Consanguinity: The innocent culprit in autism severity
Watfa Al-Mamari, Ahmed B. Idris, Najat Fadlallah, Saquib Jalees, Muna Al-Jabri, Halima Al-Shehhi, Maha Mohammed, Abeer Alsayegh

TL;DR
This study found no significant link between consanguinity and autism severity in a sample of children from Oman.
Contribution
The study provides new evidence on the lack of correlation between consanguinity and ASD severity in a specific population.
Findings
Consanguinity was reported in 59% of the ASD cases studied.
No significant correlation was found between consanguinity or homozygosity and ASD severity levels.
Most ASD cases were classified at severity levels 2 and 3.
Abstract
This study aimed to investigate the relationship between consanguinity and the severity of autism spectrum disorder (ASD), a neurodevelopmental condition influenced by both genetic and environmental factors. This retrospective study, conducted at the Genetic & Developmental Medicine Clinic at Sultan Qaboos University Hospital (SQUH), Muscat, Oman, examined the records of 139 children aged 1.5 to 14 years who were diagnosed with ASD between June 2011 and May 2024. The study analysed the correlation between consanguinity, homozygosity and ASD severity. Of the 139 cases evaluated, 74.1% were male, with an average age of diagnosis of 4.5 ± 2 years. Most ASD cases were classified at severity levels 2 (63.3%) and 3 (35.3%). Consanguinity was reported in 59% of the cases, with a mean homozygosity rate of 4.6%. No significant correlation was found between consanguinity or homozygosity rates…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
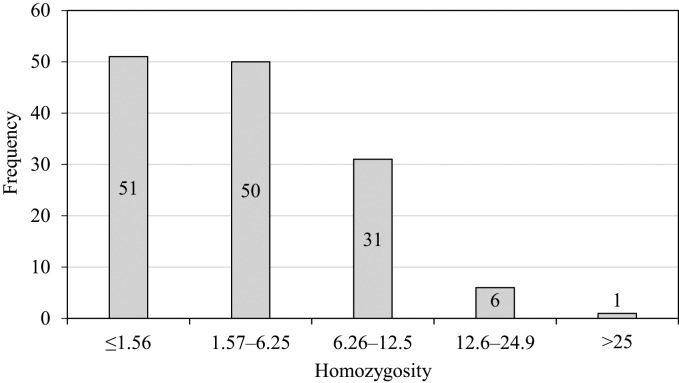 Fig. 1
Fig. 1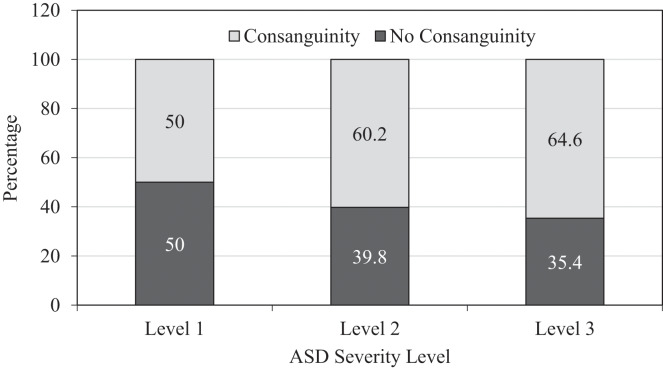 Fig. 2
Fig. 2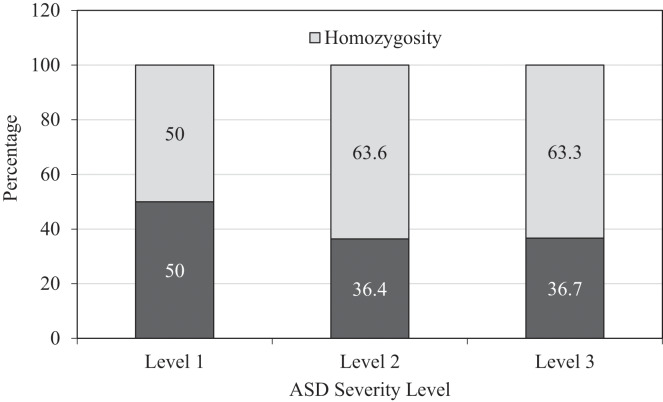 Fig. 3
Fig. 3| Characteristics | n (%) |
|---|---|
| Gender | |
| Male | 103 (74.1) |
| Female | 36 (25.9) |
| Age at diagnosis, mean ± SD | 4.475 ± 2 |
| Age of father at diagnosis, mean ± SD | 38.7 ± 8.2 |
| Age of mother at diagnosis, mean ± SD | 34.4 ± 5.5 |
| Father educational level | |
| Primary education or lower | 15 (10.8) |
| Secondary school | 61 (43.9) |
| University or postgraduate | 61 (43.9) |
| Mother educational level | |
| Primary education or lower | 7 (5) |
| Secondary school | 13 (9.4) |
| University or postgraduate | 113 (81.3) |
| Area of residence | |
| Muscat | 42 (30.2) |
| Ad Dakhiliyah | 23 (16.5) |
| Al Batinah North | 20 (14.4) |
| Al Batinah South | 19 (13.7) |
| Ash Sharqiyah | 20 (14.4) |
| Dhofar | 6 (4.3) |
| Ad Dhahirah | 7 (5.0) |
| Musandam | 2 (1.4) |
| Prematurity | |
| Full term | 124 (89.2) |
| Preterm | 15 (10.7) |
| Mode of delivery | |
| SVD | 103 (74.1) |
| C/S | 32 (23.0) |
| Consanguinity | |
| Yes | 82 (59) |
| No | 51 (36.7) |
| Homozygosity | |
| ≤1.56 | 51 (36.7) |
| >1.56 | 88 (63.3) |
| Seizures | 12 (8.6) |
| Sleeping problems | 33 (23.7) |
| Feeding problems | 42 (30.2) |
| Others | 17 (12.2) |
| Homozygosity | ||||
|---|---|---|---|---|
| ≤1.56 (n = 51) | >1.56 (n = 88) | Total | P-value | |
| Gender | 0.472 | |||
| Male | 36 (35) | 67 (65.0) | 103 (74.1) | |
| Female | 15 (41.7) | 21 (58.3) | 36 (25.9) | |
| Age at diagnosis, mean ± SD | 4.14 ± 2.03 | 4.67 ± 2.02 | 0.138 | |
| Father educational level | 0.475 | |||
| Primary education or lower | 7 (46.7) | 8 (53.3) | 15 (10.8) | |
| Secondary school | 24 (39.3) | 37(60.7%) | 61 (43.9) | |
| University or postgraduate | 19 (31.1) | 42(68.9%) | 61 (43.9) | |
| Mother educational level | 0.465* | |||
| Primary education or lower | 1 (14.3) | 6(85.7%) | 7 (5.0) | |
| Secondary school level | 5 (38.5) | 8(61.5%) | 13 (9.3) | |
| University or postgraduate level | 42 (37.2) | 71(62.8%) | 113 (81.3) | |
| Family history of developmental disorders in siblings (including ASD) | 0.413 | |||
| Yes | 9 (40.9) | 13 (59.1) | 22 (15.8) | |
| No | 42 (35.9) | 75 (64.1) | 117 (84.2) | |
| Consanguinity | <0.001 | |||
| Yes | 6 (7.3) | 76 (92.7) | 82 (59.0) | |
| No | 41 (80.4) | 10 (19.6) | 51 (36.7) | |
| Prematurity | 0.507 | |||
| Full term | 46 (37.1) | 78 (62.9) | 124 (89.2) | |
| Preterm | 5 (33.3) | 10 (66.7) | 15 (10.8) | |
| Mode of delivery | 0.525 | |||
| SVD | 37 (35.9) | 66 (64.1) | 103 (74.1) | |
| C/S | 11 (34.4) | 21 (65.6) | 32 (23.0) | |
| ASD severity level | 0.925* | |||
| Level 1 | 1 (50.0) | 1 (50.0) | 2 (1.4) | |
| Level 2 | 32 (36.4) | 56 (63.6) | 88 (63.3) | |
| Level 3 | 18 (36.7) | 31 (63.3) | 49 (35.2) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemoglobinopathies and Related Disorders
1. Introduction
Autism spectrum disorder (ASD) is a complex neurodevelopmental condition characterised by challenges in social interaction, communication and the presence of repetitive behaviours.^1^ Global prevalence estimates for ASD exhibit substantial variability, with a median rate of 100 cases per 10,000 individuals (1%) and a range from 1.09 to 436 per 10,000.^2^ In Oman, the estimated prevalence of ASD is 20.35 per 10,000 children, with a 95% confidence interval of 19.39 to 21.32.^3^ The aetiology of ASD is multifactorial, including both genetic and environmental components. Recent developments in genetic research have underscored the importance of genetic contributions to ASD. A multitude of studies have identified distinct genetic variants and polymorphisms linked to ASD.^456^
Consanguinity – the practice of marrying within a close family – is common in several regions, including the Middle East, South Asia and North Africa.^7^ Approximately 20% of the global population prefers consanguineous marriages due to their positive social implications. Consanguinity rates can vary among different groups due to factors such as geography, ethnicity, culture and religion.^8^ In Oman, it is estimated that 52% of marriages are consanguineous, involving couples who are second- or third-degree relatives.^9^
Consanguineous marriages increase homozygosity within the population, as the offspring of such unions are more likely to inherit identical alleles from both parents. Elevated homozygosity can result in a higher incidence of autosomal recessive disorders and may influence the expression and severity of complex traits.^1011^ On the other hand, the association between consanguinity and ASD as a risk factor is somewhat obscured in the context of a polygenic multifactorial disorder such as ASD, with conflicting evidence present in the current literature.^1213^
Runs of homozygosity, which serves as an indicator of genetic diversity within an individual's genome, are particularly relevant in consanguineous populations. The percentage of homozygosity (FROH) can be inferred from single nucleotide polymorphism (SNP) microarray data and used to estimate the degree of parental consanguinity. This estimation is typically conducted by aggregating the total length of autosomal regions of homozygosity (ROH) that exceed a specified size threshold and dividing this sum by the total number of autosomal base pairs represented on the microarray platform.^141516^ Higher homozygosity rates can increase the likelihood of inheriting recessive genetic variants.^17^ The association between consanguinity, homozygosity and intellectual disability has been investigated, revealing that the level of homozygosity seems to modulate the degree of cognitive impairment regardless of the underlying cause of intellectual disability.^18^ However, the impact of homozygosity on the severity of ASD remains to be fully understood.
Therefore, this study aims to investigate the correlation between homozygosity rates, which serve as a marker of consanguinity, and the severity of ASD. This study underscores the significance of considering genetic diversity in the context of ASD, particularly among consanguineous populations.
2. Methods
The study was conducted at the Genetic & Developmental Medicine Clinic at Sultan Qaboos University Hospital (SQUH), Muscat, Oman. A retrospective analysis was performed for computerised records of patients diagnosed with ASD between June 2011 and May 2024. Children aged 14 years or younger who had a homozygosity rate determined by SNP and comparative genomic hybridization (CGH) microarray testing and who presented a complete clinical phenotype as assessed by developmental paediatricians and medical geneticists were eligible for inclusion in this study. A total of 710 children, aged 1.5 to 14, underwent microarray CGH testing during the study period. Among these, 139 cases had comprehensive clinical information recorded in the electronic health record, including the homozygosity rate and degree of severity. To eliminate potential interference from substantial copy-number variations (CNVs) that could compromise the accuracy of ROH measurements (specifically, genomic deletions that may appear as segments of homozygosity but actually reflect hemizygosity), cases with CNVs were excluded from the dataset.
A multidisciplinary team led by a senior developmental paediatrician employed the Autism Diagnostic Interview-Revised and the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) to confirm the diagnosis of ASD in the cases. Abiding by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria, ASD specifiers require clinicians to exercise their clinical judgement to delineate among three classifications: level 1 (‘requiring support’), level 2 (‘requiring substantial support’) and level 3 (‘requiring very substantial support’). Consequently, the severity level was determined by diagnosticians trained in developmental paediatrics at the time of diagnosis.^119^
The consanguineous couple's data were incurred from electronic records, where the consanguineous definition involved ‘first cousin, father's side’, including the father's brother's son (patrilateral parallel cousin) and the father's sister's son (cross-cousin Type I). Similarly, the ‘first cousin, mother's side’ included the mother's brother's son (matrilateral parallel cousin), the mother's sister's son (cross-cousin Type II) and second-degree cousins. Non-consanguineous marriages consisted of non-relatives or distant relatives with a degree of relatedness less than that of second cousins.^9^ The homozygosity rates were classified as follows: offspring of second cousins are expected to have 1.56% (1/64) of their genome homozygous; offspring of first cousins are expected to have 6.25% (1/16); offspring of double first cousins are expected to have 12.5% (1/8); and offspring of incestuous unions are expected to have 25% (1/4).^17^
The DNA samples from patients were collected to facilitate etiological diagnosis as part of the clinical protocol. These samples were sent to SISTEMAS GENóMICOS S.L., a laboratory that adheres to the American College of Medical Genetics and Genomics (ACMG) guidelines for interpreting deletions, duplications, homozygosity and variants.^2021^
A set of clinical phenotypic characteristics, along with the parent's and child's demographic characteristics, were evaluated. Data analysis employed both descriptive and inferential statistical techniques. The analysis was conducted using the Statistical Package for the Social Sciences (SPSS), Version 27 (IBM Corp., Armonk, New York, USA). The characteristics of children with ASD were described using frequency distribution. The correlation between categorical factors was assessed using a chi-square test, while the significance of the association between a categorical variable and a numerical variable was examined using one-way analysis of variance (ANOVA). Fisher's exact test was conducted when a cell's expected value was less than five. A P value of <0.05 was considered statistically significant. Furthermore, the parental report of consanguinity was correlated with the rate of homozygosity and tested against the severity level of ASD.
3. Results
The study included 139 cases, with males constituting the majority at 74.1%. The average age at diagnosis was 4.5 ± 2 years. Around 50% of the cases originated from Muscat and Al Batinah. The average age of fathers was 38.7 ± 8.2 years, while the mean age of mothers was 34.4 ± 5.5 years. Most parents (60%) had completed secondary school education [Table 1]. Approximately 15.8% of the subjects had a family history of ASD or developmental disorders in their siblings. Approximately 10.8% of subjects were preterm, and 23% were delivered via caesarean section. Regarding ASD severity, 1.4% had level 1 ASD, 63.3% had level 2 ASD and 35.3% had level 3 ASD. The reported rate of consanguinity was 59%, and the mean homozygosity rate was 4.6 ± 4.8.
The distribution of homozygosity rates was as follows: 51 subjects had a homozygosity rate of ≤1.56%, 50 were children with a homozygosity rate between 1.57% and 6.25%, 31 were children with a homozygosity rate between 6.26% and 12.5%, six were children with a homozygosity rate between 12.6% and 24.9% and one subject had a homozygosity rate of 30%. This distribution is illustrated in Fig. 1.
Distribution of homozygosity rate among children with autism spectrum disorder.
A significant relationship was observed between homozygosity and consanguinity. The mean homozygosity rate among subjects from consanguineous marriages was 6.9%, while the mean homozygosity rate among subjects from non-consanguineous marriages was 1.25% [Table 2].
A comparative analysis of consanguinity status and ASD severity revealed no statistically significant association [Fig. 2]. Similarly, the investigation into the relationship between homozygosity and ASD severity indicated no significant correlation [Fig. 3].
Comparison between consanguinity and autism spectrusm disorder severity level (P = 0.836).
Comparison between homozygosity rate and autism spectrum disorder severity level (P = 0.925).
4. Discussion
This cohort comprised 74% males, highlighting the gender imbalance in the distribution of autism.^22^ Additionally, the consanguinity rate was 59%, which is characteristic of the Middle Eastern Arab population.^8^ The cases were widely distributed across the country, with most parents residing in the capital city. Additionally, the parents’ educational attainment was predominantly at the secondary school level.
The distribution of severity levels within this cohort reveals a significant skew towards more severe cases of ASD. Specifically, 63.3% of the cases were classified as level 2 ASD, with only one case classified as level 1. This distribution contrasts with findings from the Autism Treatment Network (ATN) sites in the United States, where approximately 30% of cases were classified as level 1.^23^ This discrepancy may be attributed to several factors, including limited community awareness of ASD and inadequately distributed diagnostic services in Oman. The constrained availability and accessibility of these services likely contribute to the prevalence of more severe ASD phenotypes in the Omani population.^32425^
The study demonstrated a statistically significant disparity between parental reports of consanguinity and observed homozygosity rates exceeding 1.56. This finding indicates potential discrepancies in estimating the theoretical inbreeding coefficient, which may stem from parental misconceptions about their relatedness or inaccuracies in calculating the homozygosity rate. Although the percentage of homozygosity is commonly employed to estimate consanguinity, and physicians managing families with known consanguinity may utilise SNP microarrays, emerging research indicates that data mining within ROH can substantially enhance the diagnosis of suspected autosomal recessive conditions.^26^ Notably, the percentage of homozygosity may inaccurately represent the theoretical inbreeding coefficient due to various confounding factors. These factors include deviations from theoretical expectations, challenges in accounting for multiple generations of consanguinity, random crossover events during meiosis, variability in ROH size inclusion criteria and differences in microarray platform coverage.^16^ Consequently, a nuanced approach that integrates the history of consanguinity with other genetic assessment tools is imperative for achieving accurate diagnostic outcomes.
The association between the severity of ASD and consanguinity, as well as the rate of homozygosity, was not statistically significant in this cohort. This suggests that neither consanguinity nor the rate of homozygosity influences ASD severity. These findings align with those of Gamsiz et al., who observed a statistical relationship between runs of homozygosity and measures of intellectual functioning but not with measures of autism symptoms or severity.^27^ Conversely, recent data from Saudi Arabia reported that children of consanguineous parents had higher Autism Treatment Evaluation Checklist (ATEC) scores, indicating more severe symptoms; however, this finding was not statistically significant across all analyses.^28^ Several scholars have criticised the reliance on parental reports for determining the degree of a child's disability, arguing that parents may misclassify severity compared to clinical diagnoses.^293031^ Furthermore, it is crucial to acknowledge that the ATEC was specifically designed to assess treatment efficacy rather than to serve as a diagnostic tool. Consequently, the ATEC can only provide an approximation of ASD severity through total scores, which are further differentiated by age.^3233^
In India, Mamidala et al. found a significant association between consanguineous marriages and an increased ASD risk, highlighting the genetic implications of such unions.^34^ Similarly, Bitar et al. reported from Lebanon that children born to consanguineous parents exhibited a higher prevalence of ASD, suggesting that consanguinity may contribute to the genetic burden of autism-related mutations.^35^ In contrast, studies conducted on the Arabian Peninsula present a different perspective. Data from the Omani population and Qatar show no significant increase in ASD prevalence among consanguineous populations.^312363738^ These findings imply that while consanguinity may be a risk factor in specific populations, its impact on ASD prevalence is not universally observed. The discrepancies in the data may indicate that other genetic, environmental or sociocultural factors could play a more significant role in these regions.
The limitations of this study stem from its retrospective design and its status as a single-centre study with a relatively small sample size. The low prevalence of ASD in the country – compared to global estimates – may affect the variability of cases and the generalisability of the results to other regions of the world. The aggregation of consanguinity into a single category rather than stratifying it into levels may introduce bias. The predominance of cases at levels 2 and 3 of ASD severity within the dataset may further skew the findings towards a more severe ASD population, thereby limiting the generalisability of the results. This bias also hindered comprehensive intellectual abilities testing. Additionally, outsourcing genetic testing posed another limitation, as it restricted the ability to analyse the entire ROH due to incomplete data availability.
5. Conclusion
This study did not support the hypothesis that consanguinity increases the severity of ASD. Further research is necessary to understand the genetic mechanisms involved and to determine the extent to which consanguinity influences both the risk and severity of ASD.
Funding
No funding was received for this study.
Ethics Statement
The study received ethical approval from the Medical Research and Ethics Committee at Sultan Qaboos University in Oman. The report adheres to the ethical guidelines set out in the World Medical Association's Declaration of Helsinki (1964–2008), which pertains to the privacy and confidentiality of participants as well as the handling of data.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contributions
The authors confirm their contributions to the paper as follows. Study conception and design: Ahmed B. Idris and Watfa Al-Mamari. Data collection and cleansing: Najat Fadlallah, Muna Aljabri and Ahmed B. Idris. Data analysis: Maha Mohammed and Ahmed B. Idris. Interpretation of results: Ahmed B. Idris, Maha Mohammed, Abeer Al-Saegh and Watfa Al-Mamari. Drafting the initial manuscript: Ahmed B. Idris and Saquib Jalees. All authors reviewed the results and approved the final version of the manuscript.
Acknowledgements
The author expresses gratitude to all personnel involved in this study, specifically Dr. Siamak Saber, for his assistance with the manuscript review.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5®). Washington: American Psychiatric Association; 2013.
- 2Zeidan J Fombonne E Scorah J Ibrahim A Durkin MS Saxena S. Global prevalence of autism: A systematic review update. Autism Res 2022; 15:778–90. https://doi.org/10.1002/aur.2696.10.1002/aur.269635238171 PMC 9310578 · doi ↗ · pubmed ↗
- 3Al-Mamri W Idris AB Dakak S Al-Shekaili M Al-Harthi Z Alnaamani AM. Revisiting the prevalence of autism spectrum disorder among omani children a multicentre study. Sultan Qaboos Univ Med J 2019; 19:e 305–9.10.18295/squmj.2019.19.04.00531897313 PMC 6930034 · doi ↗ · pubmed ↗
- 4Du X Gao X Liu X Shen L Wang K Fan Y. Genetic diagnostic evaluation of trio-based whole exome sequencing among children with diagnosed or suspected autism spectrum disorder. Front Genet [Internet] 2018; 9:594. https://doi.org/10.3389/fgene.2018.00594.10.3389/fgene.2018.0059430555518 PMC 6284054 · doi ↗ · pubmed ↗
- 5Huguet G Ey E Bourgeron T. The genetic landscapes of autism spectrum disorders. Annu Rev Genomics Hum Genet 2013; 14:191–213.10.1146/annurev-genom-091212-15343123875794 · doi ↗ · pubmed ↗
- 6Vorstman JAS Parr JR Moreno-De-Luca D Anney RJL Nurnberger JI Hallmayer JF. Autism genetics: Opportunities and challenges for clinical translation. Nat Rev Genet 2017; 18:362–76. https://doi.org/10.1038/nrg.2017.4.10.1038/nrg.2017.428260791 · doi ↗ · pubmed ↗
- 7Bittles AH. Consanguinity and its relevance to clinical genetics. Clin Genet 2001; 60:89–98. https://doi.org/10.1034/j.1399-0004.2001.600201.x.10.1034/j.1399-0004.2001.600201.x 11553039 · doi ↗ · pubmed ↗
- 8Tadmouri GO Nair P Obeid T Al Ali MT Al Khaja N Hamamy HA. Consanguinity and reproductive health among Arabs. Reprod Health 2009; 6:17. https://doi.org/10.1186/1742-4755-6-17.10.1186/1742-4755-6-1719811666 PMC 2765422 · doi ↗ · pubmed ↗