Recovery | Recovery | Recovery | Recovery | Recovery |
| Prevention of recurrence | Not mentioned | Not mentioned | Dietary orientation | Not mentioned | Dietary orientation | Dietary orientation |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions · Surgical Sutures and Adhesives · Hernia repair and management
Introduction
Bezoars are masses of indigestible material that accumulate in the gastrointestinal tract, most often in the stomach. Among them, diospyrobezoars are a distinct subtype formed from excessive consumption of persimmons (Diospyros kaki), which are rich in soluble tannins and dietary fibers [1]. When exposed to gastric acid, these tannins can polymerize and interact with proteins and cellulose to form a hard, cohesive mass that resists digestion [2].
Diospyrobezoars are relatively rare but can cause significant clinical symptoms, particularly when they lead to gastrointestinal obstruction. Typically, they are associated with several risk factors, including prior gastric surgery, diabetes, and advanced age. These risk factors impair mechanical digestion and transit, creating a favorable environment for bezoar formation [2]. However, cases of intestinal obstruction in older adults without these common risk factors are extremely rare. We present the case of a 93-year-old man who developed intestinal obstruction caused by a diospyrobezoar, despite having no history of gastric surgery or diabetes.
Case presentation
A 93-year-old man with stage 5 chronic kidney disease (CKD) of unknown etiology was referred to our hospital with a two-day history of anorexia, nausea, and vomiting. He had previously opted for conservative kidney management because of his advanced age; however, he had not received dietary counseling regarding the consumption of potassium-rich fruits. He had a history of hypertension and benign prostatic hyperplasia but had no history of gastric surgery or diabetes. His medications included sacubitril/valsartan, amlodipine, carvedilol, daprodustat, and tamsulosin.
On admission, his vital signs were as follows: temperature, 37.2°C; blood pressure, 174/66 mmHg; pulse, 77 beats/minute; respiratory rate, 18 breaths/minute; and oxygen saturation, 100% on room air. He appeared ill and fatigued. Physical examination revealed abdominal tenderness without rebound, decreased bowel sounds, and bilateral pitting edema. Laboratory tests revealed anemia, renal dysfunction, and metabolic acidosis. Table 1 shows the clinical data of the patient.
Abdominal computed tomography (CT) revealed bilateral hydronephrosis due to prostatic enlargement and a large gas-containing mass in the proximal jejunum, indicating a bezoar-induced intestinal obstruction (Figure 1).
Computed tomography (A: axial view; B: coronal view) showing bilateral hydronephrosis and a massive gas-containing structure in the lumen of the proximal jejunum (arrow)
A transnasal ileus tube was inserted to achieve proximal decompression, which reduced the intestinal dilation; however, it did not resolve the obstruction. Coca-Cola (The Coca-Cola Company, Atlanta, Georgia, United States) lavage was administered every 12 hours, and endoscopic fragmentation was attempted on day 6 of hospitalization. However, the removal of the bezoar was unsuccessful. Because of the ulceration of the adjacent intestinal wall, laparoscopic partial small bowel resection was performed on day 7. Histopathological examination of the resected specimen revealed multiple ulcers (Figure 2).
Histological findings of the small intestine samples obtained during laparotomy(A) Macroscopic examination showing multiple ulcers in the resected small intestine; (B) Hematoxylin & eosin staining showing an ulcer, neutrophil infiltration, and hemorrhage
A 5 × 5-cm bezoar was extracted (Figure 3), which contained over 98% tannin on component analysis, confirming it to be a diospyrobezoar.
Image of the removed diospyrobezoarThe diospyrobezoar was hard and rough, with a dark brown surface
Further, the patient’s dietary history revealed that he had a persimmon tree in his garden, and he consumed two persimmons daily. The patient’s postoperative course was uneventful, and he was discharged with instructions to limit his persimmon intake to only one fruit per day.
Discussion
We reported a rare case of diospyrobezoar-induced intestinal obstruction requiring surgical resection in an older patient with no history of gastric surgery or diabetes.
Diospyrobezoars are formed when unripe persimmons, which contain high tannin concentrations, are ingested in large quantities. The tannins in the fruit form a coagulum that can cause diospyrobezoars [2]. Previous gastric surgery, presence of diabetes, and advanced age are the risk factors for diospyrobezoar formation. This condition results in gastric acidity, stasis, and impaired gastric motility [3]. Endoscopic examination and CT, which reveal the presence of an intraluminal mass with a mottled gas appearance and a dilated small bowel proximal to the obstruction, along with a careful review of the patient’s medical history, can help in the diagnosis of diospyrobezoar. In our case, although the patient had no history of surgery or diabetes, his clinical symptoms and imaging findings led to the suspicion of a bezoar; thus, he was diagnosed with a diospyrobezoar based on his dietary history and the results of the component analysis.
Intestinal obstruction caused by diospyrobezoars is rare and often requires urgent surgical intervention. A literature search using the terms “diospyrobezoar” or “persimmon bezoar” and “intestinal obstruction” or “ileus” revealed only five reported cases (Table 2) [4-8].
All five cases were characterized by abdominal pain, nausea, and vomiting, which are typical symptoms of intestinal obstruction, and three of them had a history of upper gastrointestinal surgery. Although treatments such as Coca-Cola lavage and endoscopic fragmentation are available, diospyrobezoars are often resistant to dissolution because of their harder consistency, compared with other types of bezoars [9]. Thus, surgical excision is inevitable in patients with an intestinal obstruction or a refractory diospyrobezoar. Among the five reported cases, four required surgery (Table 2). Our patient exhibited ulceration of the surrounding intestinal tract, and further delays in surgical treatment could have resulted in fatal complications, including bacterial peritonitis. Diospyrobezoar-induced intestinal obstruction should be diagnosed early based on the patient’s medical history, typical symptoms, and imaging findings, and surgical intervention should be selected to minimize the mortality risk.
Our case is notable because it represents one of the few instances of diospyrobezoar-induced obstruction in an older patient with no prior gastric surgery or diabetes. In the 1980s, when persimmons became popular in Israel, the number of diospyrobezoar cases increased. However, the incidence considerably decreased after the public was warned about the risks associated with the overconsumption of persimmons [10], indicating that public education about such risks can reduce the incidence of this rare condition. Older adults are more prone to diospyrobezoar-induced obstruction because of decreased gastric motility and altered digestive function [11]. Therefore, clinicians should be aware of the risks of diospyrobezoar-induced obstruction in older individuals who consume persimmon. Moreover, educating patients about the risks of excessive persimmon consumption is essential for preventing this condition.
Conclusions
The present case highlights the importance of identifying diospyrobezoar-induced intestinal obstruction in older individuals who consume persimmon, even in the absence of common risk factors, such as prior gastric surgery or diabetes. Early diagnosis based on the imaging findings and dietary history, followed by timely surgical treatment, is essential to prevent severe complications. Moreover, educating patients about the risks of excessive persimmon consumption is essential to prevent this condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diospyrobezoar and a fondness for persimmons QJM Matsuura H Moritou Y Kinoshita T Asano Y Mashima S Hayashi K 40140211020172833994210.1093/qjmed/hcx 039 · doi ↗ · pubmed ↗
- 2Review of the diagnosis and management of gastrointestinal bezoars World J Gastrointest Endosc Iwamuro M Okada H Matsueda K Inaba T Kusumoto C Imagawa A Yamamoto K 336345720152590121210.4253/wjge.v 7.i 4.336PMC 4400622 · doi ↗ · pubmed ↗
- 3Surgical aspects of gastrointestinal persimmon phytobezoar treatment Am J Surg Krausz MM Moriel EZ Ayalon A Pode D Durst AL 5265301521986377733210.1016/0002-9610(86)90221-7 · doi ↗ · pubmed ↗
- 4Intestinal obstruction caused by persimmon bezoar: a case report Int Surg Funamizu N Kumamoto T Watanabe A Okamoto T Yanaga K 1194119810020152659549310.9738/INTSURG-D-14-00269.1 · doi ↗ · pubmed ↗
- 5Acute intestinal obstruction caused by a persimmon phytobezoar after dissolution therapy with Coca-Cola Korean J Intern Med Ha SS Lee HS Jung MK Jeon SW Cho CM Kim SK Choi YH 3003032220071830969310.3904/kjim.2007.22.4.300PMC 2687663 · doi ↗ · pubmed ↗
- 6Diospyrobezoar as a cause of small bowel obstruction Case Rep Gastroenterol de Toledo AP Rodrigues FH Rodrigues MR Sato DT Nonose R Nascimento EF Martinez CA 596603620122327198910.1159/000343161 PMC 3529578 · doi ↗ · pubmed ↗
- 7Laparoscopic-assisted treatment for diospyrobezoar-induced intestinal obstruction after distal gastrectomy and cholecystectomy Drug Discov Ther Ohya Y Hayashida S Yoneda A 2172191720233733180910.5582/ddt.2023.01009 · doi ↗ · pubmed ↗
- 8''Sandwich'' treatment for diospyrobezoar intestinal obstruction: a case report World J Gastroenterol Zheng YX Prasoon P Chen Y Hu L Chen L 18503185062020142556182310.3748/wjg.v 20.i 48.18503 PMC 4277993 · doi ↗ · pubmed ↗