Distal Cholangiocarcinoma with Synchronous Intramural Bile Duct Metastasis: A Case Report
Ryota Kiuchi, Hitaru Ishioka, Tomohiro Akutsu, Mitsumasa Makino, Hisato Ishimatsu, Masanori Yamazaki, Tsuyoshi Shoji, Rui Nomura, Yutaka Kurebayashi, Hirotoshi Maruo

TL;DR
A rare case of multiple bile duct tumors was found to be a single cancer with metastasis, not separate cancers.
Contribution
The paper presents a unique case of synchronous intramural bile duct metastasis in distal cholangiocarcinoma.
Findings
Two tumors were found to be connected through immunohistochemical and pathological evidence.
The smaller tumor was identified as a metastasis of the larger tumor rather than an independent lesion.
Abstract
Distal cholangiocarcinoma is a malignant tumor that arises from the epithelial cells of the bile duct. Several risk factors associated with cholangiocarcinoma have been identified. Multiple distal cholangiocarcinomas may occur in patients with several risk factors for cholangiocarcinoma. However, synchronous multiple distal cholangiocarcinomas in the absence of risk factors are rare. Here, we presented a case of multiple tumors on the bile duct diagnosed as distal cholangiocarcinoma with synchronous intramural bile duct metastasis. A 67-year-old man was referred to our hospital for evaluation of jaundice. Contrast-enhanced computed tomography revealed an enhanced tumor on the common bile duct. Endoscopic retrograde cholangiography showed bile duct stenosis due to a nodular tumor of the common bile duct. We performed subtotal stomach-preserving pancreaticoduodenectomy under diagnosing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
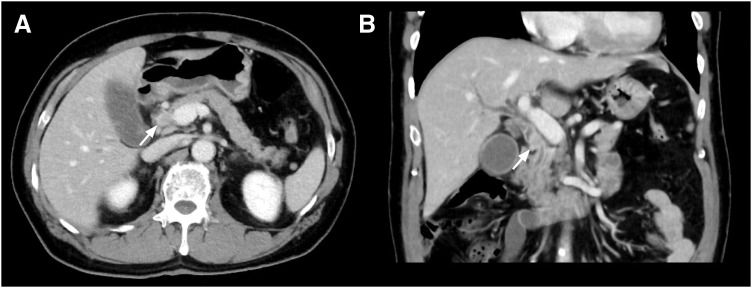 Fig. 1
Fig. 1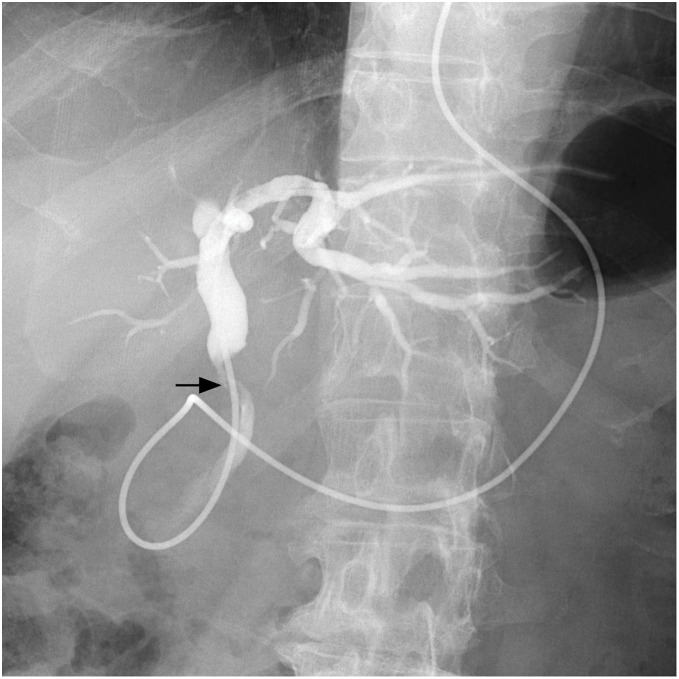 Fig. 2
Fig. 2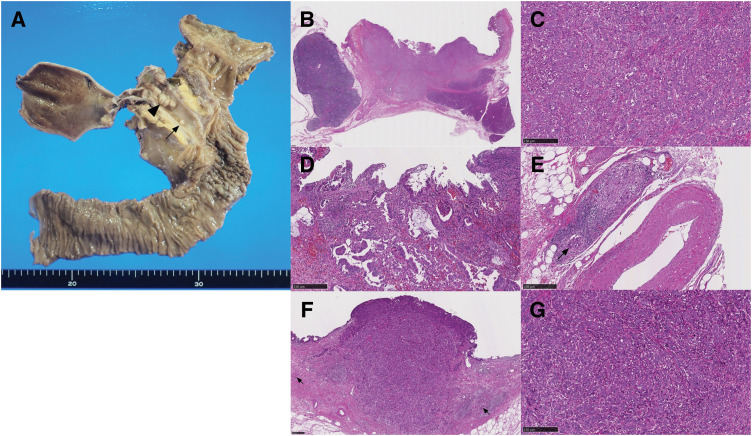 Fig. 3
Fig. 3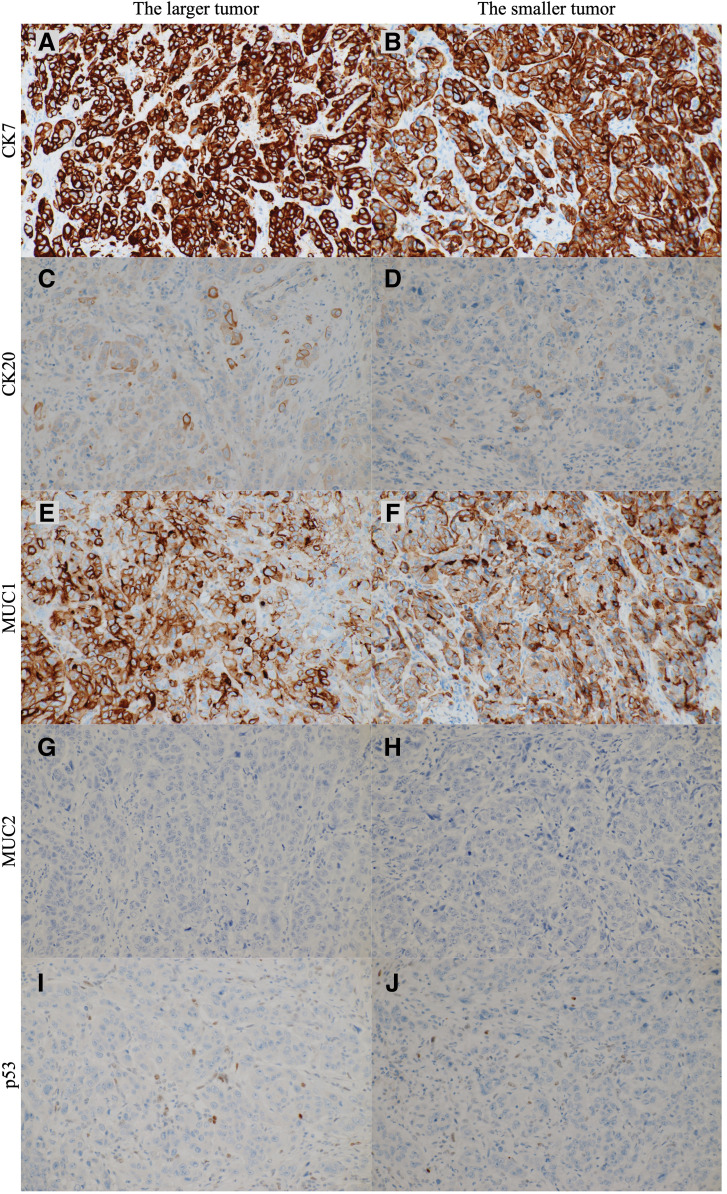 Fig. 4
Fig. 4| Author | Age | Gender | Surgical procedure | Larger tumor location | Larger tumor pathological results | Smaller tumor location | Smaller tumor pathological results | Immunohistological staining | Genetic analysis | Primary or metastasis | Prognosis |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ogawa et al. | 69 | Male | PPPD | Middle bile duct | Por | Inferior bile duct | Mod | None | PCR | Synchronous metastasis | Not described |
| Bedoui et al. | 67 | Female | PPPD | Middle bile duct | Not described | Inferior bile duct | Not described | None | None | Not described | Not described |
| Sumiyoshi et al. | 78 | Male | 1st EHBD, | Perihilar bile duct | Mod | Inferior bile duct | Pap | None | None | Not described | 31 months, alive |
| Yoo et al. | 67 | Male | PPPD | Middle bile duct | Mod | Inferior bile duct | SCC | None | None | Double primary | 8 months, dead |
| Nishi et al. | 78 | Female | PPD | Middle bile duct | Wel | Inferior bile duct | Por | CD56, chromogranine A, synaptophysin | None | Double primary | 18 months, dead |
| Morita et al. | 69 | Male | RHPD | Perihilar bile duct | Mod | Inferior bile duct | Por | p53 | PCR-SSCP | Double primary | 28 months, alive |
| Our case | 67 | Male | SSPPD | Middle bile duct | Por and mod | Inferior bile duct | Por | CK7, CK20, MUC1, MUC2, p53 | None | Synchronous metastasis | 7 months, alive |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Pancreatic and Hepatic Oncology Research · Cancer Diagnosis and Treatment
Abbreviation
HE hematoxylin and eosin
INTRODUCTION
Extrahepatic cholangiocarcinoma is a malignant tumor that arises from the epithelial cells of the extrahepatic bile duct. Extrahepatic cholangiocarcinoma is classified into perihilar and distal cholangiocarcinoma according to the anatomical location of the tumor. Several risk factors associated with distal cholangiocarcinoma have been identified, including pancreaticobiliary maljunction^1,2)^ and exposure of 1,2-dichloropropane.^3,4)^ Although multiple distal cholangiocarcinomas may occur in patients with these risk factors, most distal cholangiocarcinomas occur as a solitary lesion. The occurrence of synchronous multiple distal cholangiocarcinomas in patients without these risk factors is rare. Additionally, it is crucial to identify the relationship between these multiple distal cholangiocarcinomas.
Herein, we presented a case of distal cholangiocarcinoma with synchronous intramural bile duct metastasis occurring in the absence of any identifiable risk factors.
CASE PRESENTATION
A 67-year-old man presented to a local physician with a fever. Physical examination revealed scleral icterus, and the laboratory test showed hyperbilirubinemia and an elevated C-reactive protein level. He was referred to our hospital for a comprehensive examination and subsequent treatment. Contrast-enhanced computed tomography revealed an enhanced tumor on the common bile duct and intrahepatic bile duct dilation (Fig. 1). Cholangiography using a nasal biliary tube showed the bile duct stenosis due to the nodular tumor of the common bile duct (Fig. 2). Cholangiography did not confirm the evidence of pancreaticobiliary maljunction. Biopsy of the bile duct tumor diagnosed moderately differentiated adenocarcinoma. Preoperative radiological examinations detected only one lesion on the distal bile duct. After jaundice improved with retrograde biliary drainage, subtotal stomach-preserving pancreaticoduodenectomy was performed under diagnosing distal cholangiocarcinoma. Although postoperative pancreatic fistula in biochemical leaks, classified by the International Surgical Group of Pancreatic Fistula,^5)^ developed, the postoperative pancreatic fistula was managed conservatively. The patient was discharged on the 23rd postoperative day.
Findings of contrast-enhanced CT. Contrast-enhanced CT revealed a well-enhanced tumor in the middle bile duct (arrow) in the axial image (A) and coronal image (B).
Findings of cholangiography. Cholangiography using a nasal biliary tube revealed a contrast defect in the middle bile duct (arrow). No evidence of pancreaticobiliary maljunction was found.
Macroscopic findings of the resected specimen showed a 27-mm nodular-infiltrating tumor at the middle bile duct and a 3-mm nodular tumor at the lower bile duct (Fig. 3A). The distance between those tumors was 10 mm. Pathological examinations revealed that the larger tumor was primarily composed of poorly differentiated adenocarcinoma, with a moderately differentiated component at the periphery of the tumor (Fig. 3B–3D). The invasive tumor thickness was 8 mm. Microscopic lymphovascular infiltration was observed (Fig. 3E). The smaller tumor was located within the submucosal layer (Fig. 3F). The smaller tumor was entirely composed of poorly differentiated adenocarcinoma, which was similar to the poorly differentiated component of the larger tumor (Fig. 3G). Additionally, microscopic lymphovascular infiltration was observed in the vicinity of the smaller tumor (Fig. 3F). These two tumors were completely separated by non-tumoral biliary epithelia, without atypia. These pathological results suggested that the smaller tumor was diagnosed as an intramural bile duct metastasis of distal cholangiocarcinoma via microscopic lymphovascular infiltration, rather than multiple independent lesions. The immunohistochemical staining was performed using CK7/20, MUC1/2, and p53 antibodies (Fig. 4). The tumor cells in both the larger and smaller lesions exhibited strongly positive for CK7 and MUC1, focally positive for CK20, and negative for MUC2. The staining pattern for p53 was wild pattern in both tumor cells. These results of immunohistochemical staining substantiated the homology between both lesions. No lymph node metastasis was observed. Using the UICC TNM classification, 8th edition, the tumor was diagnosed as T2N0M0 Stage IIA.^6)^ Although adjuvant chemotherapy with S1 was completed, multiple liver metastases occurred in the 7th month after surgery.
Findings of pathological examinations. (A) Macroscopic findings of resected specimen. Two lesions were identified on the bile duct. The larger lesion was situated at the middle bile duct and measured 27 mm in diameter (arrowhead). The smaller lesion was located at the lower bile duct and measured 3 mm in diameter (arrow). The distance between those tumors was 10 mm. Macroscopic findings showed no continuity between those lesions. (B) Findings of loupe image of larger distal cholangiocarcinoma (HE staining). (C) The poorly differentiated adenocarcinoma component was located at the center of the larger distal cholangiocarcinoma (HE staining, ×100). (D) The moderately differentiated adenocarcinoma component was located at the margin of the larger distal cholangiocarcinoma (HE staining, ×100). (E) Microscopic lymphovascular infiltration of the larger distal cholangiocarcinoma (arrow) (HE staining, ×100). (F) Findings of loupe image of smaller distal cholangiocarcinoma (HE staining, ×40). The smaller distal cholangiocarcinoma was located in the mucosal lamina propria. Additionally, microscopic lymphovascular infiltration was observed in the vicinity of the smaller tumor (arrow). (G) The smaller distal cholangiocarcinoma was entirely composed of poorly differentiated adenocarcinoma, analogous to that of the larger distal cholangiocarcinoma (HE staining, ×100).HE, hematoxylin and eosin
Findings of immunohistochemical staining examinations in larger and smaller distal cholangiocarcinomas. (A, B) Findings of immunohistochemical staining for CK7 (×200). The tumor cells in both tumors were strongly positive for CK7. (C, D) Findings of immunohistochemical staining for CK20 (×200). The tumor cells in both tumors were focally positive for CK20. (E, F) Findings of immunohistochemical staining for MUC1 (×200). The tumor cells in both tumors were strongly positive for MUC1. (G, H) Findings of immunohistochemical staining for MUC2 (×200). The tumor cells in both tumors were negative for MUC2. (I, J) Findings of immunohistochemical staining for p53 (×200). The staining patterns for p53 were wild pattern in both tumors. These results of immunohistochemical staining revealed the homology between larger and smaller distal cholangiocarcinomas.
DISCUSSION
Extrahepatic cholangiocarcinoma is a malignant tumor that arises from the epithelial cells of the extrahepatic bile duct. Extrahepatic cholangiocarcinoma is classified into perihilar or distal cholangiocarcinoma according to the anatomical location of the tumor. The incidence of distal cholangiocarcinoma varies from 0.53 to 2 cases per 100,000 person-years worldwide.^7)^ Several risk factors have been identified to be associated with distal cholangiocarcinoma, including pancreaticobiliary maljunction^1,2)^ and exposure of 1,2-dichloropropane.^3,4)^ Multiple distal cholangiocarcinomas may develop in patients with these risk factors. There have been several reports of metachronous cholangiocarcinoma after curative resection.^8–10)^ Including our case, seven cases of synchronous multiple cholangiocarcinomas in the absence of these risk factors have been reported^11–16)^ (Table 1). Among these cases, three cases were diagnosed as double primary cancers, two cases did not describe the relationship between the tumors in detail, and only two cases, including our case, were diagnosed as synchronous intramural bile duct metastasis. These results would underscore the rarity of distal cholangiocarcinoma with synchronous intramural bile duct metastasis.
In the case of synchronous multiple tumors being identified in the same organ, it is important to determine whether these tumors are diagnosed as multiple primary tumors. Multiple primary cancers have been defined according to the following criteria: (1) each tumor must present a definite picture of malignancy, (2) each tumor must be distinct, and (3) the probability that one tumor is the metastasis of the other must be ruled out.^17)^ In the context of extrahepatic cholangiocarcinoma, the relationship between multiple tumors should be considered in light of four proposed mechanisms: (1) intraductal spread of neoplastic cells via carcinoma in situ, (2) intramural metastasis via lymphovascular or perineural infiltration, (3) intramural seeding of neoplastic cells via bile juice, and (4) multicentric carcinogenesis in the setting of field carcinogenesis.^18)^ In our case, no identifiable risk factors for the development of cholangiocarcinoma were found. No evidence of carcinoma in situ was observed between the two lesions. The smaller tumor was primarily located under mucosal layer, making intramural seeding via bile juice an unlikely mechanism. Microscopic lymphovascular infiltrations were observed in the vicinity of both tumors. Furthermore, the smaller tumor, composed of poorly differentiated adenocarcinoma, resembled the larger tumor. Based on these pathological findings using hematoxylin and eosin (HE) staining, the case was diagnosed as distal cholangiocarcinoma with synchronous intramural bile duct metastasis.
Recent advances in immunohistochemical and genetic analyses have helped us evaluate the relationships between the multiple cholangiocarcinomas. Immunohistochemical staining of p53 protein and polymerase chain reaction-single-strand conformation polymorphism of TP53 gene aided in the evaluation of synchronous double cholangiocarcinomas as double primary cancers.^12)^ The loss of heterozygosity assay revealed the synchronous double cholangiocarcinomas as intramural bile duct metastasis.^14)^ Next-generation sequencing has been recently used to analyze the genomics of extrahepatic cholangiocarcinomas.^19,20)^ A comprehensive analysis of the molecular characteristics of primary and metachronous cholangiocarcinomas using next-generation sequencing has elucidated the pathways and mechanisms underlying multiple cholangiocarcinomas.^18)^ Comprehensive analysis revealed the three distinct molecular pathways: (1) the successional pathway, (2) the phylogenic pathway, and (3) the distinct pathway. Although genetic analyses were not performed in this case, immunohistochemical staining examination was conducted. The results of immunohistochemical staining using CK7/20, MUC1/2, and p53 antibodies revealed the homology between the larger and smaller tumors, and would substantiate the diagnosis established by the results from HE staining. These validation analyses including next-generation sequencing would have been possible if the advanced inspections could be made readily available.
The optimal treatment for extrahepatic cholangiocarcinoma is surgical resection, such as pancreaticoduodenectomy or hepatectomy with bile duct resection.^21,22)^ Several articles have reported aggressive reoperations for metachronous cholangiocarcinoma at the remnant bile duct following curative resection. Although reoperations after curative resection for cholangiocarcinoma require highly proficient surgical skills to secure sufficient surgical margins, these procedures with negative surgical margins can result in a favorable prognosis.^8,18,23)^ The benefits of surgical resection for distal cholangiocarcinoma with synchronous intramural bile duct metastasis remain unclear because of the rarity of this condition and the possibility of high malignancy due to the presence of metastasis at the time of resection. In this case, multiple liver metastases occurred in the 7th month after surgery. Nevertheless, curative surgical resection could contribute to prolong survival in patients accompanied by distal cholangiocarcinoma with synchronous intramural bile duct metastasis.
CONCLUSIONS
We experienced a patient of distal cholangiocarcinoma with synchronous intramural bile duct metastasis diagnosed based on the findings from HE and immunohistochemical staining. It is crucial to ascertain the relationship between these tumors in the cases of multiple distal cholangiocarcinomas being identified. Recent developments in immunohistochemical techniques, genetic analyses, and next-generation sequencing can facilitate assessment of the association between multiple distal cholangiocarcinomas.
DECLARATIONS
Funding
This study did not receive any funding.
Authors’ contributions
RK was involved in the clinical practice, conception, design, and acquisition of data.
HI, MM, RN, YK, and HM were involved in the clinical practice and conception and design.
TA, HI, MY, and TS approved the final version of the manuscript.
All authors have read and approved the manuscript, and they are responsible for the manuscript.
Availability of data and materials
The datasets used in this study are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
Informed consent was obtained from the patient for publication of this case report.
Competing interests
All authors declare that they have no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ohuchida J Chijiiwa K Hiyoshi M Long-term results of treatment for pancreaticobiliary maljunction without bile duct dilatation. Arch Surg 2006; 141: 1066–70.17116798 10.1001/archsurg.141.11.1066 · doi ↗ · pubmed ↗
- 2Tashiro S Imaizumi T Ohkawa H Pancreaticobiliary maljunction: retrospective and nationwide survey in Japan. J Hepatobiliary Pancreat Surg 2003; 10: 345–51.14598134 10.1007/s 00534-002-0741-7 · doi ↗ · pubmed ↗
- 3Kubo S Kinoshita M Takemura S Characteristics of printing company workers newly diagnosed with occupational cholangiocarcinoma. J Hepatobiliary Pancreat Sci 2014; 21: 809–17.25088751 10.1002/jhbp.137 · doi ↗ · pubmed ↗
- 4Kubo S Nakanuma Y Takemura S Case series of 17 patients with cholangiocarcinoma among young adult workers of a printing company in Japan. J Hepatobiliary Pancreat Sci 2014; 21: 479–88.24420816 10.1002/jhbp.86 · doi ↗ · pubmed ↗
- 5Bassi C Marchegiani G Dervenis C The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery 2017; 161: 584–91.28040257 10.1016/j.surg.2016.11.014 · doi ↗ · pubmed ↗
- 6Brierley JD Gospodarowicz MK Wittekind C. TNM Classification of Malignant Tumours: Wiley; 2017.
- 7Bridgewater JA Goodman KA Kalyan A Biliary tract cancer: epidemiology, radiotherapy, and molecular profiling. Am Soc Clin Oncol Educ Book 2016; 35: e 194–203.27249723 10.1200/EDBK_160831 · doi ↗ · pubmed ↗
- 8Kim DH Choi DW Choi SH Pancreaticoduodenectomy for secondary periampullary cancer following extrahepatic bile duct cancer resection. Ann Surg Treat Res 2014; 87: 94–9.25114889 10.4174/astr.2014.87.2.94PMC 4127899 · doi ↗ · pubmed ↗