Magnesium Sulfate-Induced Ophthalmoplegia: A Rare Postnatal Complication
Pranit Khandait, Himali Hatwar

TL;DR
A woman developed rare eye muscle weakness after magnesium sulfate treatment for eclampsia, highlighting the need to monitor for magnesium toxicity.
Contribution
This case report highlights ophthalmoplegia as a rare but important complication of magnesium sulfate therapy in postpartum patients.
Findings
The patient showed bilateral ophthalmoplegia, ptosis, and neck weakness due to elevated magnesium levels.
Symptoms resolved within 36 hours after discontinuing magnesium sulfate.
MRI and antibody tests ruled out other neurological conditions like myasthenia gravis.
Abstract
Magnesium sulfate (MgSO4) is widely used in managing eclampsia, but its neurological side effects are often overlooked. A 25-year-old woman with a second gravida pregnancy developed eclampsia in her third trimester and underwent an emergency cesarean section. In the immediate postoperative period, she presented with bilateral ophthalmoplegia, ptosis, and neck flexion weakness, though her pupillary reflexes remained intact. Initial concerns included myasthenia gravis and Miller-Fisher syndrome, but further investigations, including repetitive nerve stimulation (RNS), acetylcholine receptor (AChR), and muscle-specific kinase (MuSK) antibody testing, were negative. Three Tesla MRI brains with constructive interference in steady state (CISS) sequences of III, IV, and VI were normal, and laboratory results revealed elevated serum magnesium levels (5.5 meq/L). A diagnosis of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
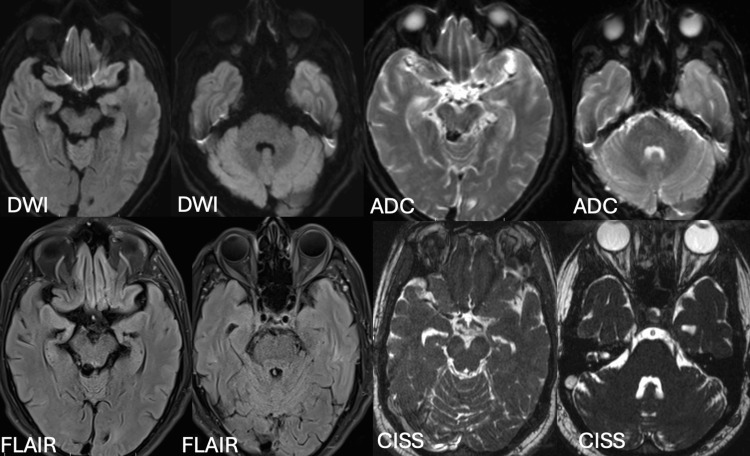 Figure 1
Figure 1| Parameter | Result | Reference range | Interpretation |
| Serum magnesium | 5.5 mEq/L | 1.5-2.5 mEq/L | Elevated |
| Serum creatinine | 0.7 mg/dL | 0.6-1.2 mg/dL | Normal |
| Blood urea | 11 mg/dL | 7-20 mg/dL | Normal |
| Total bilirubin | 0.9 mg/dL | 0.2-1.2 mg/dL | Normal |
| Conjugated bilirubin | 0.3 mg/dL | 0.0-0.3 mg/dL | Normal |
| SGPT (ALT) | 18 U/L | 7-56 U/L | Normal |
| SGOT (AST) | 15 U/L | 10-40 U/L | Normal |
| Total protein | 7.5 g/dL | 6.4-8.3 g/dL | Normal |
| Albumin | 3.9 g/dL | 3.5-5.0 g/dL | Normal |
| AChR antibody | <0.05 nmol/L | <0.25 nmol/L (negative) | Negative |
| MuSK antibody | <0.05 nmol/L | <0.05 nmol/L (negative) | Negative |
| CSF glucose | 55 mg/dL | 45-80 mg/dL (or 60-70% of blood glucose) | Normal |
| Corresponding blood glucose | 90 mg/dL | 70-110 mg/dL | Normal |
| CSF protein | 42 mg/dL | 15-45 mg/dL | Normal |
| CSF cell count | 2 cells/µL | 0-5 cells/µL | Normal |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMagnesium in Health and Disease · Neurosurgical Procedures and Complications · Amoebic Infections and Treatments
Introduction
Magnesium sulfate (MgSO_4_) is a widely used anticonvulsant in the management of preeclampsia and eclampsia due to its neuroprotective and vasodilatory properties. It acts as a calcium antagonist, reducing neuronal excitability and preventing seizures. However, its toxic effects, particularly at supra-therapeutic levels, can result in significant neuromuscular and cardiac complications. While respiratory depression and hypotension are well-documented, rare neurological manifestations such as ophthalmoplegia often go unrecognized. This report presents a rare case of MgSO_4_-induced bilateral ophthalmoplegia in a postpartum patient, shedding light on its pathogenesis and emphasizing the importance of early detection and management.
Case presentation
A 25-year-old female, gravida 2, at 36 weeks of gestation, presented with a one-week history of bilateral pedal edema, accompanied by a persistent, diffuse headache and intermittent episodes of visual blurring. These symptoms gradually intensified until, one day prior to admission, she experienced a generalized tonic-clonic seizure. At that time, her blood pressure was 164/90 mmHg, and proteinuria was present. This clinical deterioration led to a diagnosis of eclampsia.
In accordance with standard obstetric protocols, she was immediately started on an intravenous MgSO_4_ regimen following the Pritchard protocol - a regimen designed to achieve therapeutic magnesium levels that prevent recurrent seizures. Given the maternal risks and the need for rapid stabilization, an emergency lower-segment cesarean section was performed, and the renal function test was within normal limits (Table 1).
In the immediate postoperative period, the patient developed notable neurological symptoms. She had bilateral complete ptosis and ophthalmoplegia, characterized by a total restriction of eye movements. Her pupils remained reactive to light, indicating that parasympathetic innervation was largely spared. Additionally, she experienced mild weakness in neck flexion, absent knee-deep tendon reflexes, and a completely normal sensory examination.
Given the acute presentation of these neuromuscular deficits, the differential diagnosis initially included conditions such as myasthenia gravis, Miller-Fisher syndrome (a variant of Guillain-Barré syndrome), and brainstem stroke. However, extensive investigations, including brain MRI with constructive interference in steady state (CISS) sequence for cranial nerves III, IV, and VI, were normal (Figure 1).
MRI brain plain and CISS sequence within normal limitsDWI: diffusion-weighted imaging; ADC: apparent diffusion coefficient; FLAIR: fluid-attenuated inversion recovery; CISS: constructive interference in steady state
Repetitive nerve stimulation (RNS) at 3 Hz, conducted on the bilateral orbicularis oculi, bilateral nasalis, right-sided deltoid, anconeus, and abductor pollicis brevis (APB) muscles, was within normal limits. The absence of a decremental response on RNS testing, along with negative anti-acetylcholine receptor (anti-AChR) and anti-muscle-specific kinase (MuSK) antibody assays, effectively ruled out myasthenia gravis.
The above finding confirmed the diagnosis of hypermagnesemia-induced neuromuscular dysfunction, as described in Table 1. The excessive magnesium likely exerted its effects by competitively inhibiting calcium at presynaptic sites of the neuromuscular junction, thereby reducing acetylcholine release and leading to the observed neuromuscular blockade - a phenomenon that, while beneficial in preventing seizures, can result in adverse effects when magnesium accumulates. Recognizing the risk, MgSO_4_ therapy was immediately discontinued, and supportive care measures were instituted, including calcium gluconate.
Following these interventions, the patient’s clinical condition improved significantly. Within 24 hours, a noticeable improvement in her neuromuscular function was evident, and by 48 hours, both the ophthalmoplegia and ptosis had completely resolved as serum magnesium levels normalized to 2.5 mEq/L. The resolution of symptoms following the cessation of MgSO_4_ therapy confirmed the diagnosis of hypermagnesemia-induced ophthalmoplegia and underscored the reversibility of this condition when promptly managed.
The management of hypermagnesemia involves several critical steps. First, discontinuation of the MgSO_4_ infusion is essential to halt further accumulation. Intravenous hydration is then administered to enhance the renal excretion of magnesium. In cases where serum magnesium levels are dangerously high or significant neuromuscular blockade is present, calcium gluconate is used as an antidote to counteract the neuromuscular effects of magnesium. Serial monitoring of serum magnesium levels is vital to ensure they remain within the therapeutic range and to prevent further iatrogenic toxicity.
This case highlights not only the efficacy of MgSO_4_ in preventing eclamptic seizures but also the potential for serious, albeit reversible, neuromuscular complications when serum magnesium levels exceed the optimal range. It emphasizes the importance of careful patient monitoring, particularly in the postpartum period, and serves as a reminder of the delicate balance clinicians must maintain between therapeutic benefits and adverse effects in the management of eclampsia.
Discussion
MgSO_4_ is a mainstay in the management of preeclampsia and eclampsia due to its anticonvulsant properties, which are mediated by its action as a calcium channel antagonist. At therapeutic doses, MgSO_4_ helps to stabilize neuronal membranes by reducing calcium-mediated acetylcholine release at the neuromuscular junction [1]. However, when serum magnesium levels exceed the therapeutic range, patients may develop signs of neuromuscular blockade such as decreased deep tendon reflexes, generalized muscle weakness, and, in rare instances, cranial nerve dysfunction leading to ophthalmoplegia [2]. In the case presented, the patient’s serum magnesium level reached 5.0 meq/L, which induced bilateral ophthalmoplegia - an uncommon manifestation where the extraocular muscles are selectively affected, while pupillary responses remain intact. This differential sensitivity may be due to inherent variations in the neuromuscular junctions of extraocular versus other skeletal muscles [3].
The pathophysiology of magnesium toxicity is rooted in its ability to inhibit presynaptic calcium influx, thereby reducing neurotransmitter (acetylcholine) release at the neuromuscular junction [4]. Experimental studies have demonstrated that elevated magnesium levels can significantly impair neuromuscular transmission, accounting for the clinical presentation of muscle weakness and, in severe cases, respiratory depression. For serum magnesium levels of 4-6 mEq/L, patients may experience headache, drowsiness, and diminished deep tendon reflexes. At levels of 6-10 mEq/L, symptoms can progress to somnolence, hypocalcemia, absent deep tendon reflexes, hypotension, bradycardia, and ECG changes. When serum magnesium exceeds 10 mEq/L, muscle paralysis may occur, leading to flaccid quadriplegia, apnea and respiratory failure, complete heart block, and cardiac arrest [5]. Although hypermagnesemia typically presents with generalized neuromuscular symptoms, isolated cranial nerve involvement - such as ophthalmoplegia - has been documented in a few case reports, suggesting that certain muscle groups may be more vulnerable to magnesium’s effects [6]. Differential diagnoses in such cases include myasthenia gravis, Miller-Fisher syndrome, and brainstem stroke; however, the absence of decremental responses on RNS, normal imaging, and negative antibody testing help to rule out these conditions [7,8].
Current guidelines emphasize the importance of serial monitoring of serum magnesium levels during MgSO_4_ therapy, especially in patients with risk factors like renal impairment, to prevent toxicity [9]. Management of magnesium toxicity primarily involves the prompt discontinuation of MgSO_4_, supportive care such as intravenous hydration, and, in severe cases, the administration of calcium gluconate to antagonize magnesium’s neuromuscular effects [10]. Early recognition and intervention are critical, as illustrated in this case, where the timely cessation of MgSO_4_ led to rapid clinical improvement and complete resolution of symptoms within 48 hours. This report, therefore, underscores the need for heightened clinical vigilance and strict adherence to monitoring protocols during MgSO_4_ administration to balance its therapeutic benefits against the risk of toxicity, even in patients with no identifiable risk factors for MgSO_4_ toxicity.
Conclusions
Hypermagnesemia-induced ophthalmoplegia, though rare, should be recognized as a potential complication of IV MgSO_4_ therapy in postpartum patients. Timely identification, discontinuation of MgSO_4_, and supportive management lead to rapid symptom resolution. Routine serum magnesium monitoring is crucial to balance the benefits of MgSO_4_ therapy with the risk of toxicity. Clinicians should maintain a high index of suspicion for magnesium-induced neuromuscular dysfunction in patients presenting with unexplained cranial nerve deficits.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Magnesium sulfate for the treatment of eclampsia: a brief review Stroke Euser AG Cipolla MJ 116911754020091921149610.1161/STROKEAHA.108.527788 PMC 2663594 · doi ↗ · pubmed ↗
- 2Cathartic-induced magnesium toxicity during overdose management Ann Emerg Med Jones J Heiselman D Dougherty J Eddy A 12141218151986375265410.1016/s 0196-0644(86)80870-8 · doi ↗ · pubmed ↗
- 3Neuroophthalmologic effects of intravenous magnesium sulfate Am J Obstet Gynecol Digre KB Varner MW Schiffman JS 184818521199010.1016/0002-9378(90)90763-w 2256494 · doi ↗ · pubmed ↗
- 4Magnesium sulfate and its versatility in anesthesia: a comprehensive review Cureus Dahake JS Verma N Bawiskar D 016202410.7759/cureus.56348 PMC 1102184838633961 · doi ↗ · pubmed ↗
- 5Hypermagnesemia Stat Pearls [Internet] Cascella M Vaqar S Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 549811/31747218 · pubmed ↗
- 6Magnesium and human health: perspectives and research directions Int J Endocrinol Al Alawi AM Majoni SW Falhammar H 904169420182018 https://doi.org/10.1155/2018/90416942984962610.1155/2018/9041694 PMC 5926493 · doi ↗ · pubmed ↗
- 7Miller Fisher syndrome Stat Pearls [Internet] Rocha Cabrero F Morrison EH Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 507717/29939539 · pubmed ↗
- 8An update on the importance of monitoring serum magnesium in advanced disease patients Curr Opin Support Palliat Care Centeno C López Saca JM 396405720132412692110.1097/SPC.0b 013e 32836575 e 3 · doi ↗ · pubmed ↗