Effect of Biologic Therapies in Treating Moderate-to-Severe Ulcerative Colitis: A Systematic Review and Meta-Analysis
Ooha Thadiboina, Syed Saim Ali Shah, Rubela Ray, Sarah A Hack, Mahpara Munir, Qalandar Shah, Amritveer Bhullar, Syed Zargham Hussain Shah, Mohammed Abdul Muhaimin Ali, Uzma Nureen, Sana Afzal, Izzat Izzat

TL;DR
This study reviews and combines data from multiple trials to show that biologic therapies are effective in treating moderate-to-severe ulcerative colitis.
Contribution
The study provides a comprehensive meta-analysis comparing the efficacy of biologic agents in treating UC.
Findings
Biologics significantly improved clinical response rates compared to placebo.
They also increased remission and mucosal healing rates in UC patients.
High heterogeneity was observed across most outcomes.
Abstract
Biological therapies have emerged as effective treatments for moderate-to-severe ulcerative colitis (UC). This systematic review and meta-analysis aimed to assess the efficacy of different biologic agents for inducing clinical response, remission, and mucosal healing in patients with moderate-to-severe UC. A systematic literature search was conducted in PubMed, Excerpta Medica database (EMBASE), and Cochrane Library from inception to February 2025. Randomized controlled trials (RCTs) and prospective cohort studies evaluating biologics in adults with moderate-to-severe UC were included. The primary outcomes were clinical response, clinical remission, and mucosal healing. Random-effects meta-analyses were performed to calculate pooled effect estimates. Forty-three studies were included. Biologics were significantly more effective than placebo for inducing clinical response rates (odds…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
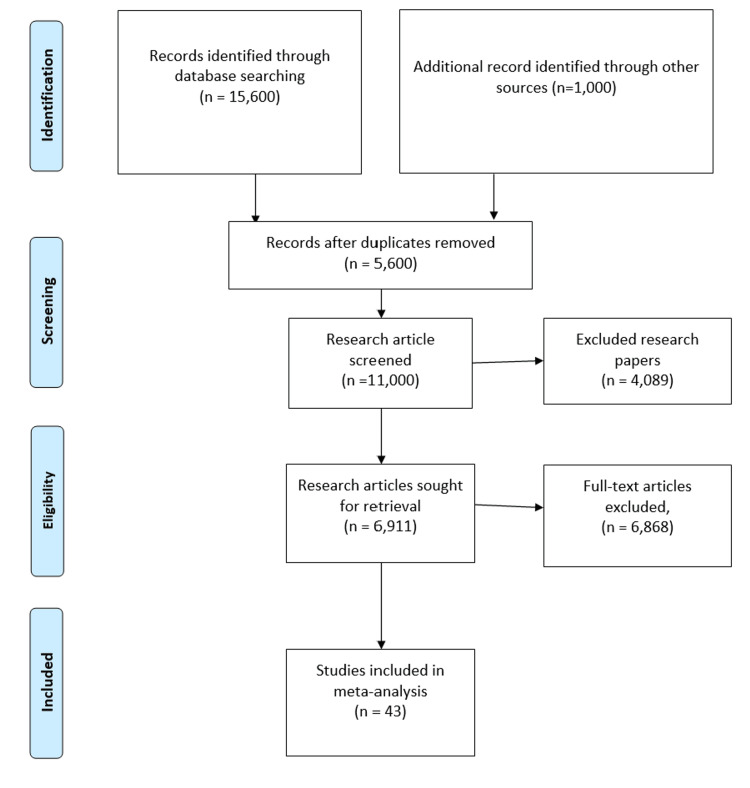 Figure 1
Figure 1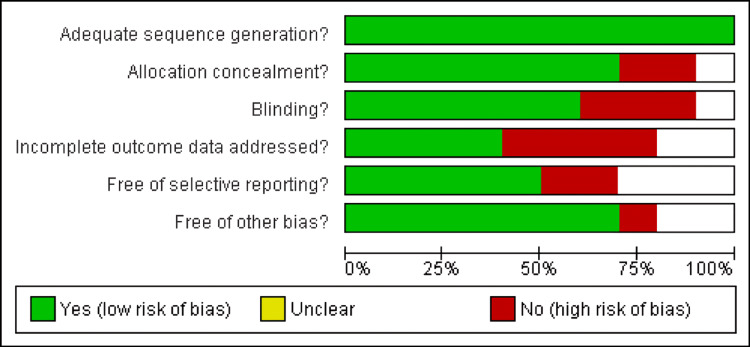 Figure 2
Figure 2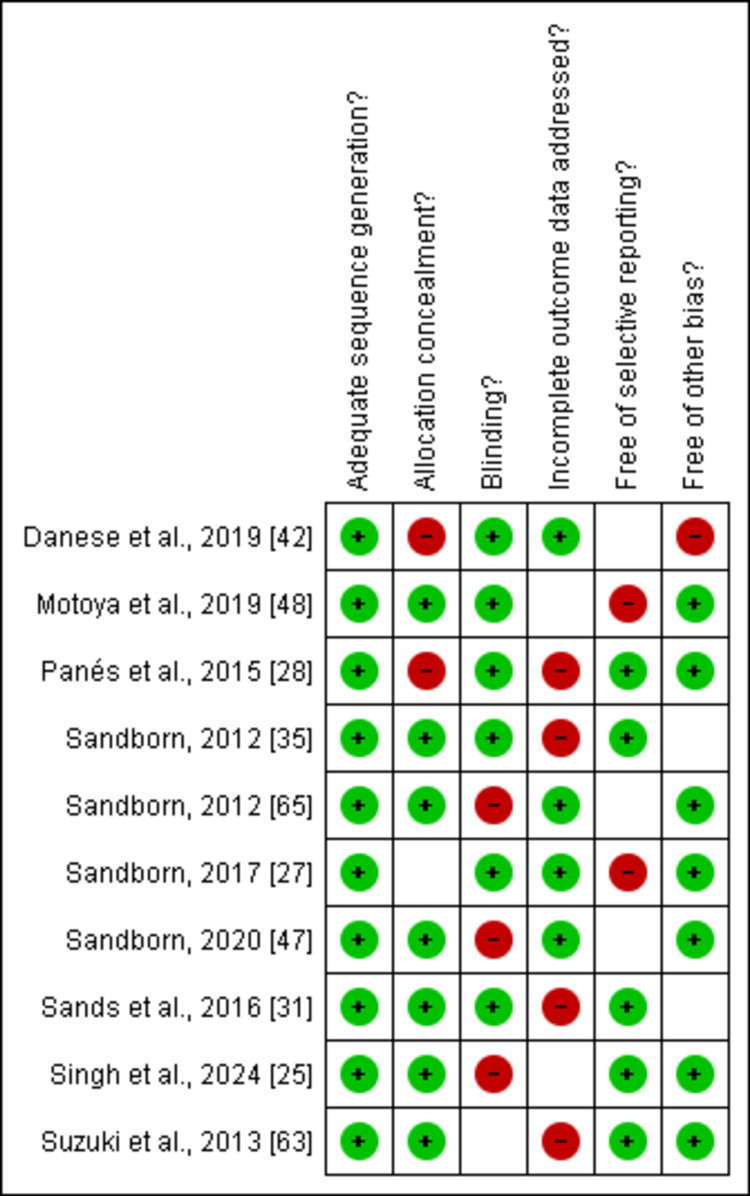 Figure 3
Figure 3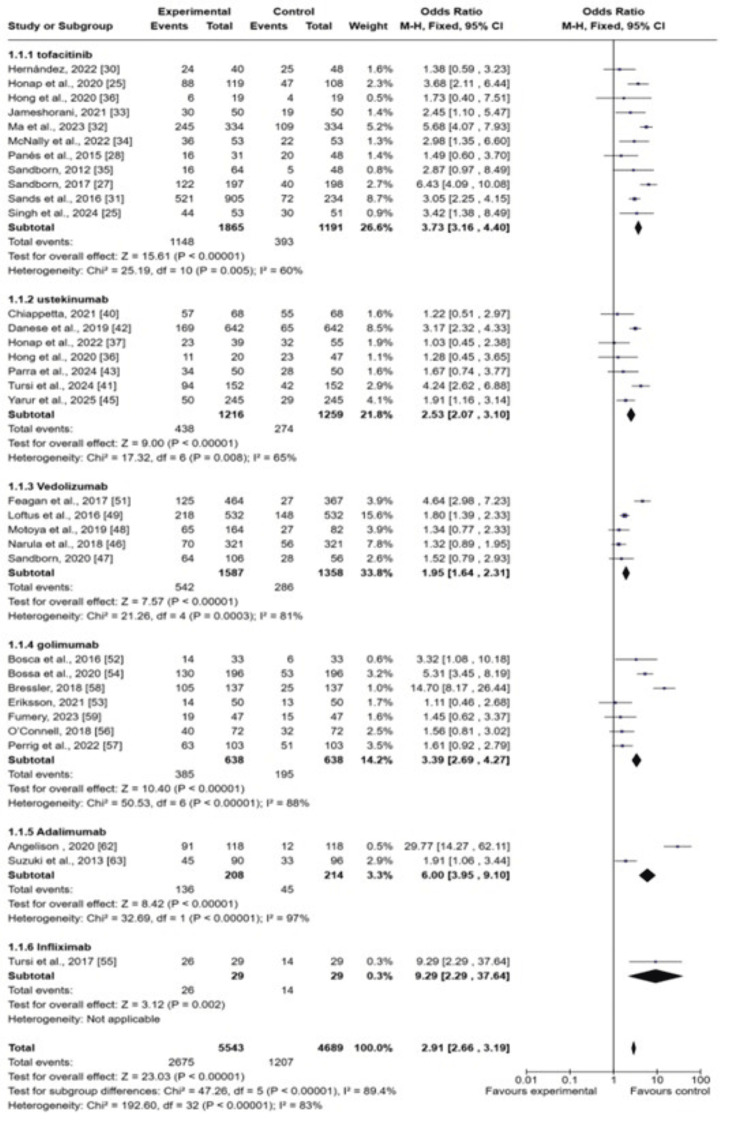 Figure 4
Figure 4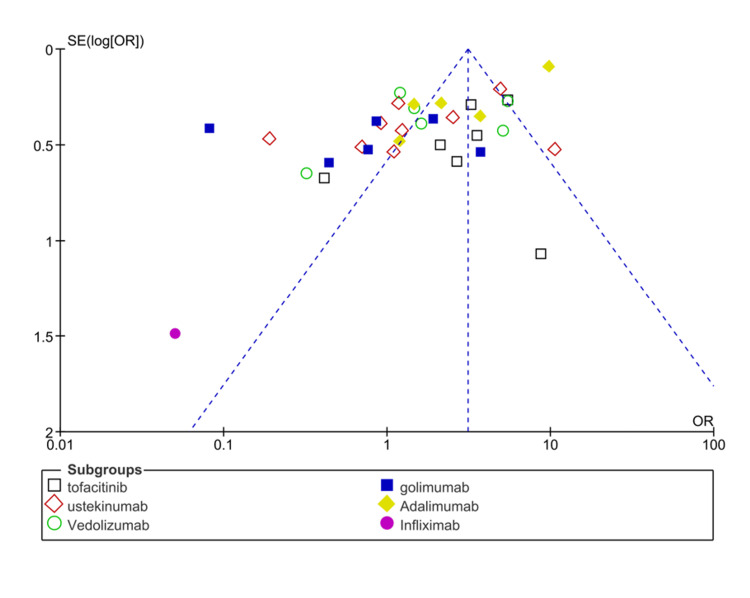 Figure 5
Figure 5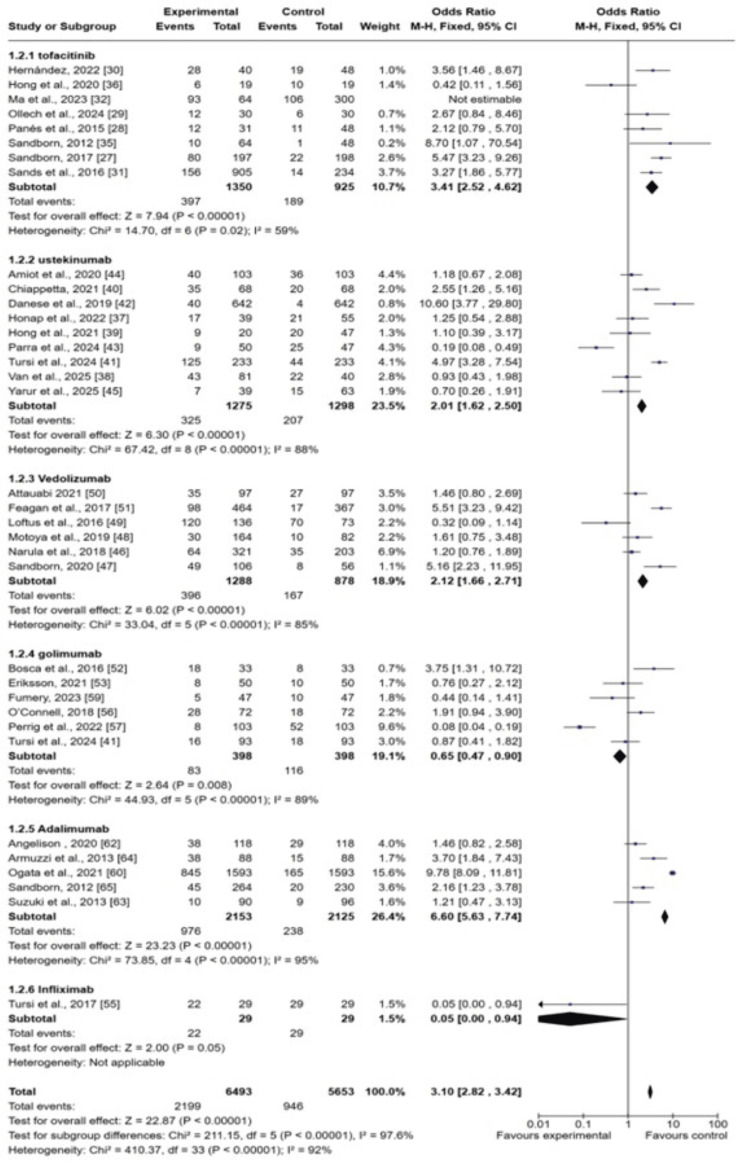 Figure 6
Figure 6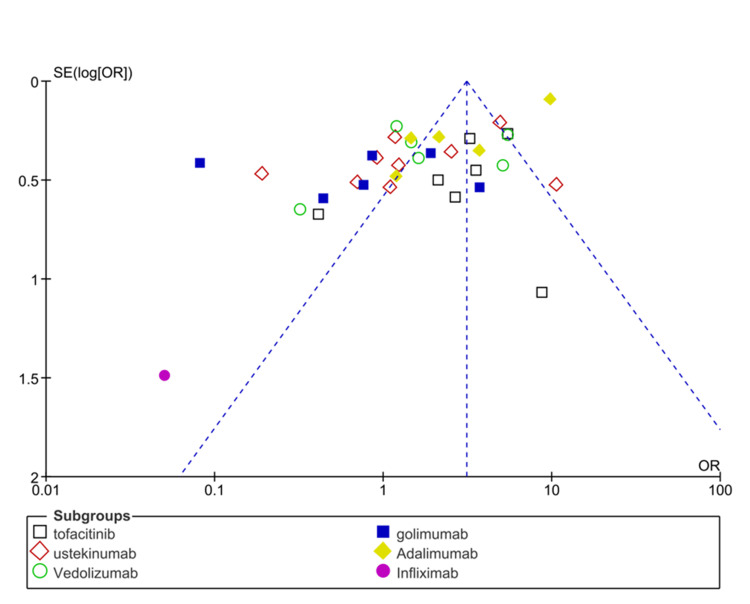 Figure 7
Figure 7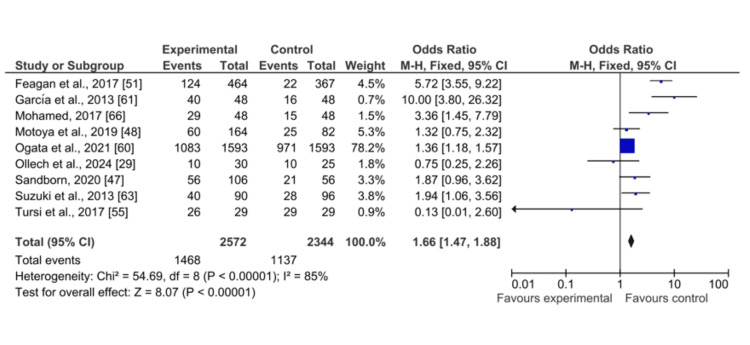 Figure 8
Figure 8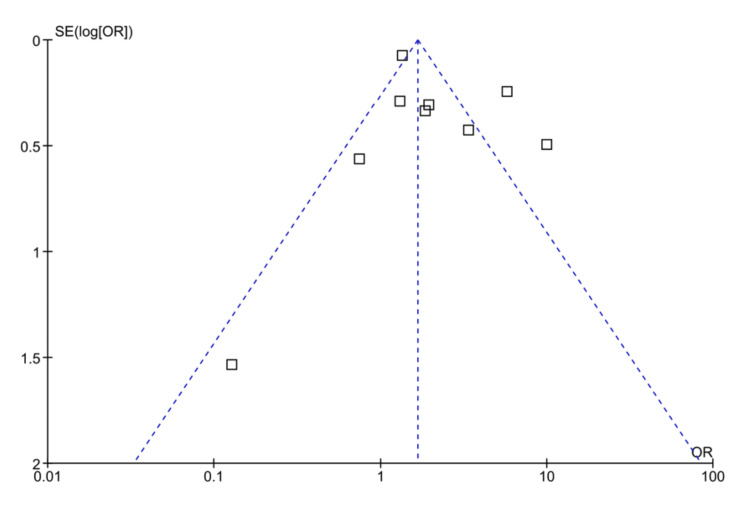 Figure 9
Figure 9| Author, year | Country | Study population (mean age in years) | Median follow-up | Study design | Drug used | Mucosal healing | Response rates | Clinical remission rates |
| Honap et al., 2020 [ | United Kingdom | 134 patients with UC (37 years) | 26 weeks | Multicenter prospective cohort | Tofacitinib | Pre: 88/119, Post: 47/108 | ||
| Singh et al., 2024 [ | India | 104 patients with UC (37.5 years) T: 53 P: 51 | 90 days | Randomized controlled trial | Tofacitinib (10 mg thrice daily) | T: 44/53, P: 30/51 | ||
| Sandborn et al., 2017 [ | United States | 593 patients with UC (39.5 years), T: 197, P: 198 | 52 weeks | Phase 3, randomized-controlled study | Tofacitinib (10 mg thrice daily) | T; 122, P; 40 | T: 80, P: 22 | |
| Panés et al., 2015 [ | Spain | 194 patients with UC, 3T: 31, P: 48 | 8 weeks | Phase 3, randomized-controlled study | Tofacitinib (10 mg thrice daily) | T: 16, P: 20 | T: 12, P: 11 | |
| Ollech et al., 2024 [ | Israel | 30 adult patients (26.3 years) | Prospective real-world study | Tofacitinib | T: 10/30, P: 10/25 | T: 12, P: 6 | ||
| Hernández Martínez et al., 2022 [ | Spain | 74 patients (45.4 years), T: 40, P: 48 | 19 months | Retrospective and multicenter observational study | Tofacitinib | T: 24, P: 25 | T: 28, P: 19 | |
| Sands et al., 2016 [ | United States | 1139 patients with UC (39.8 years), T: 905, P: 234 | 8 weeks | Randomized controlled trial | Tofacitinib 10 mg | T: 521, P: 72 | T: 156, P: 14 | |
| Ma et al., 2023 [ | Canada | 334 patients with UC | 52 weeks | Prospective cohort study | Tofacitinib 10 mg | T: 245, P: 109 | T: 64/93, P: 106/300 | |
| Jameshorani et al., 2021 [ | Iran | 50 patients with UC (40.5 years) | 52 weeks | Prospective cohort study | Tofacitinib 10 mg | T: 30, P: 19 | ||
| McNally et al., 2022 [ | Ireland | 53 UC patients (40.4 years) | 6 months | Prospective cohort study | Tofacitinib 10 mg | T: 36, P: 22 | ||
| Sandborn et al., 2012 [ | Canada | 194 UC patients (42.5 years), T: 64, P: 48 | 8 weeks | Phase II, randomized controlled trial | Tofacitinib 10mg | T: 16, P: 5 | T: 10, P: 1 | |
| Hong et al., 2020 [ | United States | 19 patients with UC (42.5 years) | 12 months | Retrospective cohort study | Tofacitinib 10mg | T: 6, P: 4 | T: 6, P: 10 | |
| Honap et al., 2022 [ | United Kingdom | 110 patients with UC (40 years) | 28 weeks | Cohort study | 6mg/kg of ustekinumab | T: 23/39, P: 32/55 | T: 17/39, P: 21/55 | |
| Van Lierop et al., 2025 [ | Canada | 121 UC patients | 141 weeks | Multicenter retrospective cohort study | 6mg/kg of ustekinumab | T: 43/81, P: 22/40 | ||
| Hong et al., 2021 [ | USA | 66 UC Patients (39.5 years) | 12 months | Real-world study | 90 mg subcutaneous (SC) injection of ustekinumab | T: 11/20, P: 23/47 | T: 9/20, P: 20/47 | |
| Chiappetta et al., 2021 [ | Italy | 68 patients with UC (42 years) | 52 weeks | Real-world study | 6mg/kg of ustekinumab | Pre: 57, Post: 55 | pre: 20, Post: 35 | |
| Tursi et al., 2024 [ | Italy | 256 patients with UC (52 years) | 24 weeks | Retrospective, observational cohort study | 6mg/kg of ustekinumab | T: 94/152, P: 42/152 | T: 125/235, P: 44/235 | |
| Danese et al., 2019 [ | Italy | 642 patients with UC | 16 weeks | Phase 3 randomized clinical trial | 90 mg of ustekinumab | Pre: 169, post: 65 | Pre: 40, post: 4 | |
| Parra et al., 2024 [ | Brazil | 56 UC patients (42.8 years) | 52 weeks | Multicenter retrospective observational cohort study | 90 mg of ustekinumab | Pre: 28/50, post: 34/50 | Pre; 9/50, post: 25/47 | |
| Amiot et al., 2020 [ | France | 103 UC patients | 16 weeks | GETAID multicenter real-world cohort study | 90 mg of ustekinumab | Pre: 36, post: 40 | ||
| Yarur et al., 2025 [ | USA | 245 UC patients | 33 weeks | Multicenter real-world cohort study | 90 mg of ustekinumab | T: 50, P: 29 | T: 7/39, P: 15/63 | |
| Narula et al., 2018 [ | Canada | 321 UC patients | 12 months | Retrospective cohort study | 300 mg of vedolizumab | T: 70, P: 56 | T: 64/321, P: 35/203 | |
| Sandborn et al., 2020 [ | United States | 216 UC patients (41.6 years), T: 106, P: 56 | 52 weeks | Phase 3, randomized controlled trial | 300 mg of intravenous vedolizumab | T: 56, P: 21 | T: 64, P: 28 | T: 49, P: 8 |
| Motoya et al., 2019 [ | Japan | 292 UC patients (44.6 years), T: 164 P: 82 | 10 weeks | Phase 3, randomized controlled trial | 300 mg of intravenous vedolizumab | T: 60, P: 25 | T: 65/164, P: 27/82 | T: 30, P: 10 |
| Loftus et al., 2016 [ | USA | 532 UC patients (41.7 years) | 52 weeks | Prospective cohort study | 300 mg of intravenous vedolizumab | T: 218, P: 148 | T: 120/136, P: 70/73 | |
| Attauabi et al., 2021 [ | Denmark | 97 UC patients | 52 weeks | Retrospective two-center cohort study | 300 mg of intravenous vedolizumab | T: 35, P: 27 | ||
| Feagan et al., 2017 [ | Canada | UC patients (40.5 years) T: 464 P: 367 | 52 weeks | Prospective cohort study | 300 mg of intravenous vedolizumab | T: 124, P: 22 | T: 125, P: 27 | T: 98, P: 17 |
| Bosca-Watts et al., 2016 [ | Spain | 33 UC patients (40.4 years) | 52 weeks | Prospective cohort study | 50 mg of golimumab | T: 14, P: 6 | T: 18 P:8 | |
| Eriksson et al., 2021 [ | Sweden | 50 UC patients (41 years) | 52 weeks | Prospective cohort study | 50 mg of golimumab | T: 14, P: 13 | T: 8, P: 10 | |
| Bossa et al., 2020 [ | Italy | 196 UC patients | 3 months | Prospective cohort study | 50 mg of golimumab | T: 130, P: 53 | ||
| Tursi et al., 2017 [ | Italy | 93 UC patients (47.5 years) | 6 months | Prospective cohort study | 50-200 mg of golimumab | T: 72, P: 30 | T: 16, P: 18 | |
| O’Connell et al., 2018 [ | Ireland | 72 UC patients (41.4 years) | 6 months | Cohort study | 50-200 mg of golimumab | T: 40, P: 32 | T: 28, P: 18 | |
| Perrig et al., 2022 [ | Switzerland | 103 UC patients | 1 year | Cohort study | 50-200 mg of golimumab | T: 63, P: 51 | T: 8, P: 52 | |
| Bressler et al., 2018 [ | Canada | 137 UC patients (44.4 years) | 1 year | Cohort study | 50-200 mg of golimumab | T: 105, P: 25 | ||
| Fumery et al., 2023 [ | France | 47 UC patients (39 years) | 24 weeks | Prospective cohort study | 50-200 mg of golimumab | T: 19, P: 15 | T: 5, P: 10 | |
| Ogata et al., 2021 [ | Japan | 1,593 UC patients (41.8 years) | 52 weeks | Prospective, multicenter, single-cohort, | Adalimumab | T: 1083, P: 971 | T: 845, P: 165 | |
| García-Bosch et al., 2013 [ | Spain | 48 UC patients | 54 weeks | Retrospective cohort study | Adalimumab | T: 40 P: 16 | ||
| Angelison et al., 2020 [ | Sweden | 118 UC patients (34.4 years) | 1.27 years | Retrospective cohort study | Adalimumab | T: 91, P: 12 | T: 38, P: 29 | |
| Suzuki et al., 2013 [ | Japan | 273 UC patients (42.5 years), T: 90, P: 96 | 52 weeks | Phase 2/3, randomized, double-blind study | Adalimumab | T: 40, P: 28 | T: 45, P: 33 | T: 10, P: 9 |
| Armuzzi et al., 2013 [ | Italy | 88 UC patients (42.8 years) | 54 weeks | Observational study | Adalimumab | T: 38, P: 15 | ||
| Sandborn et al., 2012 [ | United States | 494 UC patients | 52 weeks | Randomized, double-blind, placebo-controlled trial | 40-160 mg adalimumab | T: 45/264, P: 20/230 | ||
| Mohamed et al., 2017 [ | Kuwait | 48 adult patients with refractory UC (32.6 years) | 12 weeks | Prospective cohort study | 5 mg/kg of infliximab | T: 29, P: 15 | ||
| Tursi et al., 2017 [ | Italy | 29 UC patients (45 years) | 24 weeks | Prospective cohort study | 5 mg/kg of infliximab | T: 26, P: 29 | T: 26, P: 14 | T: 22, P: 29 |
| Selection | Comparability | Outcome | ||||||||
| Study | Representative of the exposed cohort | Selection of external control | Ascertainment of exposure | Outcome of interest not present | Main factor | Additional factor | Assessment of outcome | Sufficient follow-up time | Adequacy of follow-up time | Total |
| Honap et al., 2020 [ | * | 0 | * | 0 | * | 0 | * | * | * | 6/9 |
| Ollech et al., 2024 [ | * | * | * | 0 | * | 0 | * | 0 | 0 | 5/9 |
| Hernández Martínez et al., 2022 [ | * | * | 0 | * | * | * | * | 0 | * | 7/9 |
| Ma et al., 2023 [ | * | * | 0 | * | * | 0 | * | 0 | 0 | 5/9 |
| Jameshorani et al., 2021 [ | * | 0 | * | 0 | * | * | * | * | * | 7/9 |
| McNally et al., 2022 [ | * | * | * | 0 | * | 0 | * | 0 | 0 | 5/9 |
| Hong et al., 2020 [ | * | * | 0 | * | * | * | * | 8 | * | 8/9 |
| Honap et al., 2022 [ | * | * | * | 0 | * | 0 | * | 0 | 0 | 5/9 |
| Van Lierop et al., 2025 [ | * | * | 0 | * | * | * | * | 0 | * | 7/9 |
| Hong et al., 2021 [ | * | * | 0 | * | * | 0 | * | 0 | 0 | 5/9 |
| Chiappetta et al., 2021 [ | * | 0 | * | 0 | * | * | * | * | * | 7/9 |
| Tursi et al., 2024 [ | * | 0 | * | 0 | * | * | * | * | * | 7/9 |
| Parra et al., 2024 [ | * | 0 | * | 0 | * | 0 | * | * | * | 6/9 |
| Amiot et al., 2020 [ | * | 0 | * | 0 | * | 0 | * | * | * | 6/9 |
| Yarur et al., 2025 [ | * | * | * | 0 | * | 0 | * | 0 | 0 | 5/9 |
| Narula et al., 2018 [ | * | * | 0 | * | * | * | * | 0 | * | 7/9 |
| Loftus et al., 2016 [ | * | * | 0 | * | * | 0 | * | 0 | 0 | 5/9 |
| Attauabi et al., 2021 [ | * | 0 | * | 0 | * | * | * | * | * | 7/9 |
| Feagan et al., 2017 [ | * | * | * | 0 | * | 0 | * | 0 | 0 | 5/9 |
| Bosca-Watts et al., 2016 [ | * | * | 0 | * | * | * | * | 8 | * | 8/9 |
| Eriksson et al., 2021 [ | * | * | * | 0 | * | 0 | * | 0 | 0 | 5/9 |
| Bossa et al., 2020 [ | * | * | 0 | * | * | * | * | 0 | * | 7/9 |
| Tursi et al., 2017 [ | * | * | 0 | * | * | 0 | * | 0 | 0 | 5/9 |
| O’Connell et al., 2018 [ | * | 0 | * | 0 | * | * | * | * | * | 7/9 |
| Perrig et al., 2022 [ | * | 0 | * | 0 | * | * | * | * | * | 7/9 |
| Bressler et al., 2018 [ | * | 0 | * | 0 | * | 0 | * | * | * | 6/9 |
| Fumery et al., 2023 [ | * | 0 | * | 0 | * | 0 | * | * | * | 6/9 |
| Ogata et al., 2021 [ | * | * | * | 0 | * | 0 | * | 0 | 0 | 5/9 |
| García-Bosch et al., 2013 [ | * | * | 0 | * | * | * | * | 0 | * | 7/9 |
| Angelison et al., 2020 [ | * | * | 0 | * | * | 0 | * | 0 | 0 | 5/9 |
| Mohamed et al., 2017 [ | * | * | 0 | * | * | * | * | 0 | * | 7/9 |
| Tursi et al., 2017 [ | * | * | 0 | * | * | 0 | * | 0 | 0 | 5/9 |
| Armuzzi et al., 2013 [ | * | * | 0 | * | * | * | * | 0 | * | 7/9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Bowel Disease · Microscopic Colitis · Gastrointestinal motility and disorders
Introduction and background
Ulcerative colitis (UC) is a chronic inflammatory bowel disease (IBD), characterized by persistent colonic mucosal inflammation, which often starts in the rectum and spreads to all parts of the colon [1]. With incidence rates ranging from nine to 20 cases per 100,000 person-years, UC has historically been more common in Western countries, e.g., North America and Northern and Western Europe [2]. However, newly industrialized regions such as Asia, the Middle East [3], and South America [4] have seen a significant rise in newly diagnosed cases in recent decades. Urbanization, nutritional changes, environmental changes, and better disease detection are all major causes for this rapid increase in the incidence of UC [5].
Its origin is complex and includes changes in gut microbiota, immunological dysregulation, genetic predisposition, and environmental factors [6, 7]. Rectal bleeding, diarrhea, abdominal pain, and urgency are prominent symptoms of UC that seriously lower quality of life. Moderate-to-severe instances are characterized by persistent disease activity that is often resistant to standard treatments such as immunomodulators, corticosteroids, and aminosalicylates [8].
Over the past 20 years, the treatment of moderate-to-severe UC has changed due to the introduction of biological treatments [9]. Complex, protein-based medications known as biologics are made from living cells and are intended to target particular immune system elements that contribute to inflammation [9, 10]. Based on encouraging outcomes from clinical studies, they include integrin receptor antagonists (vedolizumab) [11], interleukin inhibitors (ustekinumab) [12], and tumor necrosis factor-alpha (TNF-α) inhibitors (infliximab, adalimumab, and golimumab) [13] that have been approved for the treatment of UC. These medications seek to lessen corticosteroid reliance, encourage mucosal repair, and result in sustained clinical remission [14, 15].
Outcomes of biological treatments can differ depending on patient heterogeneity, illness severity, immunogenicity, and loss of response over time, even with the growing availability of biologics [10, 16]. There is still ongoing research into the relative safety and efficacy of various drugs, particularly in light of new randomized clinical trials (RCTs) and empirical data. Furthermore, real-world research is crucial for comprehending how these therapies function in varied populations with comorbidities, concurrent medications, and varying adherence levels, even while clinical trials offer efficacy data under ideal circumstances.
Various publications have reported the effectiveness of vedolizumab, tofacitinib, infliximab, and golimumab individually [17-20]. No study has reported the outcomes of all biological drugs comprehensively to suggest a drug with more effective outcomes. Furthermore, clinical professionals find it difficult to choose the best biologic for each patient due to the therapeutic arsenal’s quick increase. Clinical guidelines and evidence-based decision-making require a thorough synthesis of the available data. An updated meta-analysis that systematically analyzes the efficacy of numerous biologics in moderate-to-severe UC is necessary, especially in light of recently published studies and long-term outcome data, even though prior evaluations have focused on individual biologic agents or certain outcomes.
The purpose of this systematic review and meta-analysis is to assess how well biologic treatments work for treating moderate-to-severe UC. This review aims to provide a consolidated evidence base to guide therapeutic strategies for patients who are not responding to conventional therapy or who need maintenance of long-term disease control by combining data from high-quality observational studies and RCTs.
Review
Methods
Search Design
This systematic review and meta-analysis were performed by following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [21] to fulfill research aims. There was no need for an additional ethical review due to the involvement of previously published retrospective and prospective cohort studies.
Population Intervention Control Outcome (PICO) Framework
This study used the PICO framework to guide the search: P: Patients with moderate-to-severe UC; I: Biologic therapies (e.g., anti-TNF agents, anti-integrins, anti-IL agents, JAK inhibitors); C: placebo or conventional therapies (e.g., corticosteroids, immunomodulators) or head-to-head comparisons between different biologics; O: clinical remission, clinical response, mucosal healing, and adverse events.
Search Strategy
The PRISMA guidelines assisted in the selection of research articles related to the study aims. Three electronic databases, PubMed, Excerpta Medica database (EMBASE), and the Cochrane Library, were searched from inception to February 2025. The Medical Subject Headings (MeSH) keywords used for the search of research articles from PubMed were ("Ulcerative Colitis"[MeSH] OR "Inflammatory Bowel Diseases"[MeSH]) AND ("Biological Products"[MeSH] OR "biologic therapy" OR "Anti-TNF agents" OR "JAK inhibitors") AND ("Treatment Outcome"[MeSH] OR "Effectiveness" OR "Clinical Remission") AND ("Moderate-to-Severe" OR "moderate" OR "severe"). A similar search strategy was used for other databases. The databases were searched from January 2011 to April 2025. The search was restricted to the English language. We carefully examined the reference lists of all previous systematic reviews and meta-analysis-based articles to search for further research articles.
Eligibility Criteria
The eligibility criteria were used to select and screen research articles after searching for research articles from electronic databases.
Inclusion Criteria
Studies were included if they analyzed adult patients over 18 years of age diagnosed with moderate to severe UC and evaluated the effects of biological therapies compared to placebo. Eligible studies reported outcomes such as response rates, remission rates, and mucosal healing. Only primary research studies, including RCTs and prospective cohort studies, were considered. Additionally, studies were required to have full-text availability and be published in the English language.
Exclusion Criteria
Studies were excluded if they involved patient populations with other types of cancer or focused on individuals receiving therapies other than biological treatments. Research investigating the long-term outcomes or maintenance effects of biological drugs for UC was also excluded. Non-primary studies, such as systematic reviews, meta-analyses, comprehensive reviews, narrative reviews, case-control studies, and editorials, were not included. Finally, studies published in languages other than English or lacking full-text access were excluded.
Data Extraction
Two independent reviewers extracted the data to be placed in a pre-specified table. The studies obtained by the database search were entered into the EndNote library (Clarivate, London, UK). Duplicates were excluded in the next step. The eligibility criteria were applied by reviewers in a blinded manner to all individual studies. Discrepancies were sorted by mutual agreement. Data related to demographic information, such as authors, year, country, study population, study design, study follow-up, and primary outcomes, were extracted. Discrepancies were resolved by consulting with a third reviewer.
Risk of Bias Assessment
The Cochrane Risk of Bias tool was applied to assess the risk of bias of included RCTs. The risk bias of included studies was evaluated on the basis of six domains: allocation concealment, blinding of participants, selection bias, blinding of outcome assessment, selective reporting, and other bias. The score or level of each included study was categorized into low risk, unclear, and high risk [22].
Quality Assessment of Cohort Studies
The quality of the included studies was assessed by using proper tools on the basis of study design. Due to the inclusion of observational studies, the Newcastle-Ottawa Scale (NOS) was used for quality assessment [23]. The score of >7 for included studies was considered low risk, scores of five to seven for included studies indicated moderate risk, and <5 for included studies showed high risk. Any disagreement in risk bias assessment was resolved through consensus.
Statistical Analysis
Review Manager Software (The Cochrane Collaboration, 2020, Review Manager (RevMan) (computer software) (version 5.4) was used to conduct statistical analyses. The studies in the analysis are assumed to be a random sample from a universe of potential studies, and this analysis was used to make an inference about that universe. Pooled analysis of data was performed for studies with potential heterogeneity using random effects models. Statistical significance was set at P < 0.05 and was considered statistically significant [24]. Heterogeneity was evaluated using the I² statistic, with I² values > 50% indicating significant heterogeneity.
Results
Search Results
The selection and screening of research articles related to the study aim, “Effectiveness of various biological therapies for treatment of UC,” was performed by following the PRISMA guidelines in this meta-analysis. A total of 39,000 research articles were extracted after applying the above-mentioned search strategy. Only 11,000 papers were initially screened, and 7,011 research articles were retrieved before final screening. Among those, only 3,001 articles were assessed for eligibility criteria, and the final number of research articles after applying exclusion criteria was 43, as mentioned in Figure 1.
PRISMA flowchart outlining the screening and selection of included studiesPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Table 1 presents the characteristics of the included studies.
Quality Assessment of the Included Studies
Among 33 observational cohort studies, 19 included studies were low risk, and 14 studies were moderate risk, as represented in Table 2. Most comparisons showed low to moderate evidence quality, and the study's limitations, inconsistencies, indirectness, and imprecision were the key reasons for the confidence decline.
Risk of Bias Assessment
The Cochrane tool was used for risk bias assessment of the 10 included RCTs. All 10 included studies were low risk, as mentioned in Figure 2 and Figure 3.
Representation of the risk bias of the included studies
Representations of the risk bias summary of the included studiesStudies included: [25, 27, 28, 31, 35, 42, 47, 48, 63, 65]
Primary Outcomes
Response rates: Among 43 included studies, 33 research studies have reported the response rates as outcomes in UC patients receiving treatment with biological drugs as compared to placebo. The pooled analysis showed that clinical response rates improved among UC patients after receiving biological drugs as compared to placebo (odds ratio (OR): 2.19 (CI 95%: 2.66-3.19), p<0.00001, I2= 83%), as shown in Figure 4.
Forest plot of the odds ratio of response rates among UC patients receiving biological drugs as compared to placeboCI: confidence interval; UC: ulcerative colitis1.1.1: [25, 27-28, 30-36, 40]; 1.1.2: [37, 36, 41-43, 45]; 1.1.3: [46, 47, 48, 49, 51]; 1.1.4: [52-54, 57, 58, 66, 68, 69]; 1.1.5: [62, 63]; 1.1.6: [55]
The subgroup analysis of different biological drugs showed that tofacitinib is more effective in improving response rates (OR: 3.73 (95% CI; 3.16-4.40), p<0.0001) and vedolizumab is least effective in terms of improving response rates (OR: 1.95 (1.64-2.33), p<0.00001). The symmetrical distribution of studies on the funnel plot showed the low publication bias as reported by meta-regression results of response rates among the included studies (Figure 5).
Funnel plot of the odds ratio (OR) of response rates among UC patients receiving biological drugs as compared to placeboUC: ulcerative colitisStudies included: [25, 27, 28, 31, 35, 42, 47, 48, 63, 65]
Remission rates: Among 43 included studies, 37 research studies have reported the clinical remission rates as outcomes in UC patients receiving treatment with biological drugs as compared to placebo. The pooled analysis showed that clinical response rates improved among UC patients after receiving biological drugs as compared to placebo (OR: 3.10 (CI 95%: 2.82-3.42), p<0.00001, I2= 92%), as shown in Figure 6.
Forest plot of the odds ratio of remission rates among UC patients receiving biological drugs as compared to placeboCI: confidence interval; UC: ulcerative colitis1.2.1: [27-32, 35-36]; 1.2.2: [37-39, 40-45]; 1.2.3: [46-51]; 1.2.4 [41, 52-53, 56-57, 59]; 1.2.5: [60, 62-65]; 1.2.6: [55]
The subgroup analysis of different biological drugs showed that adalimumab is more effective in improving remission rates (OR: 6.60 (95% CI; 5.63-7.74), p<0.0001) and golimumab is least effective in terms of improving remission rates (OR: 0.65 (0.47-0.90), p<0.00001). The symmetrical distribution of studies on the funnel plot showed the low publication bias as reported by meta-regression results of response rates among included studies, as shown in Figure 7.
Funnel plot of the odds ratio (OR) of remission rates among UC patients receiving biological drugs as compared to placeboUC: ulcerative colitisStudies includes: [25, 27, 28, 31, 35, 42, 47, 48, 63, 65]
Among 43 included studies, only nine research studies have reported the clinical mucosal healing as an outcome in UC patients receiving treatment with biological drugs as compared to placebo. The pooled analysis showed that mucosal healing significantly improved among UC patients after receiving biological drugs as compared to placebo (OR: 1.66 (CI 95%: 1.47-1.88), p<0.00001, I2= 85%) as shown in Figure 8.
Forest plot of the odds ratio of mucosal healing among UC patients receiving biological drugs as compared to placebo CI: confidence interval; UC: ulcerative colitisStudies included: [29, 47, 48, 51, 55, 60, 61, 63, 66]
The symmetrical distribution of studies on the funnel plot showed the low publication bias as reported by the meta-regression results of response rates among included studies, as shown in Figure 9.
Funnel plot of the odds ratio (OR) of mucosal healing among UC patients receiving biological drugs as compared to placebo UC: ulcerative colitisStudies included: [25, 27, 28, 31, 35, 42, 47, 48, 63, 65]
Discussion
This systematic review and meta-analysis evaluated the efficacy of six biological drugs in treating UC across 43 included studies. The results demonstrated that biological drugs collectively outperform placebo across all key clinical outcomes. Patients receiving biological therapies showed significantly higher response rates (OR: 2.19, 95% CI: 2.66-3.19*), remission rates (OR: 3.10, 95% CI: 2.82-3.42), and mucosal healing rates (OR: 1.66, 95% CI: 1.47-1.88), with all outcomes achieving high statistical significance (p < 0.00001). Despite substantial heterogeneity across studies (I² = 83-92%), consistent benefits were observed. All RCTs included were assessed as low-risk using the Cochrane bias assessment tool, strengthening the reliability of these findings. While 33 cohort studies were assessed by NOS, 19 studies were predicted to be low risk, and 14 studies were predicted to be moderate risk. The symmetrical distribution of studies on the funnel plot showed low to moderate publication bias among included studies.
The findings of this study were consistent with previous studies that reported the effectiveness and safety of biologics and small-molecule drugs for the treatment of UC patients [68-70]. These studies proved that biological agents are effective treatments for UC patients with fewer adverse events as compared to other therapeutic strategies.
This meta-analysis has several strengths. It assessed 43 studies from six varied biological therapies in a complete manner, thus giving a general overview of their efficacy for UC treatment. The use of systematic review and meta-analysis methodology increases the validity of the findings by aggregating data from RCTs and observational cohort studies. The use of strict quality assessment measures, Cochrane for RCTs and NOS for cohort studies, prevented methodological bias, as the majority of studies were classed as low risk. The statistically significant pooled odds ratios for clinical response, remission, and mucosal healing, each with p-values < 0.00001, strongly indicate that biological therapies work in moderate-to-severe UC. In addition, the symmetrical shape of the funnel plot indicates low publication bias, validating the findings.
Nonetheless, a number of limitations need to be recognized. The high heterogeneity between studies (I² of 83% to 92%) can affect the consistency of the pooled estimates and reflects variation in study populations, interventions, and outcome measures. While the majority of studies were at low to moderate risk, the inclusion of observational cohort studies may introduce potential confounding and selection bias. Study design differences, differing follow-up lengths, and differing drug dosing regimens might also have contributed to differences in the findings. Publication bias seemed low but cannot be entirely eliminated, particularly since biologic drug trials are of high-profile status and possibly receive industry sponsorship.
Clinically, the findings highlight the key position biologics play in the therapeutic management of moderate-to-severe UC. Clinicians can consider using biologics not only for clinical response induction but also for remission and mucosal healing, which are key to the patient's improved quality of life and long-term outcomes. The findings are consistent with existing guidelines and are likely to contribute to therapeutic decision-making, especially among patients with refractoriness to conventional therapies.
Conclusions
Overall, this study offers robust evidence that biological treatments substantially enhance treatment outcomes in patients with moderate-to-severe UC over placebo. Although there is some heterogeneity and limitations in combining studies of different types, the overall quality of evidence is low to moderate. These findings support the clinical utility of biologics and underscore the importance of ongoing comparative studies and long-term outcome data to further refine treatment strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ulcerative colitis in adults: a review JAMA Gros B Kaplan GG 95196533020233769855910.1001/jama.2023.15389 · doi ↗ · pubmed ↗
- 2Epidemiology and pathogenesis of ulcerative colitis Gastroenterol Clin North Am Du L Ha C 6436544920203312168610.1016/j.gtc.2020.07.005 · doi ↗ · pubmed ↗
- 3Epidemiology, burden of disease, and unmet needs in the treatment of ulcerative colitis in Asia Expert Rev Gastroenterol Hepatol Wei SC Sollano J Hui YT Yu W Santos Estrella PV Llamado LJ Koram N 2752891520213310734410.1080/17474124.2021.1840976 · doi ↗ · pubmed ↗
- 4Review of the epidemiology and burden of ulcerative colitis in Latin America Therap Adv Gastroenterol Kotze PG Steinwurz F Francisconi C Zaltman C Pinheiro M Salese L Ponce de Leon D 175628482093173913202010.1177/1756284820931739 PMC 735003932695230 · doi ↗ · pubmed ↗
- 5Risk factors for complications in patients with ulcerative colitis United European Gastroenterol J Manser CN Borovicka J Seibold F Vavricka SR Lakatos PL Fried M Rogler G 2812874201610.1177/2050640615627533 PMC 480437927087958 · doi ↗ · pubmed ↗
- 6Risk factors and characteristics of extent progression in ulcerative colitis Inflamm Bowel Dis Etchevers MJ Aceituno M García-Bosch O Ordás I Sans M Ricart E Panés J 132013251520091923590910.1002/ibd.20897 · doi ↗ · pubmed ↗
- 7Risk factors for extensive ulcerative colitis and ulcerative proctitis: a population based case-control study Gut Samuelsson SM Ekbom A Zack M Helmick CG Adami HO 15261530321991177396010.1136/gut.32.12.1526 PMC 1379255 · doi ↗ · pubmed ↗
- 8Clinical presentation of Crohn's, ulcerative colitis, and indeterminate colitis: symptoms, extraintestinal manifestations, and disease phenotypes Semin Pediatr Surg Yu YR Rodriguez JR 3493552620172912650210.1053/j.sempedsurg.2017.10.003 · doi ↗ · pubmed ↗