Genetic Abnormalities in the Diagnosis and Treatment of Childhood Acute Myeloid Leukemia: A Prospective Study at Hue Central Hospital, Vietnam
Hoa Thi Kim Nguyen, Hao Kiem Tran, Viet Hung Phan, Son Binh Bao Bui

TL;DR
This study examines genetic abnormalities in childhood AML in Vietnam and their impact on diagnosis, treatment, and prognosis.
Contribution
The study identifies specific genetic fusions in childhood AML and their association with treatment outcomes in a Vietnamese cohort.
Findings
34.3% of patients had genetic abnormalities, including AML1/ETO, PML/RARA, and MLL/AF6 fusions.
Genetic risk groups correlated with remission rates but not with relapse or survival rates.
Supportive care and non-genetic factors significantly influence treatment outcomes in childhood AML.
Abstract
Background: Genetic tests are important in the classification, treatment, and prognosis of acute myeloid leukemia (AML). The present study aimed to detect genetic abnormalities and investigate the correlation between gene abnormalities and the treatment results of childhood AML. Methods: A descriptive cross-sectional study of 35 children with de novo AML was established between 2017 and 2022 at Hue Central Hospital, Vietnam. Parameters of age, gender, gene fusions, remission, relapse rate, and survival rates were investigated. Results: The male-to-female ratio was 1.92:1. The mean age was 7.3±4.9 years. The multiplex reverse transcription polymerase chain reaction (RT-PCR) using the HemaVision 28N kit test results showed that 12 (34.3%) patients had genetic abnormalities, of which five (14.2%) patients had AML1/ETO fusion, three (8.6%) had PML/RARA fusion, two (5.7%) had MLL/AF6…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
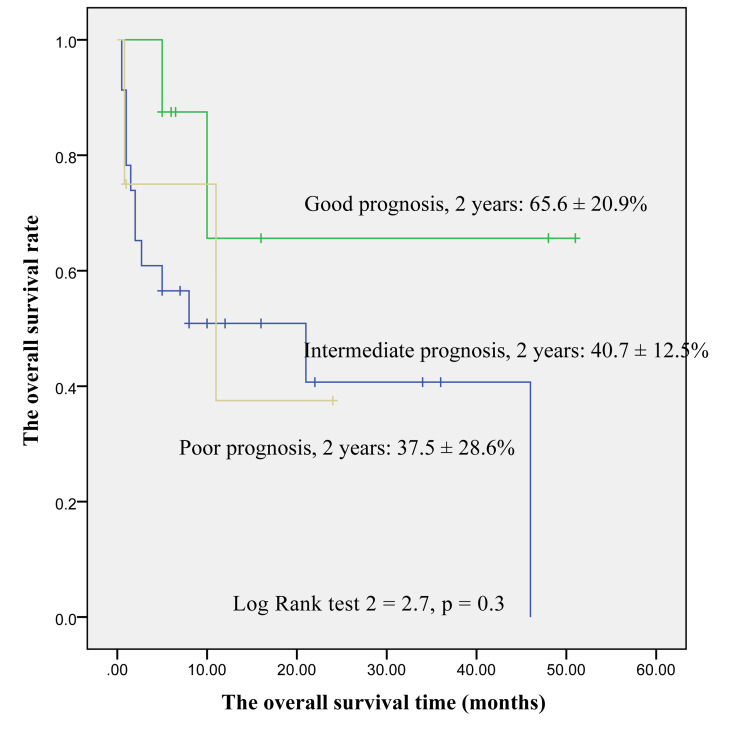 Figure 1
Figure 1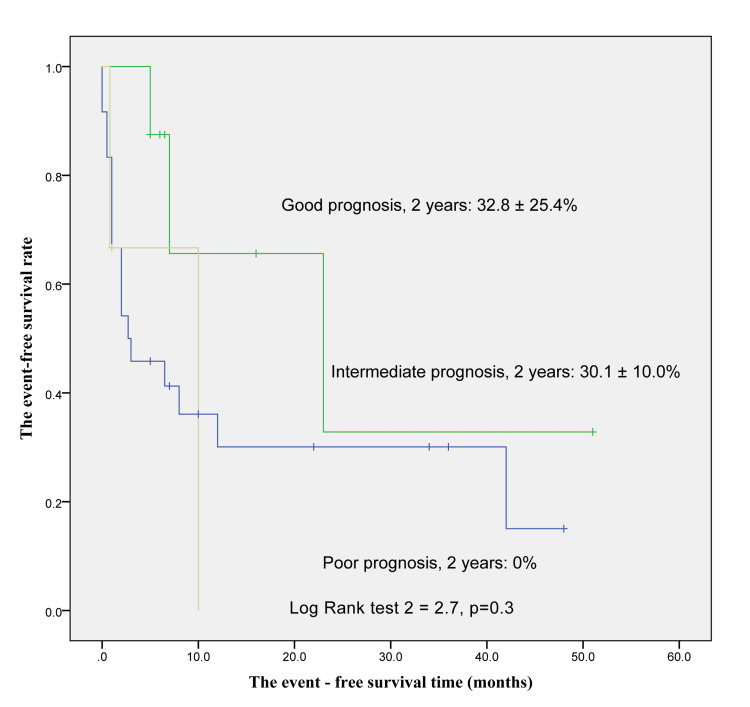 Figure 2
Figure 2| Drugs | Dose and regimen |
| Induction phase | |
| Cytarabine | 100 mg/m2/day×7 days |
| Daunorubicin | 45 mg/m2/day×3 days |
| BMA at day 14: If the patient does not achieve remission, blast cells > 20% | |
| Cytarabine | 2000 mg/m2/12 hours×6 days |
| BMA at day 14: If the patient does not achieve remission: 5% < blast cells < 20% | |
| Cytarabine | 100 mg/m2/day×7 days |
| Daunorubicin | 45 mg/m2/day×3 days |
| Intensification 1 | |
| Cytarabine | 1000 mg/m2/12 hours×4 days |
| Daunorubicin | 45 mg/m2×3 days |
| Intensification 2 | |
| Cytarabine | 1000 mg/m2/12 hours×4 days |
| Etoposide | 100 mg/m2/day×4 days |
| Intensification 3: Repeat intensification 1 or | |
| Cytarabine | 3000 mg/m2/12 hours×3 days |
| For AML-M3 | |
| Induction phase | |
| ATRA | 25 mg/m2/day |
| Daunorubicin | 45 mg/m2/day×3 days |
| Consolidation (2-3 episodes) | |
| Daunorubicin | 45 mg/m2/day×3 days |
| Cytarabine | 1000 mg/m2/12 hours×4 days |
| Maintenance for two years | |
| ATRA | 25 mg/m2/day |
| MTX | 15 mg/m2/week |
| Purinethol | 75 mg/m2/day |
| Gene fusions | Number (%) |
| AML1/ETO–t(8;21)(q22;q22) | 5 (14.2) |
| AML1/ETO+BCR/ABL1 | 1 (2.9) |
| PML/RARA–t(15;17)(q22; q22) | 3 (8.6) |
| MLL/AF6–t(6;11)(q27;q23) | 2 (5.7) |
| KMT2A/MLLT10–t(10;11)(p12;q23) | 1 (2.9) |
| Unexpressed | 23 (65.7) |
| Total | 35 (100) |
| Classified group according to gene fusions | Number (%) |
| Poor prognosis (MLL/AF6, KMT2A/MLLT10, BCR/ABL1+AML1/ETO) | 4 (11.4) |
| Intermediate prognosis | 23 (65.7) |
| Good prognosis (AML1/ETO, PML/RARA) | 8 (22.9) |
| Total | 35 (100) |
| The status of remission | Number (%) |
| Remission | 19 (54.3) |
| Partial remission | 4 (11.4) |
| No remission | 3 (8.6) |
| Death | 9 (25.7) |
| Total | 35 (100) |
| The status of remission | Poor prognosis group | Intermediate prognosis group | Good prognosis group | P-value |
| N (%) | N (%) | N (%) | ||
| Remission | 1 (25) | 10 (43.5) | 8 (100) | 0.03* |
| Partial remission | 2 (50) | 2 (8.7) | - | |
| No remission | - | 3 (13) | - | |
| Death | 1 (25) | 8 (34.8) | - | - |
| Total | 4 (100) | 23 (100) | 8 (100) | - |
| Risk group (relapse status) | Poor prognosis | Intermediate prognosis | Good prognosis | P-value |
| N (%) | N (%) | N (%) | ||
| No relapse | 1 (33.3) | 7 (58.3) | 5 (71.4) | 0.8 |
| Relapse | 2 (66.7) | 5 (41.7) | 2 (28.6) | |
| Total | 3 (100) | 12 (100) | 7 (100) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Acute Lymphoblastic Leukemia research · Retinoids in leukemia and cellular processes
Introduction
Acute myeloid leukemia (AML) is a malignant clonal disorder of hematopoietic progenitor cells characterized by uncontrolled proliferation, impaired differentiation, and accumulation of immature myeloid cells in the bone marrow and peripheral blood. It accounts for approximately 15-20% of pediatric leukemias and remains a significant therapeutic challenge due to its aggressive clinical course and high relapse rates [1-3]. Genetic abnormalities play a central role in the pathogenesis, classification, and prognosis of AML. Specific chromosomal translocations such as t(8;21), inv(16), and t(15;17) are associated with favorable prognoses and are categorized as low-risk. Conversely, abnormalities like monosomy 7, FLT3-ITD, and complex karyotypes are often linked with poor outcomes and classified as high-risk [4]. The most recent World Health Organization (WHO) classification (2022) integrates genetic profiles as a central element in AML diagnosis, underscoring their prognostic significance and therapeutic implications [5]. To detect these abnormalities, genetic testing has become an integral component of AML workup. Techniques such as cytogenetics, fluorescence in situ hybridization (FISH), and polymerase chain reaction (PCR) allow for the precise identification of fusion genes and other pathogenic mutations. In Vietnam, genetic tests on AML patients are carried out at a number of large centers, with the test being used to detect four types of common gene fusions using the reverse transcription (RT)-PCR technique. The Pediatric Center of Hue Central Hospital was established in 2013 on the basis of the original pediatric department. Children with blood cancer have been treated in Hue since 2005 [6]. However, until 2018, the Pediatric Center of Hue Central Hospital could do multiplex RT-PCR using the HemaVision 28N kit genetic analysis for AML patients. In addition to molecular characteristics, demographic factors such as age and gender have been investigated in the literature for their potential association with treatment outcomes in AML. However, our study did not evaluate age or gender in relation to the clinical endpoint. Instead, we focused specifically on exploring the correlation between genetic risk classification and treatment outcomes.
This study aims to detect genetic abnormalities and assess the relationship between genetic risk groups, identified using the HemaVision 28N RT-PCR panel and key treatment responses, including complete remission (CR) after induction, relapse, overall survival (OS), and event-free survival (EFS) in pediatric patients diagnosed with AML at Hue Central Hospital. By strengthening the understanding of molecular risk factors in this context, we hope to contribute to improved stratification and management strategies for childhood AML in Vietnam.
Materials and methods
All patients underwent multiplex RT-PCR using the HemaVision 28N kit. A DNA diagnostic RT-PCR assay is capable of identifying 28 recurrent chromosomal translocations and over 145 clinically relevant fusion transcripts associated with hematologic malignancies. The test employs a nested RT-PCR design to enhance sensitivity and specificity, making it a reliable method for rapid profiling and risk stratification in pediatric AML cases.
The study materials included 35 children diagnosed with AML treated at the Pediatric Center of Hue Central Hospital with the AML protocol (Table 1) between November 2017 and May 2022.
Inclusion criteria were as follows: patients diagnosed with AML and treated with the AML protocol (Table 1), those aged <16, and all patients who underwent multiplex RT-PCR using the HemaVision 28N kit genetic analysis and with 28 basic genetic mutations in AML detected.
Criteria for the diagnosis of AML included clinical features, the results of bone marrow morphology, where the leukemic blasts were counted for equal or more than 20% in the marrow space, and immune markers consistent with AML.
Exclusion criteria were as follows: pediatric patients with secondary or relapsed AML and cases where the child and the representative did not agree to participate in the study.
Data were analyzed according to genetic tests, the remission rate, the relapse rate, and the OS and EFS rates. All statistical analysis was performed using IBM SPSS Statistics for Windows, Version 18.0 (Released 2019; IBM Corp., Armonk, New York, United States).
Ethical approval
This study was approved by the Hue Central Hospital Ethics Committee on October 20, 2017, with the approval number 18/NCKH-BVH for both research on AML and acute lymphoblastic leukemia [6]. Consent was obtained from all participants' parents or guardians in this study.
Results
Among 35 new AML patients, there were 23 males and 12 females; the male-to-female ratio was 1.92:1. The mean age was 7.3±4.9 years. There was no age peak in disease incidence, which increased slightly after the first year of age. Regarding the classification of AML subtypes, M2 and M5 accounted for the highest percentages, 10 (28.6%) for each subtype. The percentages of M6, M3, M1, M0, and M7 were 5 (14.3%), 4 (11.4%), 3 (8.6%), 2 (5.7%), and 1 (2.8%), respectively.
The results of multiplex RT-PCR using the HemaVision 28N kit showed that 12 (34.3%) patients had genetic abnormalities, of which five (14.2%) had AML1/ETO fusion, three (8.6%) had PML/RARA fusion, two (5.7%) had MLL/AF6 fusion, one (2.9%) had KMT2A/MLLT10 fusion, and one (2.9%) had AML1/ETO and BCR/ABL1 fusion (Table 2).
The prognostic grouping according to genetic mutation was as follows: good prognosis 8 (22.9%), intermediate prognosis 23 (65.7%), and poor prognosis 4 (11.4%) (Table 3). Fusion genes play a role in the classification of AML subtypes. Patients with PML/RARA gene fusion were classified as an M3 subtype. Patients with the AML1/ETO gene fusion were mainly in the M2 subtype, and patients with KMT2A/MLLT10 gene fusion were in the M5 subtype.
In the evaluation after the induction phase, the results showed that 19 (54.3%) patients achieved remission, four (11.4%) patients had partial remission, and three (8.6%) patients did not. Moreover, nine (25.7%) patients died during the induction phase (Table 4). The remission rates of people with poor, intermediate, and good prognosis groups were 25%, 43.5%, and 100%, respectively. There was a statistically significant correlation between genetic abnormalities and the remission rate (p=0.03) (Table 5). We used Fisher's exact test because of the small samples.
When evaluating the AML relapse rate according to genetic risk groups, the results showed no correlation between them (p=0.8). The relapse rates for patients with poor, intermediate, and good prognosis groups were 66.7%, 41.7%, and 28.6%, respectively (Table 6).
Regarding the evaluation of the survival rate according to the genetic risk group, the result showed that at the end of the study, out of a total of 35 AML patients, there were 17 patients who had died. The number of surviving patients was 18 (51.4%).
At two years, the poor prognosis group had an OS rate of 37.5±28.6%, and the figures for the intermediate and favorable prognosis groups were 40.7±12.5% and 65.6±20.9%, respectively. However, the difference was not statistically significant (p=0.3) (Figure 1). In the second year, the EFS rates of people experiencing poor, intermediate, and good prognostic groups were 0%, 30.1±10.0%, and 32.8±25.4%, respectively. This difference was not statistically significant (p=0.3) (Figure 2).
The overall survival rate for AML patientsAML: acute myeloid leukemia
The event-free survival rate for AML patientsAML: acute myeloid leukemia
Discussion
The observed male predominance (M:F=1.92:1) in our cohort is consistent with previous studies [5,6]. However, gender is not currently considered an independent risk factor for AML incidence or outcome, and this difference may result from population-based variation or chance [7,8]. The mean age was 7.3±4.9 years, similar to some studies by Juliusson et al. and Deschler and Lübbert [9,10]. Regarding the classification of AML subtypes, M2 and M5 accounted for the highest percentages (28.6% for each subtype), which was similar to the results of Pui's and Shahab and Raziq's studies [7,11].
The results of the multiplex RT-PCR test using the HemaVision 28N kit showed that there were 34.3% of patients with genetic abnormalities, including 14.2% of patients with AML1/ETO, 8.6% of patients with PML/RARA, 5.7% of patients with MLL/AF6, 2.9% of patients with KMT2A/MLLT10, and 2.9% of patients with AML1/ETO and BCR/ABL1 fusion. A new point in our result was that one patient had two fusion genes: AML1/ETO and BCR/ABL1. This was a special case and was reported for the first time in Vietnam. For AML patients, the presence of the BCR/ABL1 fusion gene is rare [12]. The combination of AML1/ETO and BCR/ABL1 is extremely rare. According to foreign literature, there are a few cases having AML1/ETO and BCR/ABL1. And these patients will have a poor prognosis [13]. Besides that, our result also found two fusion genes (MLL/AF6 and KMT2A/MLLT10) which have not been reported in Vietnamese children yet. According to Quessada et al.'s research, the percentages of two gene fusions, MLL/AF6 and KMT2A/MLLT10, were 1-2% and 2-3%, respectively [8]. These mutations are associated with MLL rearrangement and have a poor prognosis. Therefore, detecting gene fusions in AML is critically important for accurate risk stratification, prognosis, and guiding therapeutic decisions.
Based on genetic abnormalities, Quessada et al., Rubnitz and Inaba, and Pui et al. classified patients into three risk genetic groups: favorable, intermediate, and poor prognosis [8,14,15]. In our result, there were 22.9% of patients with a good prognosis, 65.7% of patients with an intermediate prognosis, and 11.4% of patients with a poor prognosis.
The rate of remission after the induction phase for AML was 54.3%; 11.4% of patients had partial remission, and 8.6% of patients did not achieve remission. There, 25.7% of patients passed away during the induction phase. The rate of remission in our study was lower than that of Waack et al.'s study and Bui et al.'s study rates of 84.7% and 89.4%, respectively [16,17]. This issue reflected that supportive care plays an important role in AML treatment. The infection rate was still high in my hospital, and it caused failure in treatment for childhood AML. And we need to improve. The successful treatment for AML patients is still limited; therefore, numerous new therapeutic strategies have been developed globally to improve treatment outcomes for pediatric AML patients [18]. Regarding the correlation between genetic abnormalities and the rate of remission in childhood AML, there was a statistically significant correlation between them (p=0.03). The rates of remission in poor, intermediate, and good prognosis groups were 25%, 43.5%, and 100%, respectively. The results of the present study regarding the remission rate were consistent with findings from previous studies conducted by Pui, Rubnitz and Inaba, and Singh et al., which also reported higher remission rates in patients with AML1/ETO and PML/RARA fusion genes [13-15]. These studies showed that AML1/ETO and PML/RARA were associated with favorable prognoses and PML/RARA had a good response with all-trans retinoic acid (ATRA) drug, while MLL/AF6 mutation was associated with a poor prognosis and a lower remission rate. The combined existence of BCR/ABL1 and AML1/ETO gene fusion had a poor prognosis, even if the patient carried AML1/ETO gene fusion, which was associated with a good prognosis [13-15].
The relapse rates of the poor, intermediate, and good prognosis groups were 66.7%, 41.7%, and 28.6%, respectively. The difference did not have statistical significance (p=0.8). In AML treatment, multiple factors can influence the relapse rate aside from gene fusions. These include high infection rates during intensive chemotherapy, delayed treatment intervals due to supportive care limitations [17], the patient's pre-transplant condition, minimal residual disease (MRD) status, cytogenetic complexity, and AML subtype such as M4/M5 [19,20]. With the use of intensive chemotherapy, the infection rate was high. Prolonged infections will delay treatment time for patients, affecting treatment results and relapse rates. Therefore, supportive care in AML plays an important role. According to Harris et al., there are some factors that predict relapse in AML after transplant: the condition of the bone marrow and the patient before transplant, genetic abnormalities, and subtype M4/M5 [19].
The OS rates after two years for childhood AML with poor, intermediate, and favorable prognosis risk groups were 37.5±28.6%, 40.7±12.5%, and 65.6±20.9%, respectively. The difference was not statistically significant (p=0.3). The EFS rates for people experiencing poverty, intermediate, and favorable prognosis risk groups after two years were 0%, 30.1±10.0%, and 32.8±25.4%. However, there is no statistical difference (p=0.2).
Our results differed from the studies by Cho et al., Pui et al., and Rubnitz and Inaba, who illustrated that there was a correlation between the genetic risk group and overall EFS [14,15,20]. AML treatment is so complicated, and supportive care plays an important role in controlling infection and reducing mortality is very necessary. In our hospital, the present study did not have isolated rooms for childhood AML patients, and supportive care had some limitations. So, the result had some differences. The present study should improve the quality of AML treatment as soon as possible.
In our research, the present study had some limitations because it did a genetic test but did not perform chromosome analysis, so the classification could be missed. In the future, the present study should combine genetic tests and chromosome analysis tests to classify genetic risk groups for childhood AML patients.
Conclusions
This study highlights the critical role of genetic abnormalities in the classification, prognosis, and initial treatment response in childhood AML. A statistically significant correlation was observed between genetic risk groups and remission rates, reinforcing the value of molecular diagnostics in risk stratification and treatment planning. However, no significant associations were found between genetic risk and relapse rate, OS, or EFS. These findings underscore the multifactorial nature of AML treatment outcomes, especially in resource-limited settings. Inadequate supportive care, particularly in managing infections, may contribute significantly to treatment failure and mortality. Therefore, in addition to advancing genetic diagnostics, enhancing supportive care infrastructure remains essential to improving long-term outcomes for children with AML in Vietnam and similar settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The leukemias: a half-century of discovery J Clin Oncol Freireich EJ Wiernik PH Steensma DP 346334693220142518509310.1200/JCO.2014.57.1034 · doi ↗ · pubmed ↗
- 2Acute lymphoblastic leukaemia Lancet Inaba H Greaves M Mullighan CG 1943195538120132352338910.1016/S 0140-6736(12)62187-4PMC 3816716 · doi ↗ · pubmed ↗
- 3Collaborative efforts driving progress in pediatric acute myeloid leukemia J Clin Oncol Zwaan CM Kolb EA Reinhardt D 294929623320152630489510.1200/JCO.2015.62.8289 PMC 4567700 · doi ↗ · pubmed ↗
- 4A comprehensive analysis of cytogenetics, molecular profile, and survival among pediatric acute myeloid leukemia: a prospective study from a tertiary referral center Am J Blood Res Meena JP Makkar H Gupta AK 177189122022 https://pmc.ncbi.nlm.nih.gov/articles/PMC 9890188/pdf/ajbr 0012-0177.pdf 36742278 PMC 9890188 · pubmed ↗
- 5The 5th edition of the World Health Organization classification of haematolymphoid tumours: myeloid and histiocytic/dendritic neoplasms Leukemia Khoury JD Solary E Abla O 170317193620223573283110.1038/s 41375-022-01613-1PMC 9252913 · doi ↗ · pubmed ↗
- 6Research of genetic abnormalities in diagnosis and treatment of childhood acute lymphoblastic leukemia at Hue Central Hospital Ann Clin Anal Med Tran HK Nguyen HTK Phan VH 2124152024
- 7Clinical presentations of acute leukemia J Coll Physicians Surg Pak Shahab F Raziq F 472476242014 https://pubmed.ncbi.nlm.nih.gov/25052968/25052968 · pubmed ↗
- 8Cytogenetics of pediatric acute myeloid leukemia: a review of the current knowledge Genes (Basel) Quessada J Cuccuini W Saultier P Loosveld M Harrison CJ Lafage-Pochitaloff M 9241220213420435810.3390/genes 12060924 PMC 8233729 · doi ↗ · pubmed ↗