Transcystic biliary tract exploration during single-stage treatment for cholecystitis/symptomatic cholelithiasis plus choledocholithiasis using the SpyGlass system: a favorable therapeutic proposal
Máximo Vicente Torres Guaicha, Tábata Lissette Tinoco Ortiz, Santiago Borja Villacres, Francisco Troya, Santiago Andrés Muñoz-Palomeque

TL;DR
A new single-stage surgical approach using the SpyGlass system successfully treats bile duct stones and gallbladder issues in one procedure.
Contribution
Demonstrates the feasibility of single-stage treatment using SpyGlass for choledocholithiasis and cholecystitis.
Findings
SpyGlass-assisted transcystic exploration achieved ductal clearance without choledochotomy or papillary trauma.
The patient recovered quickly, resuming oral intake within 6 hours and discharging within 36 hours.
The technique shows reduced complications and shorter hospital stays compared to traditional two-stage methods.
Abstract
Choledocholithiasis is traditionally managed via a two-stage approach involving endoscopic retrograde cholangiopancreatography followed by laparoscopic cholecystectomy. However, this method carries significant morbidity and logistical challenges. We report a case of a 70-year-old woman with symptomatic choledocholithiasis and mild pancreatitis successfully treated with a single-stage laparoscopic cholecystectomy and transcystic bile duct exploration using the SpyGlass DS II system. This technique enabled direct stone visualization, electrohydraulic lithotripsy, and successful ductal clearance without the need for choledochotomy or papillary trauma. The patient experienced an uneventful recovery, resuming oral intake within 6 hours and being discharged within 36 hours postoperatively. SpyGlass-assisted transcystic exploration offers important advantages over endoscopic retrograde…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
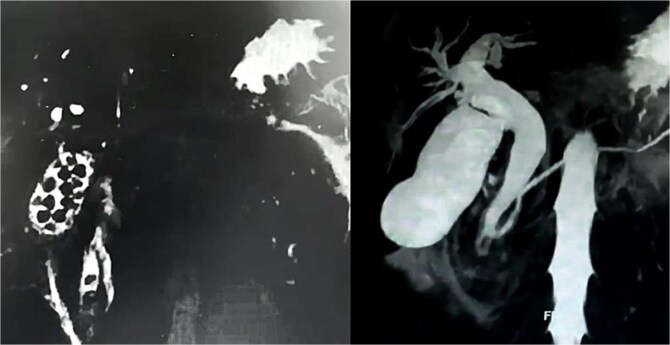 Figure 1
Figure 1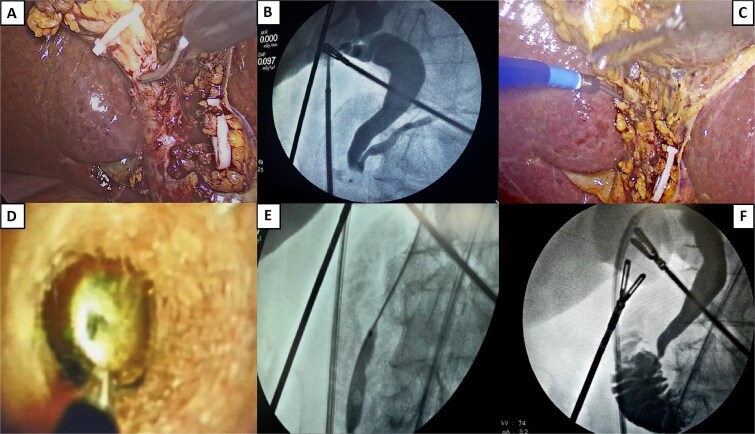 Figure 2
Figure 2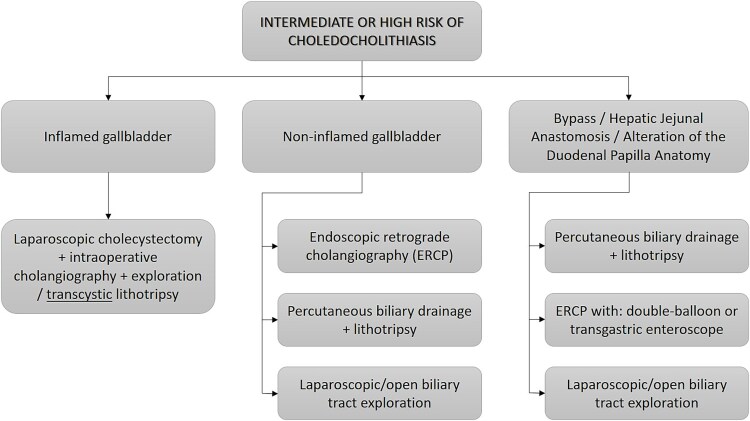 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Pancreatic and Hepatic Oncology Research
Introduction
Gallstone disease affects ~6% of the global population, with a higher prevalence among women and in certain geographic regions such as South America (up to 11%) [1]. Approximately 10%–15% of patients with cholelithiasis will eventually develop common bile duct (CBD) stones, which can lead to complications such as cholangitis and pancreatitis [2].
Traditionally, choledocholithiasis is managed in two stages: first endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy, followed by elective laparoscopic cholecystectomy. While effective, this approach is associated with ERCP-related complications and logistical challenges, especially in cases with altered anatomy or difficult papillary access. The “Rendezvous” procedure (intraoperative ERCP during cholecystectomy) also presents coordination and procedural limitations [3].
Single-stage laparoscopic CBD exploration (LCBDE) during cholecystectomy has emerged as a viable treatment. Studies have shown this approach to be equally effective—and sometimes superior—to the sequential ERCP-plus-surgery method [4].
Technological innovations, particularly the SpyGlass™ single-operator system, have significantly advanced bile duct exploration. The SpyGlass DS II, a 3.6-mm-diameter digital cholangioscope, allows direct visualization and therapeutic intervention via the cystic duct. It accommodates instruments such as electrohydraulic and laser lithotripsy probes, extraction baskets (SpyBasket®), and biopsy forceps (SpyBite®), facilitating ductal clearance without choledochotomy and enabling immediate confirmation of stone removal [5].
Here, we present a case experience involving single-stage laparoscopic cholecystectomy with transcystic cholangioscopy and electrohydraulic lithotripsy using the SpyGlass DS II system, demonstrating cost and morbidity advantages compared to the traditional two-stage approach or conventional open CBD exploration.
Case report
A 70-year-old woman with a history of arterial hypertension presented with a 72-hour history of epigastric pain radiating to the back, jaundice, nausea, and vomiting. Physical examination revealed a positive Murphy's sign. Laboratory tests showed leukocytosis, elevated liver enzymes aspartate aminotransferase (AST) 17× upper limit normal, alanine transaminase (ALT) 11× upper limit normal, gamma-glutamyl transpeptidase (GGT) 18× upper limit normal, direct hyperbilirubinemia, and mild pancreatitis without organ dysfunction. Abdominal ultrasound revealed gallbladder wall thickening and a 16 mm CBD. Magnetic resonance imaging (MRI) identified two CBD stones (4.4 and 4.0 mm) (Fig. 1).
Magnetic resonance cholangiography reconstruction (360°) demonstrating the presence of multiple gallbladder stones and two embedded in the distal common bile duct.
After supportive treatment for pancreatitis, the patient underwent laparoscopic cholecystectomy with transcystic CBD exploration using the SpyGlass DS II system and electrohydraulic lithotripsy (Fig. 2). The 150-minute procedure included intraoperative cholangiography and successful stone fragmentation.
Surgical procedure. (A) Opening of the cystic duct. (B) Initial cholangiography showing no passage into the duodenum and passage into the main pancreatic duct. (C) Introduction of a transcystic SpyGlass over a hydrophilic guidewire. (D) Stone lodged in the distal common bile duct, ready for fragmentation. An electrohydraulic lithotripsy probe is visible, aimed at the center of the stone. (E) Sphincteroplasty by balloon dilation. A notch is visible, coinciding with the sphincter of the Oddi area. (F) Final cholangiography showing free passage of contrast into the duodenum, with no filling defect.
Under general anesthesia and in reverse Trendelenburg position, four ports were placed in the standard cholecystectomy configuration. Intraoperative findings revealed a Parkland grade 3 gallbladder and Zühlke grade II adhesions between the gallbladder fundus and the anterior abdominal wall. Moderate perivesicular inflammatory fluid was sampled for culture. Careful dissection proceeded to achieve the critical view of safety. A long, wide cystic duct and a dilated CBD were identified. Hem-o-lock clips were placed on the cystic artery and distal cystic duct, which was then partially incised.
A Navigator 11–13F catheter was introduced through the midclavicular port for initial cholangiography, which revealed filling defects in the distal bile duct and no contrast passage into the duodenum, but with contrast reflux into the pancreatic duct. A hydrophilic guidewire was advanced into the duodenum using the Seldinger technique, followed by the insertion of the SpyGlass DS II system (Boston Scientific). This 3.5-mm-diameter, 65–cm-long scope features 30° tip angulation.
Choledochoscopy confirmed two stones occupying ~90% of the distal CBD lumen. Electrohydraulic lithotripsy was used to fragment stones delivering multiple shockwave pulses to achieve complete stone fragmentation. Then a percutaneous balloon was used for sphincteroplasty over 3 minutes, followed by saline flushing and fragmentation extraction using the SpyGlass instruments. Free contrast passage into the duodenum was confirmed, and final cholangiography showed no residual filling defects or contrast leakage, verifying biliary and duodenal integrity.
The patient had an uneventful recovery, tolerated oral intake 6 hours postoperatively, and was discharged 36 hours after surgery.
Discussion
Prompt management of choledocholithiasis is critical to avoid complications such as cholangitis or pancreatitis [6]. Although ERCP is a well-established treatment, it carries significant risks, including pancreatitis (3%–5%, up to 10% in high-risk patients), duodenal perforation (<1%), bleeding (1%–2%), and cholangitis (<1%) [5, 7]. ERCP failure occurs in 5%–10% of cases, particularly with anatomical challenges such as periampullary diverticula [8].
Single-stage strategies like LCBDE during cholecystectomy offer several benefits, including high success rates (88%–92%), comparable morbidity to ERCP, and improved hospitalization metrics [6]. Abdelkader et al. [5] reported a 100% success rate in CBD stone clearance using SpyGlass compared to 89% with conventional ERCP, along with shorter hospital stays and lower complication rates.
Although the SpyGlass system entails significant equipment and training costs, the reduction in hospital stays and procedures may offset these expenses [5]. Open choledochotomy is now rarely used due to higher morbidity and invasiveness, and even laparoscopic choledochotomy involves T-tube drain placement and risk of bile leak or stricture formation [7].
The transcystic approach, particularly with SpyGlass assistance, avoids these complications. In difficult cases, a mini choledochotomy can still accommodate SpyGlass with reduced risk [7]. Notably, transcystic SpyGlass procedures avoid papillary trauma, reducing the incidence of postprocedural pancreatitis.
The clinical advantages of SpyGlass include
direct visualization: it enables precise localization and real-time monitoring of stone fragmentation and extraction [3].advanced lithotripsy: electrohydraulic and laser probes achieve 90%–95% success in complex stone fragmentation under direct vision [9].targeted biopsy: SpyBite® forceps allow in situ sampling of biliary lesions with higher diagnostic accuracy than traditional blind ERCP brushings [10].balloon sphincteroplasty: it facilitates stone passage while preserving the sphincter of Oddi, reducing bleeding and perforation risks [11].lower complication rates: by avoiding endoscopic manipulation and fluoroscopy, intraoperative transcystic exploration reduces the risks of pancreatitis and infection [10, 12].
In our case, complete ductal clearance was achieved without complication, consistent with the existing literature on SpyGlass-assisted transcystic exploration. No postoperative leaks, infections, or pancreatitis occurred.
Conclusion
SpyGlass-assisted transcystic bile duct exploration during laparoscopic cholecystectomy represents a safe, effective, and minimally invasive alternative to conventional two-stage ERCP plus surgery. This technique offers combined diagnostic and therapeutic capabilities in a single session, avoiding choledochotomy and minimizing ERCP-associated morbidity.
It is particularly well suited for high-risk or anatomically complex CBD stone cases, provided appropriate training and resources are available. Although further studies are needed to define its place in global clinical guidelines, current data and international algorithms increasingly support its integration into advanced biliary surgical practice (Fig. 3). Our findings further validate this approach as both clinically effective and safe.
New flowchart proposed for the management of patients at intermediate or high risk of choledocholithiasis due to the advent of new technologies such as SpyGlass.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang X, Yu W, Jiang G, et al. Global epidemiology of gallstones in the 21st century: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2024;22:1586–95. 10.1016/j.cgh.2024.01.05138382725 · doi ↗ · pubmed ↗
- 2Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut Liver 2012;6:172–87. 10.5009/gnl.2012.6.2.17222570746 PMC 3343155 · doi ↗ · pubmed ↗
- 3Fugazzola P, Bianchi CM, Calabretto F, et al. Intraoperative transcystic laparoscopic common bile duct stone clearance with Spy Glass™ Discover during emergency and elective cholecystectomy: a single-center case series. World J Emerg Surg 2024;19:8. 10.1186/s 13017-023-00529-038438899 PMC 10913229 · doi ↗ · pubmed ↗
- 4Ricci C, Pagano N, Taffurelli G, et al. Comparison of efficacy and safety of 4 combinations of laparoscopic and intraoperative techniques for management of gallstone disease with biliary duct calculi: a systematic review and network meta-analysis. JAMA Surg 2018;153:e 181167. 10.1001/jamasurg.2018.116729847616 PMC 6137518 · doi ↗ · pubmed ↗
- 5Abdelkader A, Basu S, Khalid AUA, et al. Laparoscopic transcystic Spy Glass Discover-assisted common bile duct exploration and clearance: an efficient and cost-effective alternative for common bile duct stone management. Cureus 2025;17:e 80398. 10.7759/cureus.80398 PMC 1198627440225425 · doi ↗ · pubmed ↗
- 6Silva HMD, Howard T, Bird D, et al. Outcomes following common bile duct exploration versus endoscopic stone extraction before, during and after laparoscopic cholecystectomy for patients with common bile duct stones. HPB (Oxford) 2022;24:2125–33. 10.1016/j.hpb.2022.08.01436130852 · doi ↗ · pubmed ↗
- 7Li Q, Ji J, Wang F, et al. ERCP-induced duodenal perforation successfully treated with endoscopic purse-string suture: a case report. Oncotarget 2015;6:17847–50. 10.18632/oncotarget.407926068948 PMC 4627350 · doi ↗ · pubmed ↗
- 8Chen L, Xia L, Lu Y, et al. Influence of periampullary diverticulum on the occurrence of pancreaticobiliary diseases and outcomes of endoscopic retrograde cholangiopancreatography. Eur J Gastroenterol Hepatol 2017;29:105. 10.1097/MEG.000000000000074427606949 · doi ↗ · pubmed ↗