Scrub Typhus Masquerading As Infectious Mononucleosis: A Case Report
Tomoko Yasuda, Takaaki Kobayashi, Kazuaki Aoki, Masayuki Nogi

TL;DR
A 74-year-old man's scrub typhus was initially mistaken for infectious mononucleosis due to overlapping symptoms, highlighting the need for careful diagnosis.
Contribution
This case report highlights the atypical presentation of scrub typhus and the diagnostic challenges it can pose.
Findings
Scrub typhus can present without a rash and mimic infectious mononucleosis.
A physical examination and serology confirmed scrub typhus after initial misdiagnosis.
Early detection and treatment with tetracycline led to full recovery.
Abstract
Scrub typhus is a tick-borne disease caused by the intracellular organism Orientia tsutsugamushi. It typically presents with the cardinal "triad" of fever, rash, and eschar, along with other nonspecific symptoms. We report a case of scrub typhus in a 74-year-old man who did not exhibit the typical rash. He presented to the emergency room with a one-week history of generalized symptoms, including fever, throat pain, and myalgia, and was admitted due to suspected cholangitis based on elevated liver enzymes. However, computed tomography (CT) and magnetic resonance cholangiopancreatography (MRCP) ruled out this diagnosis. A transient rash developed after the initiation of antibiotics, considered to be a drug reaction. Further laboratory workup showed mildly positive results for cytomegalovirus (CMV)-IgM, and subsequent tests revealed an elevation of atypical lymphocytes, leading to a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
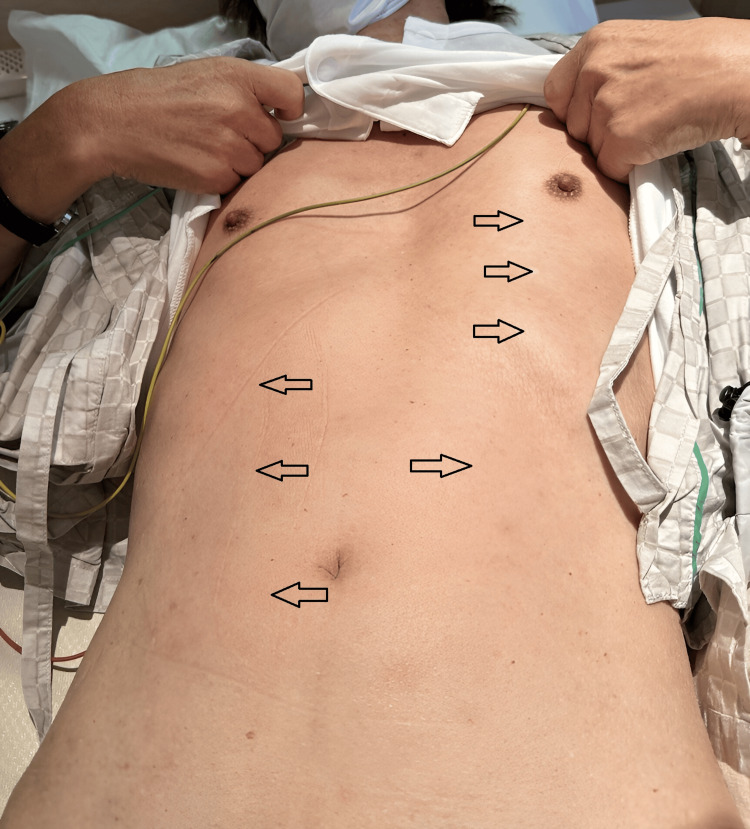 Figure 1
Figure 1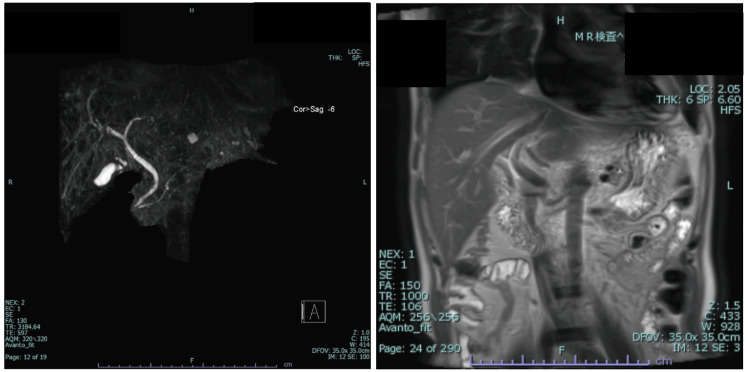 Figure 2
Figure 2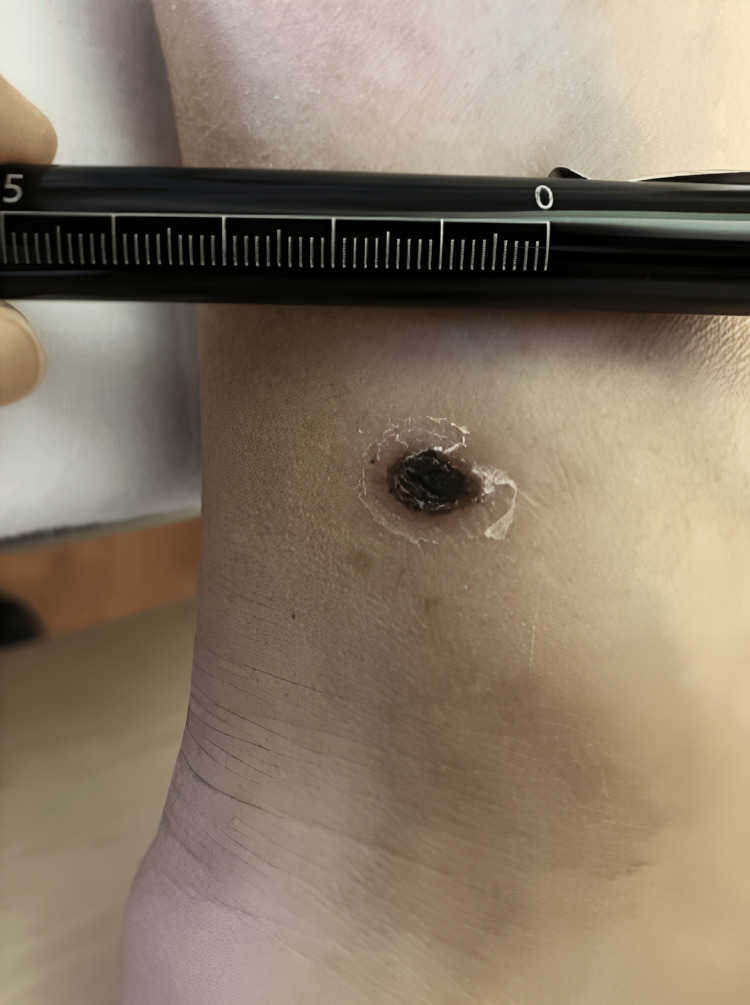 Figure 3
Figure 3| Parameter | Day 1 | Day 3 | Day 6 | Day 10 | Reference |
| WBC (102/mcL) | 110 | 68 | 44 | 57 | 33-86 |
| Neutro (%) | 86.0 | 72.0 | 45.0 | 55.6 | 42.4-75.0 |
| Lymph (%) | 10 | 21 | 42 | 34.4 | 16-49 |
| At-lymph (%) | 0.0 | 4.0 | 3.0 | 0.0 | 0 |
| Hb (g/dL) | 12.9 | 12.0 | 12.2 | 12.6 | 11.6-14.8 |
| Plt (104/mcL) | 21.9 | 20.9 | 33.7 | 46.4 | 15.8-34.8 |
| AST (U/L) | 150 | 153 | 102 | 40 | 13-30 |
| ALT (U/L) | 153 | 136 | 112 | 73 | 7-23 |
| LD (U/L) | 346 | 336 | 228 | 208 | 124-22 |
| ALP (U/L) | 495 | 417 | 347 | 286 | 38-113 |
| GGT (U/L) | 373 | 351 | 338 | 314 | 9-32 |
| T-bil (mg/dL) | 1.4 | 0.8 | 0.7 | 0.9 | 0.4-1.5 |
| D-bil (mg/dL) | 0.9 | 0.5 | 0.4 | 0.4 | 0.0-0.4 |
| CRP (mg/dL) | 20.75 | 10.93 | 2.52 | 0.40 | 0.00-0.14 |
| Test | Day 1 | Day 4 | Day 20 |
| CMV-IgM | Positive | - | Inconclusive |
| Index (reference: 0.01-0.99) | 1.01 | - | 0.86 |
| CMV-IgG | Positive | - | Positive |
| Index (reference: 0.00-5.99) | 153 | - | 183 |
| HIV 1/2 CLIA | Negative | - | Negative |
| Index (reference: 0.00-0.99) | 0.100 | - | 0.100 |
|
| |||
| IgM Kato | 2560 | ||
| IgG Kato | 640 | ||
| IgM Karp | 10> | ||
| IgG Karp | 160 | ||
| IgM Gilliam | 2560 | ||
| IgG Gilliam | 640 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMosquito-borne diseases and control · Vector-Borne Animal Diseases · Vector-borne infectious diseases
Introduction
Scrub typhus is a vector-borne disease endemic to the Asia-Pacific region, caused by the intracellular organism *Orientia tsutsugamushi *and transmitted by ticks and mites. An estimated one million people are infected worldwide each year, but the true incidence remains unknown due to substantial under-recognition and frequent misdiagnosis, including in Japan [1,2]. While fever, rash, and eschar constitute the classical clinical "triad," symptoms are often wide-ranging and non-specific, mimicking other febrile diseases. Both diagnosis by serological testing and vaccine development have been complicated by the pathogen’s genetic diversity [3]. Prompt recognition and treatment are critical, as delayed therapy can result in severe complications, including death [1]. We report a case of a 74-year-old man with scrub typhus in whom diagnosis and treatment were delayed due to the lack of a characteristic rash and a clinical course mimicking cytomegalovirus (CMV) mononucleosis. This case highlights the diagnostic challenges of scrub typhus, especially when typical features are absent or serological results are confounded.
Case presentation
A 74-year-old male presented to the emergency department with a one-week history of fever and chills. Associated symptoms included bilateral lower leg myalgia, xerostomia, headache, diarrhea, nausea, pharyngeal pain, and loss of appetite. He denied other respiratory symptoms, rash, abdominal pain, muscle wasting, night sweats, or significant weight loss. He had not sought medical attention for the past 20 years, except for three dentist appointments in the past month for dental bridges. Otherwise, he was allegedly healthy, took no medications, and frequently took long walks in nearby forests. He reported having unprotected sexual intercourse with a commercial sex worker one week prior to the onset of fever. He denied alcohol consumption, recreational drug use, and international or domestic travel.
At the time of presentation, his blood pressure was 134/75 mmHg, heart rate 110 beats per minute, respiratory rate 16 breaths per minute, peripheral oxygen saturation (SpO_2_) 96% on room air, and body temperature was 39.6°C. Physical examination was notable for bilateral posterior cervical lymphadenopathy but was otherwise unremarkable. There was no pharyngeal erythema, scleral icterus, palpable tenderness to abdominal or hepatic regions, decreased muscle tone, or motor weakness throughout. Skin findings lacked rashes, splinter hemorrhages, or petechiae. Laboratory workup revealed mild leukocytosis with neutrophilic predominance and no atypical lymphocytes (white blood cell count: 11,000/mcL; neutrophils: 86.0%; hemoglobin: 12.9 g/dL; platelets: 219,000/mcL). Liver enzymes were elevated, with aspartate transaminase (AST) at 150 U/L, alanine transaminase (ALT) at 153 U/L, alkaline phosphatase (ALP) at 495 U/L, gamma-glutamyl transferase (GGT) at 373 U/L, total bilirubin at 1.4 mg/dL, and direct bilirubin at 0.9 mg/dL. He was admitted with a provisional diagnosis of cholangitis, based on fever and elevated liver enzymes, and was started on intravenous ampicillin-sulbactam.
The following day, he developed a nonpruritic, erythematous rash from his abdomen to his thighs, which completely resolved immediately after antibiotic discontinuation (Figure 1). This rash was non-specific and considered to be an antibiotic-related drug rash. Computed tomography (CT) revealed several enlarged submandibular and cervical lymph nodes bilaterally without intraoral or cervical abscesses and a collapsed gallbladder with a single gallstone measuring 4×9 mm in size. There was no evidence of choledocholithiasis, or intrahepatic or extrahepatic bile duct or pancreatic duct dilation. Magnetic resonance cholangiopancreatography (MRCP) was likewise negative for biliary tract stenosis or dilation (Figure 2). The transthoracic echocardiograph was negative for valvular vegetations, mitral regurgitation, cardiac aneurysms, or ventricular wall motion asynergy. An abdominal ultrasound detected an 11 mm sized hepatic cyst on the S3 region but otherwise revealed no hepatic masses, surface irregularities, or hepatosplenomegaly. Blood cultures, respiratory multiplex polymerase chain reaction (PCR) assay (BioFire Film array system; BioFire Diagnostics), human immunodeficiency virus (HIV) antigen, hepatitis B and C (HBV and HCV) serology and antigens, treponema pallidum hemagglutination (TPHA), and rapid plasma reagin (RPR) were all unremarkable. Epstein Barr virus (EBV) showed past infection patterns, and CMV-IgM and IgG tested positive (Table 1). Atypical lymphocytes were detected on days 3 and 6 of admission at 4.0% and 3.0%, respectively, with lymphocytic predominance appearing on day 6. Due to diffuse lymphadenopathy, elevated liver enzymes, emergence of atypical lymphocytes, flu-like symptoms, and a positive CMV-IgM, he was suspected to have an acute CMV infection. Antiviral treatment was not started in accordance with the recommended mainstay management for CMV mononucleosis in an immunocompetent host without signs of end-organ damage.
The transient rashA transient macular rash extending from the thighs to the trunk appeared after antibiotic use. The rash resolved shortly after discontinuation of the antibiotics and was considered a drug-induced rash. This picture was taken on the day the antibiotic was discontinued. Unfortunately, no photographs were taken during the active phase of the rash.
A coronal MRCP imageMRCP revealed no abnormalities of the gallbladder or bile ducts, such as dilation, stenosis, stones, or masses, despite elevated liver enzymes.MRCP, magnetic resonance cholangiopancreatography
However, the patient continued to have intermittent fever after admission. A thorough full-body examination was repeated on hospital day 4, revealing an eschar approximately 8×5 mm in size on the left medial malleolus, concealed under his socks (Figure 3). It had been overlooked in previous physical examinations, although it was discovered the patient himself had been aware of it prior to admission and had thought the scab was from “an ill-fitting shoe.” Rickettsial infection was suspected, and serum antibody tests and an eschar tissue biopsy were immediately submitted. However, initiation of antibiotic treatment was withheld due to a gradually improving clinical picture and uncertainty in diagnosis.
The escharAn eschar approximately 0.8x0.5 cm in size was discovered on the left medial malleolus.
On day 7 of admission, an indirect fluorescent antibody (IFA) serology test returned reporting significantly elevated tsutsugamushi IgM levels (Table 2), while the PCR test of the eschar returned negative for Rickettsia japonica. Oral doxycycline was initiated on day 7 for the persistent symptoms and administered for seven days. He was discharged on day 10 and upon his three-week follow-up visit, he showed complete resolution of symptoms and laboratory abnormalities including liver enzyme tests, with no further complications. The repeat CMV paired serology testing was negative, and a follow-up test for tsutsugamushi was deemed unnecessary due to the initial high IgM titer confirming his diagnosis.
Discussion
Scrub typhus is a mite-borne disease endemic to the Asia-Pacific region, caused by Orientia tsutsugamushi of the Rickettsiaceae family. An estimated 1 million people are infected worldwide annually, with the death toll reaching as high as 150,000 per year [1]. Over 400 cases are reported every year in Japan alone, although numbers are suspected to be vastly under-reported with many cases passing undiagnosed [2]. Multiple subtypes with varying genome sequences have been identified, hindering the development of an effective vaccine [3]. Its increasing prevalence, at times attributed to global climate change expanding the field of vector activity [4,5], has prompted the World Health Organization (WHO) to identify it as one of the most neglected causes of tropical fevers in terms of research, diagnosis, and control [6].
Symptoms of scrub typhus appear after an incubation period of 10-12 days and are often flu-like, making it difficult to diagnose. In Japan, fever and rash are the most frequently observed features, present in 95% and 86% of all cases, respectively, although these figures widely vary worldwide [2,7,8]. Other non-specific symptoms include malaise, headache, myalgia, nausea, abdominal pain, and cough [2,9]. If left untreated, scrub typhus can proceed to cause systemic vasculitis with complications including meningoencephalitis, myocarditis, interstitial pneumonia, acute respiratory distress syndrome, renal failure, and disseminated intravascular coagulopathy [1,2,10].
*Tsutsugamushi *infection can be tested directly or indirectly, although the latter method of detecting antibodies via agglutination reactions or immunofluorescence remains the mainstay in Japan, given that PCR testing for *tsutsugamushi *is not covered by national insurance. Serology tests can diagnose scrub typhus if there is a greater than four-fold increase in IgG antibody titers at acute and convalescent stages (at least 14 days apart), or in a single test based on elevated IgM in the appropriate clinical setting [11,12]. Routinely tested antibodies include subtypes Karp, Kato, and Gilliam, although various strains show different patterns of reactivity [3]. In this case, the eschar, highly elevated initial single timepoint IgM, and clinical syndrome that improved with doxycycline administration were interpreted to be sufficient for diagnosis for scrub typhus (although not to the specific subtype), thus a follow-up serology was not performed. Furthermore, symptoms had completely resolved in the two-week minimum interval required between paired tests, making the costly antigen test clinically inconsequential. Direct methods of testing include culture and PCR, which are often only performed in specialized facilities. A PCR of the eschar is more sensitive than blood and can be used for diagnosis even with prior antibiotic use [11,13]. The pathognomonic scab is reported in 85% of all diagnosed cases in Japan and appears at the site of a chigger bite, most frequently on the anterior chest wall, such as the axilla and inguinal regions [14].
Many infectious diseases can be mistaken for scrub typhus due to their similar clinical presentations as febrile illnesses. Especially noteworthy are malaria, dengue, leptospirosis, Salmonella typhi, and other rickettsial diseases due to their overlap in geographical spread in endemicity [15]. Of these infections, *Rickettsia japonica, *which causes Japanese spotted fever, is also endemic in Japan and presents almost identically to scrub typhus with fever, rash, and a localizing eschar at the site of the tick bite, posing a significant diagnostic challenge in the country. Suggested features of *tsutsugamushi *that help distinguish it from Rickettsia japonica include the eschar being slightly larger, the rash being more likely to spare the hands and/or plantar areas, and more prevalent in cooler seasons [16]. Regardless, the two diseases are difficult to differentiate singularly based on clinical presentation, and laboratory tests are usually necessary. Fortunately, the treatment of all rickettsial diseases requires the same antibiotics, making appropriate management possible even if there is a delay in definitive diagnosis.
Once diagnosed, treatment for scrub typhus is relatively simple, with either oral or intravenous antibiotic monotherapy of tetracycline, azithromycin, or chloramphenicol. There have also been studies suggesting combination therapy of intravenous doxycycline and azithromycin to improve outcomes in severe cases [1]. Of note, in recent years, the use of chloramphenicol has declined due to its toxicity profile, including severe side effects such as aplastic anemia. With appropriate treatment, the mortality rate is estimated to be around 1.4%; if untreated, this value increases to 6-70% [1,10,17], emphasizing the gravity of prompt diagnosis and management to reduce fatality [1].
The diagnosis of this case was initially implicated by the failure to detect the eschar and the lack of a characteristic rash. The rise in prevalence of the disease itself and international travelers has increased the risk of its expansion to previously non-endemic regions. The variability of manifestations, as discussed above, poses a particular diagnostic challenge, especially to clinicians unaccustomed to scrub typhus. However, clinical suspicion is critical for initiating appropriate antibiotics in a timely manner, underscoring the importance of raising awareness of the disease and being able to hold a degree of suspicion based on patient history. The eschar can act as a suggestive marker but is small and easily overlooked, such as in this case, accentuating the importance of a detailed full-body physical exam.
The positive CMV-IgM with manifestations resembling infectious mononucleosis with atypical lymphocytes further complicated the diagnosis of this case. There has been a similar case reported where scrub typhus was misdiagnosed as CMV, although CMV-IgM was not elevated in the report [18]. Moreover, there have been past studies detailing false-positive CMV-IgM results in IM-like syndromes; some studies show specificity as low as 72% [19]. In the previous literature, antigen cross-reactivity or interfering substances, such as heterophile antibodies, were listed as potential causes for the false-positive results [19,20].
Conclusions
In conclusion, this case highlights the diverse and non-specific presentation of scrub typhus, an emerging infectious disease with various clinical mimickers. It reiterates the value of performing a detailed physical exam, especially in endemic areas, in guiding accurate diagnosis. Additionally, it draws attention to the possibility of false-positive antibody results due to potential cross-reactivity between *Orientia tsutsugamushi *and other common viruses, emphasizing the need for careful interpretation of serological findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intravenous doxycycline, azithromycin, or both for severe scrub typhus N Engl J Med Varghese GM Dayanand D Gunasekaran K 79280338820233685661510.1056/NEJ Moa 2208449 PMC 7614458 · doi ↗ · pubmed ↗
- 2Scrub typhus and Japanese spotted fever in Japan 2007-2016. IASRIASR 6 2024 INFECTIOUS AGENTS SURVEILLANCEREPORT 109112382007-2016 https://id-info.jihs.go.jp/niid/ja/tsutsugamushi-m/tsutsugamushi-iasrtpc/7324-448t.html
- 3Scrub typhus: the geographic distribution of phenotypic and genotypic variants of Orientia tsutsugamushi Clin Infect Dis Kelly DJ Fuerst PA Ching WM Richards AL 2032304820091922014410.1086/596576 · doi ↗ · pubmed ↗
- 4Climate influences scrub typhus occurrence in Vellore, Tamil Nadu, India: analysis of a 15-year dataset Sci Rep D'Cruz S Sreedevi K Lynette C Gunasekaran K Prakash JA 15321420243823341710.1038/s 41598-023-49333-5PMC 10794692 · doi ↗ · pubmed ↗
- 5Impacts of climate on the incidence of scrub typhus Epidemiol Kim JH Cheong HK 03202009
- 6WHO Recommended Surveillance Standards 4 2025 202421999 https://iris.who.int/handle/10665/65517
- 7Scrub typhus in Japan: epidemiology and clinical features of cases reported in 1998 Am J Trop Med Hyg Ogawa M Hagiwara T Kishimoto T 1621656720021238994110.4269/ajtmh.2002.67.162 · doi ↗ · pubmed ↗
- 8Scrub typhus: overview of demographic variables, clinical profile, and diagnostic issues in the sub-Himalayan region of India and its comparison to other Indian and Asian studies J Family Med Prim Care Pathania M Amisha Amisha Malik P Rathaur VK 11891195820193104127210.4103/jfmpc.jfmpc_124_19PMC 6482722 · doi ↗ · pubmed ↗