Depression and Anxiety Among Obese and Overweight Individuals in Saudi Arabia: A Systematic Review and Meta-Analysis
Amer H Alshahre, Saad A Alqahtani, Maryam S Alsharif, Alaa A Alyahya, Maher A Alsmail, Abdulaziz S Almasabi, Waleed S Abumelha

TL;DR
This study finds that obesity in Saudi Arabia is linked to higher rates of severe depression and anxiety, highlighting the need for mental health support for overweight individuals.
Contribution
The study provides the first meta-analysis on the mental health impact of obesity in Saudi Arabia, revealing significant associations with severe depression and anxiety.
Findings
Obesity is significantly associated with severe depression (OR = 1.76) and severe anxiety (OR = 1.62) in Saudi Arabia.
Overweight individuals show a significant link to severe anxiety (OR = 1.46), but not depression.
The prevalence of depression and anxiety among obese individuals is 25.02% and 29.23%, respectively.
Abstract
The escalating prevalence of obesity in Saudi Arabia raises concerns about its impact on mental health. This meta-analysis explores the associations between obesity and the prevalence of depression and anxiety within the distinctive cultural context of Saudi Arabia. A systematic review identified 12 cross-sectional studies conducted in Saudi Arabia, collectively involving 17,232 participants. Pooled effect sizes were calculated for depression and anxiety outcomes among obese and overweight individuals. Heterogeneity was assessed, and subgroup analyses were planned to explore potential sources of variation. The meta-analysis revealed a significant association between obesity and overall depression (OR = 1.42, 95% CI (1.07, 1.87)), severe depression (OR = 1.76, 95% CI (1.08, 2.86)), and severe anxiety (OR = 1.62, 95% CI (1.24, 2.11)). Severe anxiety was also significantly associated with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
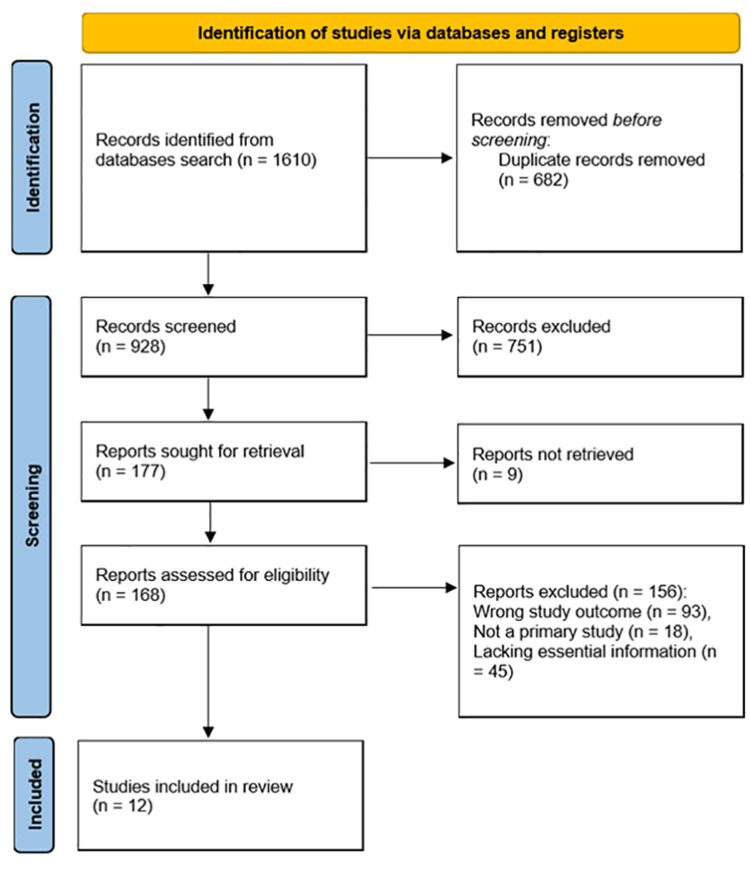 Figure 1
Figure 1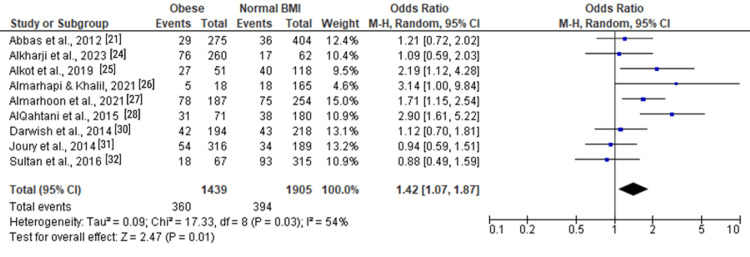 Figure 2
Figure 2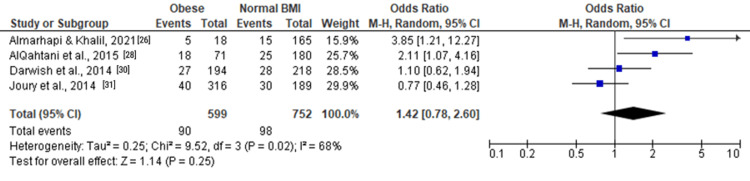 Figure 3
Figure 3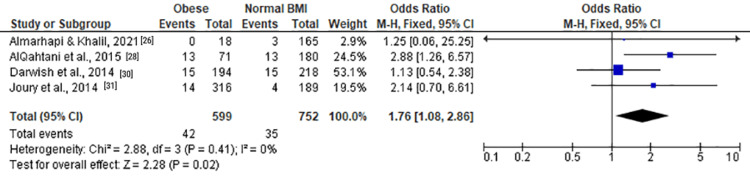 Figure 4
Figure 4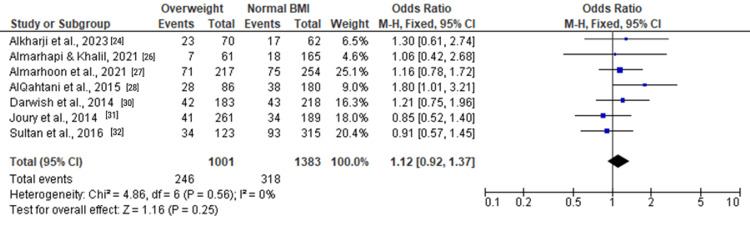 Figure 5
Figure 5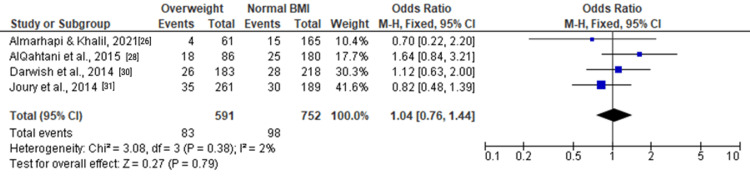 Figure 6
Figure 6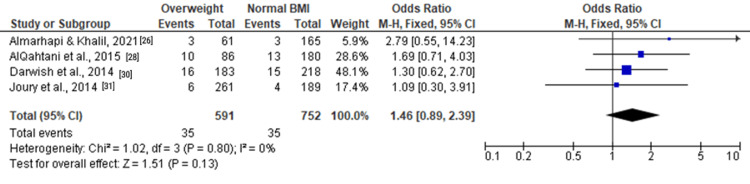 Figure 7
Figure 7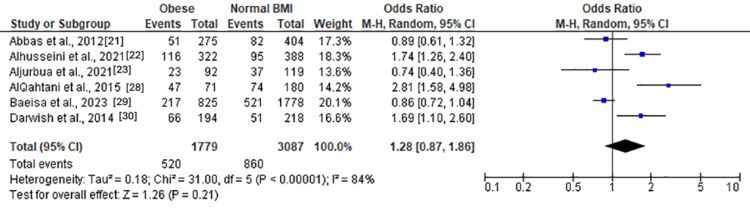 Figure 8
Figure 8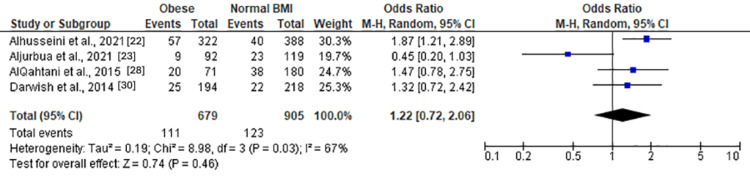 Figure 9
Figure 9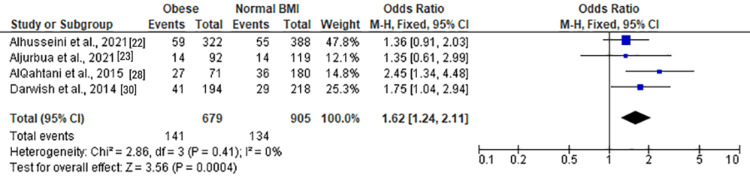 Figure 10
Figure 10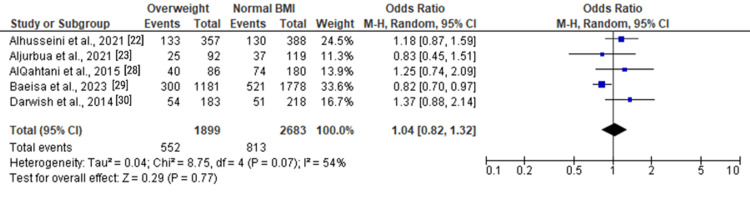 Figure 11
Figure 11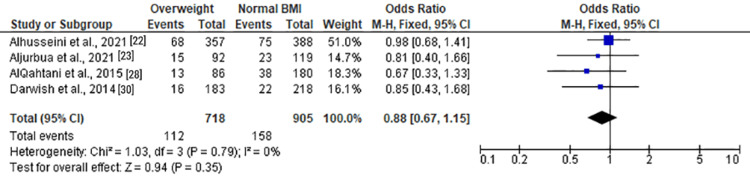 Figure 12
Figure 12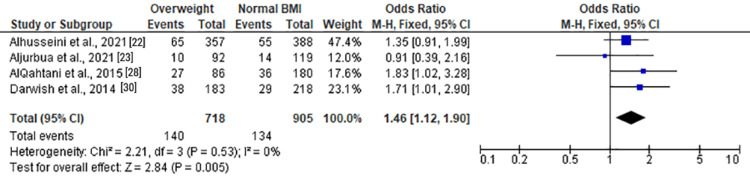 Figure 13
Figure 13| Study | Study design | Study setting | City | Study duration | Population type | Population number | Age (year) | Males (%) | Normal BMI (%) | Overweight (%) | Obese (%) | Diagnostic tool for depression | Diagnostic tool for anxiety | Overall depression rate among the entire population (%) | Overall anxiety rate among the entire population (%) |
| Abbas et al. (2012) [ | Cross-sectional study | Hospital-based | Riyadh | 2011 | Nurses | 715 | 35.2 ± 8.2 | 11.60% | 56.50% | Overweight and obese: 38.46% | HAD-D | HAD-A | 10% | 20% | |
| Alhusseini et al. (2021) [ | Cross-sectional study | Community-based | Nonspecific | 2020 | General public | 1,123 | 18-29 | 29.11% | 34.55% | 31.79% | 28.67% | NA | GAD-7 | NA | 36.33% |
| Aljurbua et al. (2021) [ | Cross-sectional study | Community-based | Nonspecific | 2021 | General public in KSA | 338 | 18-64 | 39.30% | 36.30% | 28% | 28% | NA | GAD-7 | NA | 29% |
| Alkharji et al. (2023) [ | Cross-sectional study | Hospital-based | Jeddah | 2023 | Adults visiting PHCCs | 397 | NR | 56.90% | 15.60% | 17.60% | 65.50% | PHQ-9 | NA | 29.70% | NA |
| Alkot et al. (2019) [ | Cross-sectional study | Community-based | Makkah | 2018-2019 | Diabetic population | 169 | 40.27 + 15.95 | 69.20% | NR | NR | 30.20% | BDI-II | NA | 24.30% | NA |
| Almarhapi and Khalil (2021) [ | Cross-sectional study | Hospital-based | Tabuk | 2021 | Healthcare workers | 255 | 30.6 ± 5.3 | 41.20% | 64.70% | 23.90% | 7.10% | PHQ-9 | NA | 11.76% | NA |
| Almarhoon et al. (2021) [ | Cross-sectional study | Community-based | Eastern Province | 2020-2021 | Saudi adults | 711 | 18-65 | 24.90% | 35.70% | 30.50% | 26.40% | PHQ-9 | NA | 34.80% | NA |
| AlQahtani et al. (2015) [ | Cross-sectional study | Community-based | Abha | 2013-2014 | Male university students | 389 | 21.2 ± 1.5 | 100% | 46.20% | 22.10% | 18.30% | DASS | DASS | 29.30% | 48.30% |
| Baeisa et al. (2023) [ | Cross-sectional study | Community-based | Nonspecific | 2021-2023 | General public | 4,224 | 31.12 ± 11 | 39.10% | 42% | 27.96% | 19.53% | NA | GAD-7 | NA | 29% |
| Darwish et al. (2014) [ | Cross-sectional study | Hospital-based | Qatif | 2013-2014 | Public attending PHCCs | 630 | 34.3 ± 9.3 | 0% | 34.60% | 29% | 36% | DASS | DASS | 21.40% | 29.20% |
| Joury (2014) [ | Cross-sectional study | Community-based | Riyadh | 2012 | General public | 787 | NR | 69.80% | 24% | 33.16% | 40.15% | BDI-II | NA | 17.40% | NA |
| Sultan et al. (2016) [ | Cross-sectional study | Community-based | Madina | 2014 | Medical students | 555 | NR | 47% | 56.75% | 22.16% | 12.07% | PQ-2 | NA | 28.28% | NA |
| Measure | Number of studies | Participants (N) | Prevalence (%) | Heterogeneity | Model | OR | Test for overall effect |
| Depression among obese individuals | |||||||
| Moderate and severe depression | 9 | 3,344 | 25.02% | Tau² = 0.09; Chi² = 17.33, df = 8 (P = 0.03); I² = 54% | RE | 1.42 (1.07, 1.87) | Z = 2.47 (P = 0.01) |
| Moderate depression | 4 | 1,351 | 15.03% | Tau² = 0.25; Chi² = 9.52, df = 3 (P = 0.02); I² = 68% | RE | 1.42 (0.78, 2.60]) | Z = 1.14 (P = 0.25) |
| Severe depression | 4 | 1,351 | 7.01% | Chi² = 2.88, df = 3 (P = 0.41); I² = 0% | FE | 1.76 (1.08, 2.86) | Z = 2.28 (P = 0.02) |
| Depression among overweight individuals | |||||||
| Moderate and severe depression | 7 | 2,384 | 24.58% | Chi² = 4.86, df = 6 (P = 0.56); I² = 0% | FE | 1.12 (0.92, 1.37) | Z = 1.16 (P = 0.25) |
| Moderate depression | 4 | 1,343 | 14.04% | Chi² = 3.08, df = 3 (P = 0.38); I² = 2% | FE | 1.04 (0.76, 1.44) | Z = 1.16 (P = 0.25) |
| Severe depression | 4 | 1,343 | 5.92% | Chi² = 1.02, df = 3 (P = 0.80); I² = 0% | FE | 1.46 (0.89, 2.39) | Z = 1.51 (P = 0.13) |
| Anxiety among obese individuals | |||||||
| Moderate and severe anxiety | 6 | 4,866 | 29.23% | Tau² = 0.18; Chi² = 31.00, df = 5 (P < 0.00001); I² = 84% | RE | 1.28 (0.87, 1.86) | Z = 1.26 (P = 0.21) |
| Moderate anxiety | 4 | 1,584 | 16.35% | Tau² = 0.19; Chi² = 8.98, df = 3 (P = 0.03); I² = 67% | RE | 1.22 (0.72, 2.06) | Z = 0.74 (P = 0.46) |
| Severe anxiety | 4 | 1,584 | 20.77% | Chi² = 2.86, df = 3 (P = 0.41); I² = 0% | FE | 1.62 (1.24, 2.11) | Z = 3.56 (P = 0.0004) |
| Anxiety among overweight individuals | |||||||
| Moderate and severe anxiety | 5 | 4,582 | 29.07% | Tau² = 0.04; Chi² = 8.75, df = 4 (P = 0.07); I² = 54% | RE | 1.04 (0.82, 1.32) | Z = 0.29 (P = 0.77) |
| Moderate anxiety | 4 | 1,623 | 15.59% | Chi² = 1.03, df = 3 (P = 0.79); I² = 0% | FE | 0.88 (0.67, 1.15) | Z = 0.94 (P = 0.35) |
| Severe anxiety | 4 | 1,623 | 19.49% | Chi² = 1.03, df = 3 (P = 0.79); I² = 0% | FE | 1.46 (1.12, 1.90) | Z = 2.84 (P = 0.005) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObesity and Health Practices · Health and Lifestyle Studies · Cardiac Health and Mental Health
Introduction and background
The Kingdom of Saudi Arabia has witnessed a remarkable epidemiological transition over the past few decades, marked by a surge in noncommunicable diseases [1,2]. Among these, obesity stands out as a pressing public health concern, with far-reaching implications for both physical and mental well-being [3]. As the prevalence of obesity continues to rise globally, the complex interplay between excess body weight and mental health outcomes has garnered increased attention [4].
Saudi Arabia, like many countries worldwide, has experienced a significant increase in the prevalence of obesity [5]. Rapid urbanization, changes in dietary patterns, and sedentary lifestyles have contributed to the escalating rates of overweight and obesity in the population [6]. According to national surveys, the prevalence of obesity among adults in Saudi Arabia has surged from 22.4% in 1995 to 35.4% in 2017, underscoring the urgency of addressing this burgeoning epidemic [4-7].
The consequences of obesity extend beyond physical health, encompassing a spectrum of mental health outcomes [8]. The intricate relationships between obesity, depression, and anxiety have been a subject of extensive research globally [8-12]. However, understanding these connections within the specific cultural and contextual nuances of Saudi Arabia is vital for tailoring effective public health interventions.
Mounting evidence suggests bidirectional associations between obesity and mental health conditions. Individuals with obesity may experience stigma, discrimination, and societal pressure, contributing to psychosocial distress [13,14]. Concurrently, mental health challenges may influence behaviors related to diet and physical activity, exacerbating the risk of obesity. This reciprocal relationship creates a complex web that warrants careful examination [15].
Depression and anxiety, two prevalent mental health disorders, have been consistently linked to obesity in diverse populations [16]. The psychosocial impact of obesity, coupled with potential physiological mechanisms involving inflammation and hormonal dysregulation, forms the basis for exploring these associations [17]. Understanding the nuanced nature of these relationships is crucial for informing comprehensive healthcare strategies that address the dual burden of obesity and mental health issues [18,19].
While individual studies have explored the connections between obesity, depression, and anxiety in Saudi Arabia, synthesizing the existing evidence through a meta-analysis provides the highest level of evidence-based medicine. This approach allows for the quantification of associations, the identification of patterns across diverse populations, and the exploration of potential sources of heterogeneity. Moreover, a meta-analysis enables the examination of the collective impact of obesity on varying degrees of depression and anxiety, shedding light on the nuances of these relationships. This meta-analysis aims to explore the associations between obesity and two prevalent mental health conditions, depression and anxiety, within the sociocultural context of Saudi Arabia, which will subsequently contribute to the general literature on this subject.
Review
Materials and methods
This study is a meta-analysis that adhered to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, ensuring transparency and completeness in reporting the study methodology and results. The PRISMA checklist was systematically followed to enhance the rigor and reproducibility of the meta-analysis [20]. The methodology commenced with an exhaustive literature search conducted across electronic databases, including PubMed, Scopus, and PsycINFO, covering articles published up to the cutoff date of January 2022. The search strategy utilized a combination of controlled vocabulary (MeSH terms) and free-text keywords related to depression, anxiety, obesity, overweight, and Saudi Arabia. Boolean operators (AND, OR) were employed to refine the search and ensure inclusivity.
Study Search and Screening Process
Inclusion criteria were systematically applied at each stage of the screening process. Duplicates were identified and removed. Title and abstract screening followed, with records undergoing evaluation based on predetermined eligibility criteria. Studies were included if they were cross-sectional in design, conducted in Saudi Arabia, focused on individuals with obesity or overweight status, and reported quantitative data on the prevalence of depression and anxiety. Subsequently, studies were sought for retrieval, and the remaining studies were meticulously assessed for eligibility by two independent reviewers. Studies that did not meet the inclusion criteria or lacked relevant outcome measures were excluded.
Data Extraction
A standardized data extraction form was developed to systematically extract relevant information from the included studies. Two independent reviewers extracted data, including study characteristics (e.g., author and publication year), study design, setting, city, study duration, population type, population number, age distribution, sex distribution, BMI trends, diagnostic tools for depression and anxiety, and overall rates of depression and anxiety. For each outcome of interest (depression and anxiety), data on prevalence, ORs, and associated 95% CIs were extracted. Special attention was given to data related to different levels of depression and anxiety, such as moderate and severe categories, when reported by the included studies.
Statistical Analysis
The statistical synthesis involved the use of the Review Manager software, version 5.4. Pooled effect sizes (ORs) were calculated for each outcome of interest using a random-effects model to account for potential heterogeneity among the included studies. The I² statistic was used to assess heterogeneity. Forest plots were generated to visually represent the effect sizes and associated CIs for each outcome. Subgroup analyses were planned to explore potential sources of heterogeneity. Additionally, publication bias was evaluated using funnel plots and Egger’s regression test.
Results
A systematic review of the literature was conducted, yielding 1610 records, from which 682 duplicates were removed. After title and abstract screening, 928 records were enrolled, leading to the exclusion of 751 studies. Subsequently, 177 records were retrieved, with nine studies not obtained. A total of 168 studies were assessed for eligibility, and 156 were excluded, resulting in 12 studies being included in the meta-analysis (Figure 1).
PRISMA flow diagram for summary of the study selection processPRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses
Characteristics of the Included Studies
Table 1 provides a summary of the included studies.
All studies adopted a cross-sectional study design. The settings varied, including hospital-based studies such as Abbas et al. (2012) [21], Alkharji et al. (2023) [24], Almarhapi and Khalil (2021) [26], and Darwish et al. (2014) [30]. Community-based studies were conducted by Alhusseini et al. (2021) [22], Aljurbua et al. (2021) [23], Alkot et al. (2019) [25], Almarhoon et al. (2021) [27], AlQahtani et al. (2015) [28], Baeisa et al. (2023) [29], Joury (2014) [31], and Sultan et al. (2016) [32]. The studies were conducted in various cities, including Riyadh, Jeddah, Makkah, Tabuk, Eastern Province, Abha, and Qatif. The durations of the studies ranged from 2011 to 2023, with a focus on different time periods.
The populations under investigation were diverse, encompassing nurses [21], the general public [22,23,26,27,29,31], adults visiting primary health care centers [24], diabetic population [25], healthcare workers [26], male university students [28], and medical students [32]. The population numbers ranged from 169 to 4,224.
Age distribution varied across studies, with age ranges specified for each study. Males constituted different percentages, ranging from 0% [30] to 100% [28]. BMI trends showed variability, with studies reporting the percentage of normal weight, overweight, and obese individuals.
Studies utilized various tools for assessing depression and anxiety. The Hospital Anxiety and Depression Scale (HAD-D and HAD-A) was used in Abbas et al. (2012) [21], and the Depression, Anxiety, and Stress Scale (DASS) in AlQahtani et al. (2015) [28] and Darwish et al. (2014) [30]. The Patient Health Questionnaire-9 (PHQ-9) was employed by Alkharji et al. (2023) [24] and Almarhoon et al. (2021) [27], and the Beck Depression Inventory-II (BDI-II) in Alkot et al. (2019) [25] and Joury et al. (2014) [31]. The Generalized Anxiety Disorder 7-item scale (GAD-7) was used in Alhusseini et al. (2021) [22], Aljurbua et al. (2021) [23], Almarhapi and Khalil (2021) [26], and Baeisa et al. (2023) [29]. Sultan et al. (2016) [32] used the Patient Health Questionnaire-2 (PHQ-2).
Depression rates ranged from 10% to 34.8%, with the highest rate observed in Almarhoon et al. (2021) [27]. Anxiety rates ranged from 20% to 48.3%, with the highest rate reported in AlQahtani et al. (2015) [28].
Quantitative Data Synthesis
Table 2 presents the pooled effect sizes and heterogeneity assessment for the assessed outcomes, offering a comprehensive overview of the prevalence of depression and anxiety among both obese and overweight individuals in Saudi Arabia.
Depression Among Obese Individuals
For moderate and severe depression (Figure 2), the pooled OR was 1.42 (1.07, 1.87), indicating a significant association with obesity (Z = 2.47, P = 0.01). Moderate depression (Figure 3) showed a similar trend with an OR of 1.42 (0.78, 2.60), although not statistically significant (Z = 1.14, P = 0.25). Severe depression (Figure 4) demonstrated a significant association with obesity, with an OR of 1.76 (1.08, 2.86) (Z = 2.28, P = 0.02).
Forest plot of moderate and severe depression among obese versus normal BMI individuals
Forest plot of moderate depression among obese versus normal BMI individuals
Forest plot of severe depression among obese versus normal BMI individuals
Depression Among Overweight Individuals
Among overweight individuals, the forest plots in Figure 5, Figure 6, and Figure 7 depicted no statistically significant associations with depression. The ORs for moderate and severe depression were 1.12 (0.92, 1.37), 1.04 (0.76, 1.44), and 1.46 (0.89, 2.39), respectively.
Forest plot of moderate and severe depression among overweight versus normal BMI individuals
Forest plot of moderate depression among overweight versus normal BMI individuals
Forest plot of severe depression among overweight versus normal BMI individuals
Anxiety Among Obese Individuals
Moderate and severe anxiety (Figure 8) revealed a nonsignificant association with obesity (OR = 1.28 (0.87, 1.86), Z = 1.26, P = 0.21). Moderate anxiety (Figure 9) also exhibited a nonsignificant association (OR = 1.22 (0.72, 2.06), Z = 0.74, P = 0.46). However, severe anxiety (Figure 10) demonstrated a significant association with obesity, with an OR of 1.62 (1.24, 2.11) (Z = 3.56, P = 0.0004). Heterogeneity was absent (Chi² = 2.86, df = 3, P = 0.41; I² = 0%).
Forest plot of moderate and severe anxiety among obese versus normal BMI individuals
Forest plot of moderate anxiety among obese versus normal BMI individuals
Forest plot of severe anxiety among obese versus normal BMI individuals
Anxiety Among Overweight Individuals
Among overweight individuals, the forest plots in Figure 11 and Figure 12 illustrated no statistically significant associations with anxiety. The ORs for overall and moderate anxiety were 1.04 (0.82, 1.32) and 0.88 (0.67, 1.15), respectively. Severe anxiety, as shown in Figure 13, was significantly associated with overweight status with an OR of 1.46 (1.12, 1.90) (Z = 2.84, P = 0.005).
Forest plot of moderate and severe anxiety among overweight versus normal BMI individuals
Forest plot of moderate anxiety among overweight versus normal BMI individuals
Forest plot of severe anxiety among overweight versus normal BMI individuals
Discussion
Obesity is a global health concern with multifaceted implications, and its association with mental health, particularly depression and anxiety, has garnered significant research interest [33,34]. In the context of Saudi Arabia, where the prevalence of obesity is escalating, understanding the interplay between obesity and mental health is crucial [35]. This meta-analysis aimed to consolidate and analyze data from 12 cross-sectional studies to elucidate the prevalence of depression and anxiety among obese and overweight individuals in Saudi Arabia.
Our meta-analysis yielded compelling insights into the relationship between obesity and mental health in the Saudi Arabian population. In terms of depression among obese individuals, the pooled OR for overall depression was 1.42 (1.07, 1.87), indicating a significant association. Moreover, the observed OR for severe depression was 1.76 (1.08, 2.86), reinforcing the association between obesity and more severe forms of depressive symptoms [36,37]. These results coincide with the growing body of literature suggesting that obesity is a risk factor for the development and exacerbation of depression, as highlighted in studies such as AlQahtani et al. (2015) [28].
Contrastingly, the analysis of depression among overweight individuals did not reveal statistically significant associations. This nuanced difference in the association between depression and different weight statuses echoes the findings of Baeisa et al. (2023) [29], where depression rates were observed in the general public but did not show a significant correlation with overweight status.
As regards anxiety, our findings demonstrate that among obese individuals, severe anxiety exhibited a significant association with an OR of 1.62 (1.24, 2.11). However, the associations with moderate anxiety and moderate and severe anxiety combined did not reach statistical significance. This mirrors the complexity of the relationship between obesity and anxiety [38], as suggested by Alhusseini et al. (2021) [22], who found a nonsignificant association in a community-based study.
Similarly, among overweight individuals, our analysis did not unveil statistically significant associations with overall or moderate anxiety. These results are in line with the findings of Joury et al. (2014) [31], where anxiety rates in the general public in Riyadh did not exhibit a significant correlation with overweight status. However, the study found a significant association between overweight state and severe anxiety [39].
The observed significant association between obesity and both severe depression and severe anxiety underscores the need for comprehensive mental health interventions among individuals with higher BMIs [37,39,40]. Our findings align with previous meta-analyses and systematic reviews that have identified obesity as a risk factor for the development and exacerbation of depressive and anxiety disorders [41-43].
The intricate interplay between obesity and mental health can be attributed to various factors, including biological mechanisms, societal stigmatization, and lifestyle factors [41]. Biological mechanisms involve the impact of adipose tissue on inflammatory processes and hormonal imbalances, contributing to changes in brain function and mood regulation. Societal stigmatization may result in increased stress and decreased self-esteem, further exacerbating mental health issues [38]. Additionally, lifestyle factors such as physical inactivity and poor dietary habits may contribute to both obesity and mental health disorders [39].
The implications of our findings extend beyond the academic realm, influencing public health strategies and interventions in Saudi Arabia. The significant associations between obesity and severe mental health outcomes underscore the need for integrated healthcare approaches that address both physical and mental well-being [43]. Public health interventions should prioritize early detection and management of mental health issues among individuals with higher BMIs [38].
Tailored interventions that consider cultural nuances and societal perceptions of obesity can enhance the effectiveness of mental health programs in Saudi Arabia. Addressing the stigma associated with obesity and fostering a supportive environment are crucial components of holistic healthcare strategies [42,43]. Collaboration between healthcare providers, policymakers, and community stakeholders is imperative to develop and implement comprehensive programs that address the complex interplay between obesity and mental health.
While our study provides insights, it is essential to acknowledge certain limitations. The cross-sectional nature of the included studies prevents the establishment of causal relationships. Additionally, variations in study populations, assessment tools, and methodologies may contribute to heterogeneity. Future research should prioritize longitudinal designs to elucidate the temporal dynamics of the obesity-mental health relationship and consider diverse population groups.
Conclusions
Our meta-analysis contributes insights into the relationship between obesity and mental health in Saudi Arabia, which will subsequently contribute to the general knowledge of the subject. The significant associations observed with severe depression and anxiety emphasize the need for a holistic approach to healthcare that integrates mental health considerations into obesity management strategies. These findings have direct implications for public health policies, calling for the development of targeted interventions that address the complex interplay between physical and mental well-being in individuals with higher BMIs in Saudi Arabia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States Obes Rev Ng SW Zaghloul S Ali HI Harrison G Popkin BM 11312201110.1111/j.1467-789X.2010.00750.x 20546144 · doi ↗ · pubmed ↗
- 2Non-communicable diseases in the Arab world Lancet Rahim HF Sibai A Khader Y 35636738320142445204410.1016/S 0140-6736(13)62383-1 · doi ↗ · pubmed ↗
- 3Prevalence, risk factors, and interventions for obesity in Saudi Arabia: a systematic review Obes Rev Salem V Al Husseini N Abdul Razack HI Naoum A Sims OT Alqahtani SA 023202210.1111/obr.13448 PMC 928700935338558 · doi ↗ · pubmed ↗
- 4Obesity and public health in the Kingdom of Saudi Arabia Rev Environ Health De Nicola E Aburizaiza OS Siddique A Khwaja H Carpenter DO 1912053020152635180110.1515/reveh-2015-0008 · doi ↗ · pubmed ↗
- 5Trends and future projections of the prevalence of adult obesity in Saudi Arabia, 1992-2022 East Mediterr Heal J Al Quwaidhi AJ Pearce MS Critchley JA Sobngwi E O’Flaherty M 58959520201425356689 · pubmed ↗
- 6Obesity and associated factors — Kingdom of Saudi Arabia, 2013 Prev Chronic Dis Memish ZA El Bcheraoui C Tuffaha M 011201410.5888/pcd 11.140236 PMC 419306025299980 · doi ↗ · pubmed ↗
- 7Overweight and obesity among adults in the Gulf States: a systematic literature review of correlates of weight, weight-related behaviours, and interventions Obes Rev Balhareth A Meertens R Kremers S Sleddens E 7637932020193065380310.1111/obr.12826 PMC 6850146 · doi ↗ · pubmed ↗
- 8Diet, obesity, and depression: a systematic review J Pers Med Patsalos O Keeler J Schmidt U Penninx BW Young AH Himmerich H 1761120213380248010.3390/jpm 11030176 PMC 7999659 · doi ↗ · pubmed ↗