Excision of a Solitary Neurofibroma in the Right Masseter Muscle via a High Perimandibular Approach: A Case Report and Review of the Literature
Anna Tomimatsu, Atsushi Kasamatsu, Masumi Igari, Chisato Hashimoto, Shuko Koide, Yutaro Kase, Manabu Iyoda, Dai Nakashima, Katsuhiro Uzawa

TL;DR
A 52-year-old man had a tumor in his masseter muscle successfully removed using a high perimandibular approach, with no complications and no recurrence after 24 months.
Contribution
The paper demonstrates the effectiveness of the high perimandibular approach for excising a solitary neurofibroma in the masseter muscle.
Findings
The high perimandibular approach allowed successful tumor excision without facial nerve damage or trismus.
The patient showed no tumor recurrence over a 24-month follow-up period.
MRI and CT imaging helped in the accurate diagnosis of the intramasseteric mass.
Abstract
We present a case of solitary neurofibroma in the masseter muscle that was excised via the high perimandibular approach (HPMA). A 52-year-old Japanese man complained of an uncomfortable feeling in his right buccal region. On examination, the buccal mucosa appeared normal, and overall, there were no skin disorders on the patient's body. Computed tomography revealed a well-defined 33 × 22-mm mass in the right masseter muscle showing a low density in the center and a slightly higher density at the margin of the mass. Magnetic resonance imaging also showed a hyperintense area on T1-weighted and T2-weighted images in the masseter muscle. An excisional biopsy was scheduled for the diagnosis of the intramasseteric mass. It was performed via the HPMA with the patient under general anesthesia. The final diagnosis was a neurofibroma. The patient recovered after the surgery without postoperative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1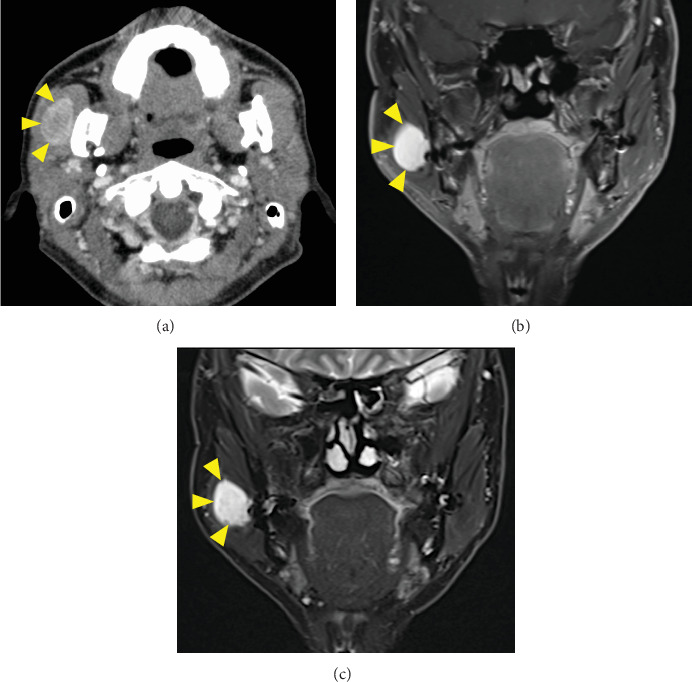 Figure 2
Figure 2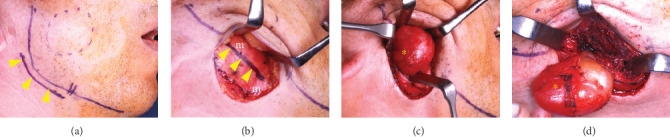 Figure 3
Figure 3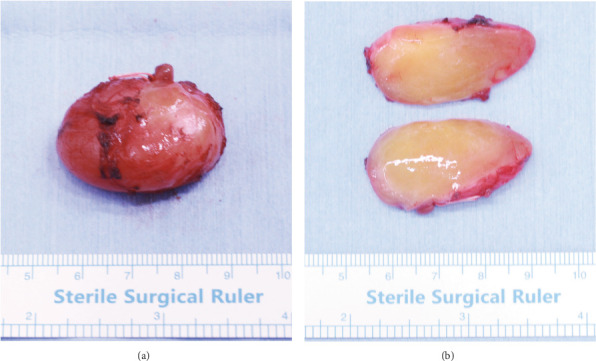 Figure 4
Figure 4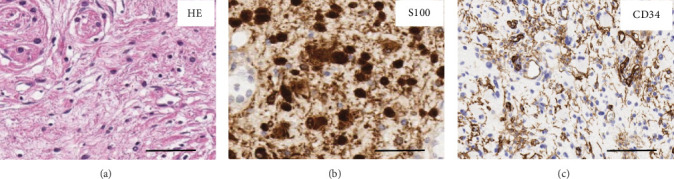 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurofibromatosis and Schwannoma Cases · Meningioma and schwannoma management · Bone Tumor Diagnosis and Treatments
1. Introduction
A neurofibroma is a benign tumor of the peripheral nerve that is composed of a variable mixture of Schwann cells, perineurial-like cells, and fibroblasts. It is known to be a manifestation of the von Recklinghausen disease (neurofibromatosis Type 1; NF1) [1]. The frequency of solitary neurofibromas occurring in the oral cavity is reported to be approximately 6.5% [2]. A common site of neurofibroma in the oral cavity is the tongue [3], whereas its occurrence in the masseter muscle is quite rare.
Intramasseteric tumors have been excised via several approaches, including the submandibular approach, the pre/intra-auricular approach, the retromandibular approach, the high perimandibular approach (HPMA), and the intraoral approach [4, 5]. Each approach presents both advantages and disadvantages for approaching the intramasseteric mass, securing the operative field, and risking injury to the facial nerve [6]. Among the approaches, there have been a few published reports on the use of HPMA for the excision of intramasseteric tumors [7–9]. Here, we present a case of solitary neurofibroma in the masseter muscle that was excised via the HPMA and provide a review of the clinical approaches to intramasseteric tumors.
2. Case Report
A 52-year-old Japanese man was referred to our clinic with the complaint of an uncomfortable feeling in the right buccal region. The medical examination found a painless, slightly swollen area in the right buccal region. There were no palpable lymph nodes bilaterally in the submandibular and neck regions. The patient underwent bilateral orthognathic surgery 30 years prior to this clinic visit and did not have a history of systemic diseases.
Panoramic radiography was negative for abnormal findings. Wires placed during his orthognathic surgery were visible on the mandibular rami (Figure 1). Computed tomography (CT) revealed a well-defined 33 × 22-mm mass in the right masseter muscle showing a low density in the center and a slightly higher density at the margins of the mass (Figure 2a). Magnetic resonance imaging (MRI) also showed a hyperintense mass on T1-weighted (Figure 2b) and T2-weighted images (Figure 2c) in the right masseter muscle. The tumor was isolated, and there were no clinical findings suggesting neurofibromatosis. An excisional biopsy was scheduled for the diagnosis of the intramasseteric mass. The surgery was performed via the HPMA with the patient under general anesthesia.
The HPMA was performed according to the Nakaoka method [6]. Briefly, a 5-cm skin incision was placed 5 mm below and parallel to the edge of the mandibular angle (Figure 3a). Skin and subcutaneous tissue were dissected and undermined 2–3 cm upward over the platysma muscle. The platysma muscle was incised to expose the masseter muscle (Figure 3b), and the intramasseteric tumor was then exposed (Figure 3c,d). Finally, the tumor was completely excised from the masseter muscle. Grossly, the excised specimen was a well-circumscribed oval mass measuring 33 × 22 mm. The surfaces of longitudinal cross-sections of the excised tumor appeared homogeneous, shiny, and light yellow (Figure 4a,b).
On histopathological examination, hematoxylin–eosin (HE) staining showed small spindle cells, fine fibers, Schwann cells, and occasional mast cells (Figure 5a, × 400). Immunohistochemical stainings were positive for S100 (Figure 5b) and CD34 (Figure 5c), indicating that the final diagnosis was neurofibroma. The patient's postoperative course was uneventful without complications, including facial nerve damage and trismus. The patient was satisfied with the esthetic outcome, and recurrence has not occurred over a 24-month period after surgery.
3. Discussion
NF1 is one of the most common autosomal dominant conditions of the nervous system. Its clinical presentation is highly variable and may include multiple neoplasms, as well as cutaneous, vascular, bony, and cognitive manifestations [10]. The clinical manifestations of NF1 include neurofibromas, café-au-lait spots, freckles on the skin, skeletal dysplasia, Lisch nodules, and optic gliomas. Solitary neurofibromas not associated with NF1 are unlikely to recur and show malignant change [11–13], suggesting that complete excision is important for initial treatment.
Oral neurofibromas are most frequently found in the tongue [3] and rarely on the gingiva, mandible, and floor of the mouth. To date, there is a lack of information on neurofibromas in the masseter muscle, and intramuscular hemangiomas make up the majority of intramasseteric tumors [14].
There are two main objectives involved in the surgical procedures used to excise intramasseteric tumors. First, the surgeons must avoid damage to the facial nerve because the trunk and branches of the facial nerve involve the parotid gland and regions adjacent to the masseter muscle. Second, esthetically, it is important to avoid creating conspicuous postoperative scarring.
Intraoral and extraoral surgical approaches have been reported for tumors in the masseter muscle [15–18]. The intraoral approach avoids visible scarring; however, the operative field is limited, and the surgical procedures are complicated. Extraoral approaches more easily secure the surgical field than the intraoral approaches but are likely to injure the branches of the facial nerve and leave an obvious scar on the face [5].
Hamada and Nakaoka reported that the incidence of facial neuropathy after the HPMA is performed for mandibular fractures is 0%–0.9%, which is extremely low compared with other approaches, such as the retromandibular approach and the Risdon approach [5]. The findings suggest that the HPMA is a suitable technique not only for mandibular fractures but also for intramasseteric tumors. The HPMA through the skin provides the easiest access to intramasseteric tumors, with a wide field of view that allows identification of the mandibular and buccal branches of the facial nerve while the skin flap is elevated [8, 19]. An issue of concern with HPMA is that the scar of the skin incision is located below the edge of the mandibular angle. The postoperative scar has been reported to be inconspicuous by several studies because the scar is hidden by the shadow of the mandibular angle [4, 6, 9]. Table 1 lists the five cases of intramuscular tumors located in the masseter muscle that were excised via the HPMA. There were four cases of hemangioma and our case of neurofibroma [7–9]. None of the cases developed postoperative complications, including facial nerve damage, trismus, and motor dysfunction. Therefore, HPMA is an effective and useful alternative approach for intramasseteric tumors.
4. Conclusions
HPMA is a surgical approach for subcondylar fracture of the mandible. Since this approach has been reported to be effective in avoiding damage to the facial nerve and solves esthetic issues, it is also suitable for intramasseteric tumors. The excellent outcomes obtained by the HPMA in our case show that the HPMA may be a useful and convenient approach for excision of intramasseteric neurofibromas.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Komatsu Y. Takeda Y. Kawai T. A Case of Solitary Neurofibroma in the Maxillary Gingiva Journal of Surgical Case Reports 2022202271310.1093/jscr/rjac 22235919699 PMC 9341226 · doi ↗ · pubmed ↗
- 2Broly E. Lefevre B. Zachar D. Hafian H. Solitary Neurofibroma of the Floor of the Mouth: Rare Localization at Lingual Nerve With Intraoral Excision BMC Oral Health 201919119720410.1186/s 12903-019-0888-02-s 2.0-8507161974631464607 PMC 6714308 · doi ↗ · pubmed ↗
- 3Singh Sahota J. Viswanathan A. Nayak R. Hazarika P. Giant Neurofibroma of the Tongue International Journal of Pediatric Otorhinolaryngology 199634153157877068310.1016/0165-5876(95)01233-8 · doi ↗ · pubmed ↗
- 4Lutz J. C. Clavert P. Wolfram-Gabel R. Wilk A. Kahn J. L. Is the High Submandibular Transmasseteric Approach to the Mandibular Condyle Safe for the Inferior Buccal Branch? Surgical and Radiologic Anatomy 2010321096396910.1007/s 00276-010-0663-z 2-s 2.0-7995268174320461515 · doi ↗ · pubmed ↗
- 5Hamada Y. Nakaoka K. Current Strategy of Diagnosis and Treatment for Mandibular Condylar fractures Japanese Journal of Oral & Maxillofacial Surgery 2020661046647210.5794/jjoms.66.466 · doi ↗
- 6Nakaoka K. Yamada H. Horiuchi T. Nakajima T. Nakatani H. Hamada Y. Usefulness of a High Perimandibular Approach for Open Reduction and Internal Fixation of Mandibular Condyle Fractures Journal of Oral and Maxillofacial Surgery 201662341345
- 7Jolly S. S. Rattan V. Rai S. Kaur K. Gupta A. Intramuscular Cavernous Haemangioma of Masseter Muscle – A Case Report of Surgical Excision Journal of Clinical and Diagnostic Research 201594 p. ZD 01–210.7860/JCDR/2015/11305.57702-s 2.0-8492633015126023649 PMC 4437165 · doi ↗ · pubmed ↗
- 8Sukedai M. Manabe R. Kinoshita Y. The High Perimandibular Approach for Excision of an Intramasseter Tumor: A Clinical Report Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology 202133214815110.1016/j.ajoms.2020.09.004 · doi ↗