Impact of Sleeping Habits on the Weight Loss Effect of Oral Glucagon-Like Peptide-1 Receptor Agonists Among Obese Patients: An Observational Study in Japan
Kazuki Takakura, Nagisa Koda, Yuji Kinoshita, Maki Oh, Muneyuki Koyama, Machi Suka

TL;DR
This study found that better sleep habits may enhance weight loss effects of a drug called semaglutide in obese patients in Japan.
Contribution
The study is the first to explore how sleeping habits influence the effectiveness of oral GLP-1 receptor agonists in a real-world clinical setting.
Findings
Participants with improved sleep time or quality showed better weight loss outcomes.
Sufficient sleep was associated with enhanced therapeutic efficacy of semaglutide.
The study highlights the importance of sleep in optimizing obesity treatment with GLP-1 RAs.
Abstract
Although glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have been used as anti-obesity agents, there are individual differences between these agents, thus making it difficult to achieve optimal treatment efficacy. This study aimed to determine the impact of sleeping habits on the weight loss effect of semaglutide, an oral GLP-1 RA, among Japanese individuals with obesity. Data were collected from March 2022 to October 2024. A total of 367 Japanese adults (30.5% men and 69.5% women) were included for analysis. Among them, 83.9% had a body mass index (BMI) between 25 and 35 kg/m2, and 16.1% had a BMI of 35 kg/m2 or more. The percentage change from baseline in body weight was assessed every three months and at the end of the follow-up period. The assessments were conducted in accordance with the Japanese guidelines for the management of obesity. Logistic regression was used to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
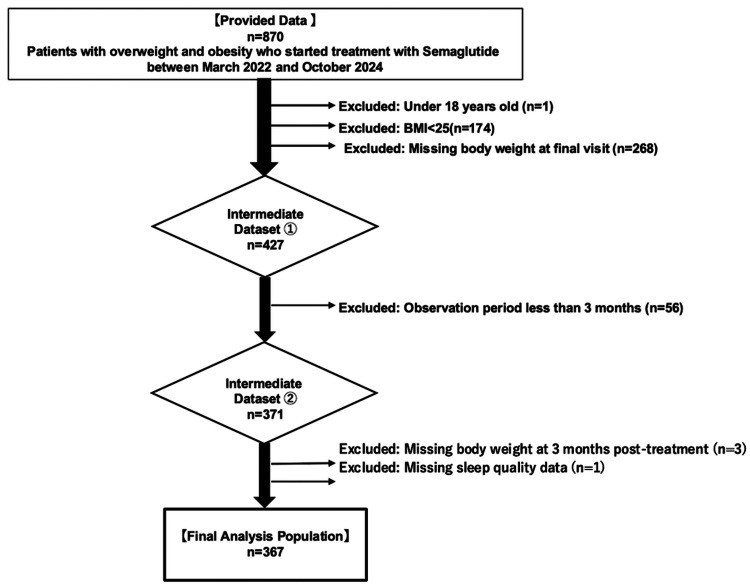 Figure 1
Figure 1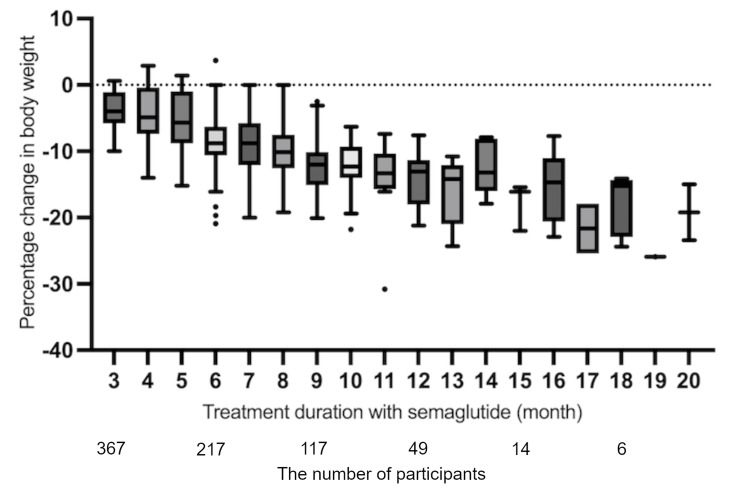 Figure 2
Figure 2| Parameters | Number | % | |
| Sex | Male | 112 | 30.5% |
| Female | 255 | 69.5% | |
| Age | 18-29 years | 31 | 8.4% |
| 30-59 years | 298 | 81.2% | |
| 60+ years | 38 | 10.4% | |
| Body mass index | 25-34 kg/m2 | 308 | 83.9% |
| 35+ kg/m2 | 59 | 16.1% | |
| Alcohol habits | Yes | 91 | 24.8% |
| Smoking habits | Yes | 55 | 15.0% |
| Exercise habits | Yes | 143 | 39.0% |
| Breakfast | No | 46 | 12.5% |
| Dinner time | After 9 PM | 58 | 15.8% |
| Interval between dinner and bedtime (hours) | Less than 3 | 25 | 6.8% |
| Stress levels | 0 | 140 | 38.1% |
| 1 | 116 | 31.6% | |
| 2 | 111 | 30.2% | |
| Medical history | Metabolic diseases | 158 | 43.1% |
| Cancers | 11 | 3.0% | |
| Mental disorders | 45 | 12.3% | |
| Sleep apnea | 21 | 5.7% | |
| Sleeping hours before treatment | Less than 6 | 115 | 31.3% |
| Sleep quality before treatment | Poor | 160 | 43.6% |
| Sleeping pills | Lemborexant | 51 | 13.9% |
| Others | 36 | 9.8% | |
| Adverse events | Yes | 26 | 7.1% |
| Time point | Median (range), % |
| After 3 months of treatment | 4.6 (-2.9 to 14.8) |
| After 6 months of treatment | 8.6 (-3.7 to 22.2) |
| Time point | Total | Achiever | Rate |
| At 3 months of treatment | 367 | 284 | 77.4% |
| At 6 months of treatment | 217 | 187 | 86.2% |
| At the last observation | 176 | 151 | 85.8% |
| Parameters | Total | Achiever | Rate | Chi-square | p | ||
| Sex | Male | 112 | 80 | 71.4% | 3.267 | 0.071 | |
| Female | 255 | 204 | 80.0% | ||||
| Age | 18-29 years | 31 | 28 | 90.3% | 3.425 | 0.180 | |
| 30-59 years | 298 | 226 | 75.8% | ||||
| 60+ years | 38 | 30 | 78.9% | ||||
| Body mass index | 25-34 kg/m2 | 308 | 237 | 76.9% | 0.208 | 0.648 | |
| 35+ kg/m2 | 59 | 47 | 79.7% | ||||
| Alcohol habits | No | 276 | 214 | 77.5% | 0.015 | 0.904 | |
| Yes | 91 | 70 | 76.9% | ||||
| Smoking habits | No | 312 | 240 | 76.9% | 0.253 | 0.615 | |
| Yes | 55 | 44 | 80.0% | ||||
| Exercise habits | No | 224 | 164 | 73.2% | 5.712 | 0.017 | |
| Yes | 143 | 120 | 83.9% | ||||
| Breakfast | No | 321 | 253 | 78.8% | 3.001 | 0.083 | |
| Yes | 46 | 31 | 67.4% | ||||
| Dinner time | Before 9 PM | 309 | 255 | 82.5% | 29.517 | <0.001 | |
| After 9 PM | 58 | 29 | 50.0% | ||||
| Interval between dinner and bedtime (hours) | More than 3 | 342 | 274 | 80.1% | 21.424 | <0.001 | |
| Less than 3 | 25 | 10 | 40.0% | ||||
| Stress levels | 0 | 140 | 125 | 89.3% | 27.893 | <0.001 | |
| 1 | 116 | 91 | 78.4% | ||||
| 2 | 111 | 68 | 61.3% | ||||
| Medical history | Metabolic diseases | No | 209 | 162 | 77.5% | 0.005 | 0.946 |
| Yes | 158 | 122 | 77.2% | ||||
| Cancers | No | 356 | 275 | 77.2% | - | 1.000 | |
| Yes | 11 | 9 | 81.8% | ||||
| Mental disorders | No | 322 | 253 | 78.6% | 2.115 | 0.146 | |
| Yes | 45 | 31 | 68.9% | ||||
| Sleep apnea | No | 346 | 270 | 78.0% | - | 0.280 | |
| Yes | 21 | 14 | 66.7% | ||||
| Sleeping hours before treatment (hours) | More than 6 | 252 | 210 | 83.3% | 16.263 | <0.001 | |
| Less than 6 | 115 | 74 | 64.3% | ||||
| Sleep quality before treatment | Good | 207 | 177 | 85.5% | 17.902 | <0.001 | |
| Poor | 160 | 107 | 66.9% | ||||
| Adverse events | No | 341 | 265 | 77.7% | 0.297 | 0.586 | |
| Yes | 26 | 19 | 73.1% | ||||
| Parameters | Model 1 | Model 2 | Model 3 | ||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | ||
| Sex | Female | 0.521 | 0.282-0.961 | 0.505 | 0.261-0.978 | 0.511 | 0.274-0.955 |
| Age | 1.001 | 0.976-1.027 | 1.012 | 0.985-1.040 | 1.006 | 0.980-1.033 | |
| Body mass index | 0.987 | 0.928-1.049 | 0.981 | 0.917-1.049 | 0.978 | 0.917-1.044 | |
| Alcohol habits | Yes | 0.942 | 0.488-1.818 | 0.965 | 0.469-1.985 | 1.012 | 0.520-1.969 |
| Smoking habits | Yes | 0.846 | 0.379-1.889 | 0.626 | 0.255-1.540 | 0.779 | 0.345-1.759 |
| Exercise habits | Yes | 0.697 | 0.383-1.269 | 0.974 | 0.509-1.864 | 0.767 | 0.417-1.412 |
| Breakfast | Yes | 0.727 | 0.341-1.551 | 1.476 | 0.614-3.550 | 0.807 | 0.372-1.749 |
| Interval between dinner and bedtime (hours) | Less than 3 | 4.132 | 1.586-10.761 | 3.748 | 1.394-10.076 | 4.208 | 1.610-11.001 |
| Stress levels | 0 | 1.000 | Reference | 1.000 | Reference | 1.000 | Reference |
| 1 | 2.007 | 0.968-4.164 | 1.917 | 0.888-4.141 | 2.043 | 0.972-4.293 | |
| 2 | 3.759 | 1.822-7.753 | 2.746 | 1.248-6.045 | 3.561 | 1.701-7.454 | |
| Sleeping hours before treatment | More than 6 | 0.486 | 0.275-0.859 | - | - | 0.431 | 0.238-0.777 |
| Changes in sleeping hours | Less than 6 | - | - | 1.000 | Reference | - | - |
| To improve under treatment | - | - | 0.147 | 0.056-0.383 | - | - | |
| More than 6 | - | - | 0.231 | 0.112-0.479 | - | - | |
| Sleep quality before treatment | Good | 0.589 | 0.328-1.059 | - | - | 0.454 | 0.243-0.846 |
| Changes in sleep quality | Poor | - | - | 1.000 | Reference | - | - |
| To improve under treatment | - | - | 0.210 | 0.071-0.621 | - | - | |
| Good | - | - | 0.224 | 0.100-0.501 | - | - | |
| Sleeping pills | Lemborexant | - | - | - | - | 0.448 | 0.186-1.081 |
| Others | - | - | - | - | 2.878 | 1.251-6.618 | |
| Adverse events | Yes | 1.237 | 0.449-3.609 | 0.963 | 0.322-2.876 | 1.245 | 0.441-3.512 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiet and metabolism studies · Obesity, Physical Activity, Diet · Sleep and related disorders
Introduction
The number of individuals with overweight and obesity has been considerably increasing worldwide. Therefore, more rigorous management is needed in many countries, including Japan. Obesity is a major risk factor for the deterioration of lifestyle diseases, cardiac infarction, stroke, and cancers in various organs; therefore, the World Health Organization is now playing a central role in accelerating the prevention of obesity [1-3]. Moreover, glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have been clinically approved as antidiabetic agents and have been shown to suppress appetite, which has resulted in their use in clinical settings as anti-obesity drugs [4]. However, not everyone who is treated with GLP-1 RAs experiences weight loss, because there are individual differences in the effects of GLP-1 RAs [5-8]. Indeed, variability in treatment outcomes is an important topic for healthcare professionals who have obese patients struggling with weight loss. Hence, detailed information regarding how to obtain sufficient weight loss efficacy of GLP-1 RA is indispensable to improve the success rate in more cases.
Recently, several investigations have revealed that a lack of sleep is a significant risk factor for obesity, and the underlying mechanisms have also become clear [9-12]. In particular, an association has been observed between appetite-related hormones, which are influenced by the sleeping state, and obesity [13-17]. Therefore, herein, we investigated the impact of sleeping habits on the weight loss effect of semaglutide, a daily oral GLP-1 RA, among Japanese individuals with obesity. Moreover, we also evaluated whether improving sleeping habits, regardless of the use of sleeping pills, can yield better treatment outcomes with semaglutide.
Furthermore, treatment progress with semaglutide was tracked and evaluated over time to perform a longitudinal evaluation of treatment outcomes with semaglutide, considering that obese patients frequently experience body weight plateau or regain after successful initial weight loss, which makes sustained weight management much more challenging [18,19].
The occurrence of obesity is multifactorial and involves genetic and environmental factors, but it is ultimately due to a long-term imbalance in energy intake and energy expenditure [20,21]. Accordingly, to perform a comprehensive assessment of the factors that influence the weight loss efficacy of semaglutide in addition to sleeping habits, various other factors, such as sex, age, medical history, dietary habits, smoking and alcohol habits, exercise routine, and stress level, were assessed via secondary analysis.
Materials and methods
Study design and population
A total of 870 patients who started treatment with semaglutide at UnMed Clinic Motomachi between March 2022 and October 2024 were potentially eligible for inclusion in this observational cohort study. All demographic and clinical data were retrospectively extracted from electronic medical records on the basis of self-reported information. In a preliminary questionnaire, participants were asked about their medical history, dietary habits, drinking and smoking habits, degree of stress, and regular exercise routine with reference to the latest guidelines for the management of obesity disease from the Japan Society for the Study of Obesity (JASSO) [22]. Clinical data, such as age, sex, height, weight, and body mass index (BMI), were also collected at baseline and during follow-up. Additionally, sleeping hours and sleep quality before initiating treatment and during treatment were also verified for all the participants by self-report. Sleep quality was assessed by dividing the participants into two groups: sufficient sleep quality and poor sleep quality. The degree of stress was also collected by self-report and assessed by dividing the participants into three groups: none, moderate, and high. In accordance with the same guidelines, the percentage change from baseline in body weight was assessed after three months, six months, and the final follow-up period from treatment initiation [22].
In terms of the dosage of semaglutide, the attending physician initially started with 3 mg as the minimum dosage and gradually increased to 7 mg and 14 mg as needed, considering not only its appetite-suppressing effect but also its side effects.
Participants were provided with informed consent for study participation and relevant information, including their right to withdraw at any time. The study protocol was approved by the Ethics Committee of UnMed Clinic Motomachi, Kanagawa, Japan (authorization number: UM23-01). The review board approved and waived the need for written informed consent from the participants because of the retrospective, non-interventional nature of this study. The study followed the recommended guidelines of the Declaration of Helsinki [23]. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline [24].
For the evaluation of therapeutic efficacy, 503 censored patients were excluded because of being under the age of 18, lack of necessary information, a BMI less than 25, or a tracking period of less than three months. In addition, participants who did not provide consent to participate in the study were excluded. Ultimately, a total of 367 patients with obesity who received semaglutide for more than three months were included in the analyses, as shown in Figure 1. A summary of the data collected from the study participants is presented in Table 1.
Flowchart of the study participantsThe reasons for screening failure and discontinuation from the study are indicated.BMI: body mass index
Weight loss criteria for Japanese individuals with obesity
Obesity is defined on the basis of BMI, which is calculated as the mass in kilograms divided by the square of the height in meters (kg/m^2^). According to the guidelines for the management of obesity from JASSO, obesity is defined as excessive fat storage in adipose tissue associated with a BMI of 25 kg/m^2^ or greater in Japan [22,25], and a BMI of 35 kg/m^2^ or greater is regarded as high-degree obesity. The BMI threshold of Japanese individuals is lower than that of individuals in Western countries (30 kg/m^2^ or greater), as Japanese individuals are susceptible to obesity-related diseases at lower BMIs [26-28]. Consequently, a BMI of 25 kg/m^2^ or greater is considered an appropriate threshold for Japanese individuals with obesity, although patients with a BMI between 25 and 30 kg/m^2^ are considered overweight according to Western standards.
Additionally, the initial weight loss goals are defined in the same guidelines as a decrease of 3% or more in initial weight in the first three months [22]. Thus, the evaluation of weight decrease in this study was performed according to the guidelines in a way that is appropriate for Japanese obese individuals.
Outcome measures
The percentage change from baseline in body weight was assessed once every three months and at the end of the follow-up period from treatment initiation. Additionally, all of the participants whose treatment progressed with semaglutide for up to 20 months were tracked and evaluated over time. We also investigated the associations between several clinical factors, including sleeping habits, and the weight loss efficacy of semaglutide in Japanese patients with obesity.
Sleeping habits during the treatment period
With respect to the sleeping hours reported by all of the study participants, we selected six hours, which is less than the hours recommended by the National Sleep Foundation Report, as the cutoff value in this analysis [29]. With respect to the sleeping situation, we confirmed whether the participants were taking sleeping pills or not, including before starting treatment.
Statistical analysis
All statistical analyses were performed via SAS V.9.4 software (SAS Institute, Cary, NC). The chi-square test was used to compare the distributions of categorical variables. Multiple logistic regression analysis was performed to identify factors associated with treatment efficacy with semaglutide. Odds ratios (ORs) and 95% confidence intervals (CIs) for treatment outcomes were calculated via multivariate adjustment. This multivariate analysis was applied to target changes in sleeping habits during the treatment period as an explanatory variable and the weight loss efficacy of semaglutide as a response variable. The influence of changes in sleeping habits, including sleeping hours and sleep quality during the treatment period, on the weight loss efficacy with semaglutide was analyzed via three adjusted models along the treatment time axis: Model 1, at the initial visit, reflecting before initiating treatment; Model 2, changes in sleeping habits during treatment period; and Model 3, therapeutic interventions for sleeping habits involving the use of sleeping pills under treatment with semaglutide. Sex, age, BMI, alcohol and smoking habits, exercise habits, habit of eating breakfast, interval between dinner and bedtime, and stress level were included as fixed factors. The threshold for statistical significance was set at p<0.05.
Results
Participant characteristics
A total of 367 Japanese participants with obesity, regardless of the presence or absence of diabetes, who received semaglutide at UnMed Clinic Motomachi between March 2022 and October 2024, were included in the analyses (Figure 1). The self-reported characteristics of the study population are summarized in Table 1. There was a greater predominance of female to male subjects, i.e., 69.5% to 30.5%, respectively. The majority of the participants (81.2%) belonged to the age group ranging from 30 to 59 years. Among them, 83.9% have obesity (25 kg/m^2^ < BMI < 35 kg/m^2^), and 16.1% have high-degree obesity (BMI ≥ 35). In terms of dietary patterns, 46 (12.5%) participants usually skip breakfast, 58 (15.8%) participants have late dinner after 9 PM, and 25 (6.8%) sleep within three hours of having dinner. According to the results of the questionnaire, the level of stress was 0 (none) in 38.1%, 1 (medium) in 31.6%, and 2 (high) in 30.2% of the study participants. Additionally, 115 (31.3%) participants slept less than six hours, and 160 (43.6%) participants experienced poor-quality sleep at the beginning of treatment. The frequency of adverse events led to the discontinuation of semaglutide in 26 (7.1%) participants, primarily gastrointestinal problems; no serious events occurred, and a total of 87 (23.7%) were taking any sleeping pills during the treatment period.
Semaglutide had both immediate and long-acting effects on weight reduction in Japanese obese individuals
At three months, the average percentage change from baseline in body weight was 4.6%, ranging from -2.9% to 14.8%. At six months, the average percentage change from baseline in body weight was 8.6%, ranging from -3.7% to 22.2% (Table 2). As shown in Table 3, 284 (77.4%) study participants achieved a weight reduction of at least 3% at three months of treatment with semaglutide. Additionally, 187 (86.2%) participants at six months successfully achieved sustained weight loss with semaglutide. All of the achievers at six months were able to maintain weight loss throughout the entire treatment period. Clinically meaningful weight reduction at an early stage (by three months) and subsequent weight management were achieved by long-term administration of semaglutide in approximately 80% of the study participants. Conversely, nonachievers who could not lose weight at an early stage ended up failing by the end of the observation period. Overall, sustained weight reduction with semaglutide was observed over the follow-up period of up to 20 months in this study (Figure 2). In short, a good start with semaglutide is an important step in long-term, successful weight management.
Time series graph showing the chronological evaluation of weight reduction with semaglutide
Severe stress and late dinner have a negative influence on the weight loss effect of semaglutide
In the evaluation of factors related to a lack of success in weight loss after three months of treatment with semaglutide, a high level of stress significantly interfered with the success rate of weight reduction for patients with obesity after three months of treatment with semaglutide (p<0.001). Moreover, late dinner after 9 PM and less than three hours from dinner to bed also resulted in a reduced therapeutic response to semaglutide (p<0.001) (Table 4). Conversely, differences in sex, age, drinking and smoking habits, habit of eating breakfast, and medical history had no significant influence on the weight loss effect of semaglutide, suggesting that there is no difference in the outcomes between diabetic and non-diabetic participants. Interestingly, the degree of obesity was also not correlated with the weight loss success rate after three months of treatment with semaglutide, whereas exercise habits on a daily basis were significantly related in the study population, as expected (p=0.017) (Table 4).
The weight loss effect of semaglutide is greater in female patients than in male patients, but there are no age differences
Similarly, female patients with obesity are more likely to experience weight loss with semaglutide, as shown in Table 5 (OR: 0.52, 95% CI: 0.28-0.96). In contrast, age was not a factor related to weight loss failure after three months of treatment with semaglutide (OR: 1.00, 95% CI: 0.98-1.03). These data are promising for obese women who are considering weight loss treatment and suggest that it is never too late to start weight loss treatment, even for patients aged 60 and above.
Sleep extension enhances the weight loss effect of semaglutide in obese patients
Finally, we investigated the impact of getting enough sleep with or without the use of sleeping pills under treatment with semaglutide. The evaluation was conducted with consideration of the changes in sleeping habits during the treatment period, as shown in Models 1-3 in Table 5. In the comparison of sleeping habits, patients who originally had more than six hours of sleep (OR: 0.49, 95% CI: 0.28-0.86) and had sufficient sleep quality by using sleeping pills (OR: 0.45, 95% CI: 0.24-0.85) had better weight loss outcomes with semaglutide for three months than those who did not (Table 4). Additionally, patients who could extend their sleeping time to more than six hours (OR: 0.15, 95% CI: 0.06-0.38) or improve their sleep quality during the treatment period (OR: 0.21, 95% CI: 0.07-0.62) successfully maintained the therapeutically effective level of semaglutide for three months, regardless of whether lemborexant, a newer orexin receptor antagonist that promotes sleep, was used (Table 5). These results show the positive impact of sleeping habits on weight loss treatment.
Discussion
This real-world observational study elucidated the impact of sleeping habits on the weight loss efficacy of semaglutide in Japanese patients with obesity. It is recognized that having more than six hours of sleep a day and enough good-quality sleep play essential roles in achieving the expected treatment outcomes for weight reduction. Moreover, improving sleeping habits during treatment enhances the weight loss efficacy of semaglutide, which has both immediate and long-acting effects on weight reduction. These findings suggest that the therapeutic effect of oral GLP-1 RA can be improved by providing enough sleep, leading to sustained weight loss management for obese patients. Related factors, such as severe stress, late dinner after 9 PM, and less than three hours from dinner to bedtime, significantly interfered with the efficacy of weight loss treatment on the basis of their direct influence on sleeping habits.
With respect to both the immediate and long-lasting effects of semaglutide for weight reduction, obese people frequently experience a body weight plateau by six months after starting self-managed hypocaloric diets, even if the initial weight loss is successful [18,19]. Since long-term maintenance of weight loss was originally much more difficult, semaglutide can become a reliable support for obese individuals to overcome this challenge. Because its impact extended beyond just the weight loss phase, its involvement in weight reduction continues in the subsequent maintenance phase. Consequently, semaglutide is suitable as a first-choice drug for weight management on the basis of its favorable outcomes in many cases and its adverse events occurring in only a few cases in the study population.
A previous study reported that sleep and meal timing may influence food intake and appetite-related hormones in overweight and obese adults [30]. Another study confirmed that short sleep duration or poor sleep quality was associated with weight regain after successful weight loss in obese adults [31]. Additionally, a Japanese multicenter study revealed that shorter sleep duration is a significant risk factor for obesity [9]. Given these previous reports, our results provide further evidence that obese patients should improve their sleep habits regardless of the use of sleeping pills when starting treatment with GLP-1 RAs. To our knowledge, this is the first study showing that sleep amelioration during the treatment period leads to improved weight reduction with oral GLP-1 RA. The underlying mechanisms explaining the link between lack of sleep and diet intake are a homeostatic control through changes in the appetite-related hormones, including leptin and ghrelin [32]. Their hormones with GLP-1 have a complementary influence on the control of appetite. Thus, better sleep is recognized as an advantageous condition for obese patients receiving weight loss treatment.
Interestingly, obese women were more likely to experience weight loss with semaglutide, whereas there was no significant age difference in the therapeutic response according to our data. Regarding sex differences in the therapeutic efficacy of semaglutide, our data are consistent with a previous report that obese women can lose more weight than obese men when treated with GLP-1RAs for weight loss [33]. Estrogen, a female hormone that reduces food intake by potentially increasing the sensitivity of the female brain to anorexigenic peptides such as GLP-1, may be a factor influencing sex differences [34]. With respect to the lack of an age difference in the therapeutic efficacy of semaglutide, a recent study demonstrated that total daily energy expenditure is stable in adults aged 20-60 years, although it begins to decline slowly after the age of 60 years [35]. The influence of semaglutide on the suppression of total energy intake may be shown directly in the treatment outcome, which is based on almost the same total energy expenditure. Taken together, these results can potentially provide grounds for future obese patients who wish to undergo weight loss treatment with GLP-1 RAs.
This study has several limitations. First, the limited sample size and the single study site of the study participants are potential sources of selection bias. Second, this study exclusively targeted Japanese individuals with obesity and followed the Japanese guidelines for the management of obesity, which include different BMI thresholds (over 25 kg/m^2^) compared with those used in Western countries (over 30 kg/m^2^). Therefore, patients who were overweight (25 kg/m^2^ < BMI < 30 kg/m^2^) according to Western standards were also included in this study. Therefore, there might be different interpretations of the analyses based on race or ethnicity. Third, this study relies on self-reported data for variables such as sleep quality and stress levels. Because both sleep quality and stress levels are basically subjective, these evaluations are commonly conducted by the self-report method [36,37]. Objective measures of sleep quality, such as polysomnography, are expensive, time-consuming, and not readily available to most clinicians in our daily routine. Indeed, several self-report questionnaires, such as the Pittsburgh Sleep Quality Index and Insomnia Severity Index, have been developed and reported good internal reliability and validity [36]. The evaluation of stress level by self-reports illuminates the duration and severity of the psychological response to stressors. However, it is certainly true that biomarkers capture a more objective measure of stress and create a deeper understanding of the biological response to chronic and acute stress [37]. Finally, we focused only on oral GLP-1 RA as a therapeutic intervention to reduce the complexity of the analysis, even in the current situation in which a number of weight loss medications, including tirzepatide, a dual glucose-dependent insulinotropic polypeptide /GLP-1 receptor agonist, are available. Further comprehensive investigations with validated objective measures of sleep quality and stress in larger populations are needed to obtain positive evidence of our findings.
Conclusions
This observational study shows that sleeping habits can have a positive effect on weight loss efficacy with oral GLP-1 RA in obese patients in real-world clinical practice, particularly women, regardless of age. Moreover, improving sleeping habits during treatment enhances the weight loss efficacy of semaglutide. Conversely, severe stress and late dinner have a negative influence on the weight loss effect of semaglutide. Because of its immediate and long-term effects and relatively low risk of adverse events, semaglutide is well suited for weight management as a first-choice drug for obese individuals with uncontrolled weight gain. Multicenter studies are required in the future to support the current findings and thoroughly investigate the underlying biological mechanisms linking sleep and semaglutide efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO acceleration plan to stop obesity 2023 https://www.who.int/publications/i/item/9789240075634
- 2An overview of obesity-related complications: the epidemiological evidence linking body weight and other markers of obesity to adverse health outcomes Diabetes Obes Metab Blüher M 31927 Suppl 2202510.1111/dom.16263 PMC 1200086040069923 · doi ↗ · pubmed ↗
- 3Obesity as a disease: the Obesity Society 2018 position statement Obesity (Silver Spring) Jastreboff AM Kotz CM Kahan S Kelly AS Heymsfield SB 792720193056964110.1002/oby.22378 · doi ↗ · pubmed ↗
- 4Real-world evidence on the utilization, clinical and comparative effectiveness, and adverse effects of newer GLP-1RA-based weight-loss therapies Diabetes Obes Metab Thomsen RW Mailhac A Løhde JB Pottegård A 668827 Suppl 220254019693310.1111/dom.16364 PMC 12000858 · doi ↗ · pubmed ↗
- 5Glucagon-like peptide 1 (GLP-1) receptor variants and glycemic response to liraglutide: a pharmacogenetics study in Iranian people with type 2 diabetes mellitus Adv Ther Eghbali M Alaei-Shahmiri F Hashemi-Madani N Emami Z Mostafavi L Malek M Khamseh ME 8268364120243817237710.1007/s 12325-023-02761-1 · doi ↗ · pubmed ↗
- 6Effect of GLP-1R rs 2254336 and rs 3765467 polymorphisms on gastrointestinal adverse reactions in type 2 diabetes patients treated with liraglutide Eur J Clin Pharmacol Long J Liu Y Duan Y 5895967820223503415010.1007/s 00228-021-03225-7 · doi ↗ · pubmed ↗
- 7A pilot study investigating the influence of glucagon-like peptide-1 receptor single nucleotide polymorphisms on gastric emptying rate in Caucasian men Front Physiol Yau AM Mc Laughlin J Maughan RJ Gilmore W Ashworth JJ Evans GH 1331920183031944310.3389/fphys.2018.01331 PMC 6167426 · doi ↗ · pubmed ↗
- 8Genetic variability in GLP-1 receptor is associated with inter-individual differences in weight lowering potential of liraglutide in obese women with PCOS: a pilot study Eur J Clin Pharmacol Jensterle M PiršB Goričar K Dolžan V JanežA 8178247120152599105110.1007/s 00228-015-1868-1 · doi ↗ · pubmed ↗