Empagliflozin Use in Cardiac Transplant Patients: Real-world experience from Saudi Arabia
Muhammad I. Butt, Roaa M. H. Albalwi, Norah Alnassar, Reem Alghamdi

TL;DR
This study examines the safety and effectiveness of empagliflozin in cardiac transplant patients with diabetes in Saudi Arabia, finding it beneficial without major side effects.
Contribution
Provides real-world evidence on empagliflozin safety and efficacy in cardiac transplant recipients, a previously understudied population.
Findings
Empagliflozin improved HbA1C levels, body weight, and serum creatinine stability in cardiac transplant patients.
No increased risk of genitourinary infections, hypoglycaemia, or diabetic ketoacidosis was observed.
The study suggests empagliflozin is safe for cardiac transplant recipients with diabetes.
Abstract
Sodium-glucose transport protein 2 (SGLT2) inhibitors are used in the treatment of patients with type 2 diabetes. Besides their beneficial metabolic effects, such as lowering glycated haemoglobin, body weight and blood pressure, these agents have shown favourable and protective effects on both the heart and kidneys. Notably, these cardio-renal benefits are even seen in individuals without diabetes. However, there is limited evidence regarding the safety and efficacy of SGLT2 inhibitors in cardiac transplant recipients. This study aimed to assess the safety and efficacy of empagliflozin in cardiac transplant recipients with diabetes. This retrospective study was conducted at the King Faisal Specialist Hospital & Research Centre in Riyadh, Saudi Arabia, from June 2003 to May 2024. Patients from the cardiac transplant recipient register who were taking empagliflozin or a combination of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
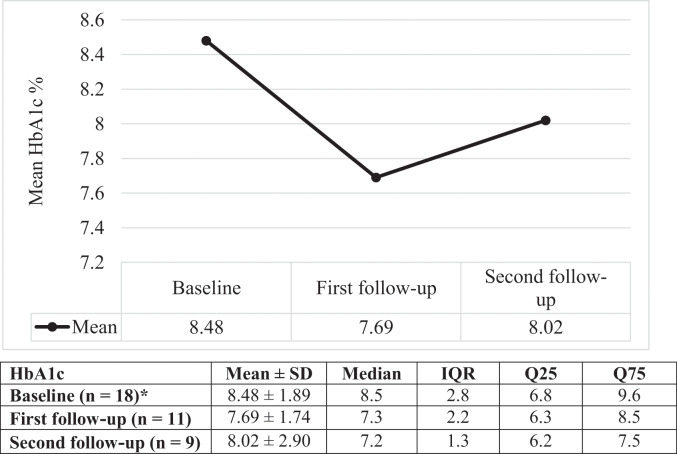 Fig. 1
Fig. 1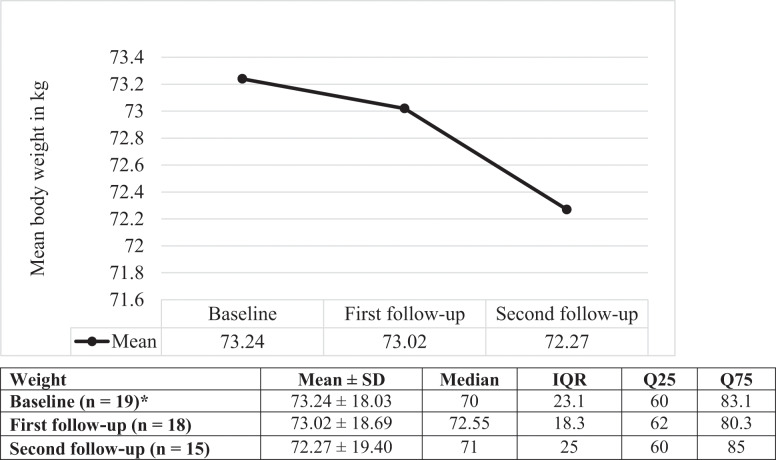 Fig. 2
Fig. 2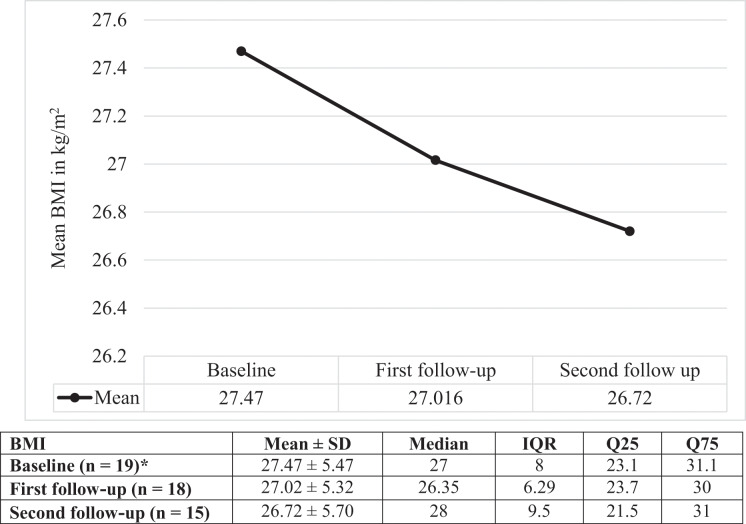 Fig. 3
Fig. 3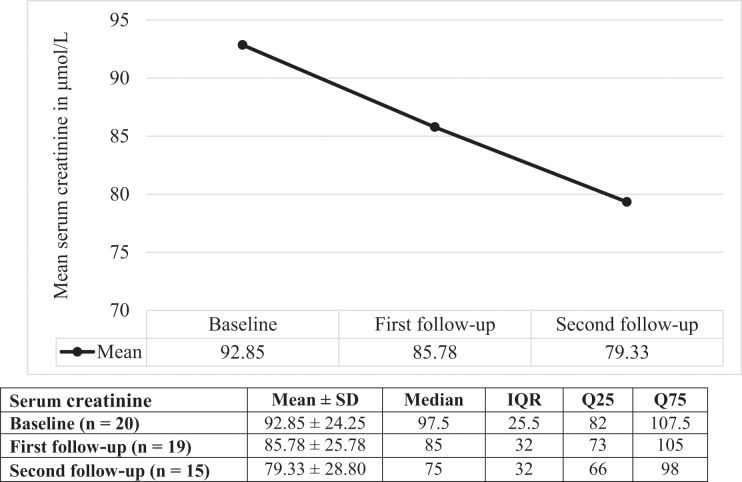 Fig. 4
Fig. 4| Characteristic | n (%) |
|---|---|
| Mean age ± SD in years | 49.6 ± 16.42 |
| Gender | |
| Male | 15 (75.0) |
| Female | 5 (25.0) |
| Mean weight ± SD in kg (n = 19)* | 73.24 ± 18.03 |
| BMI in kg/m2 (n = 19)* | |
| <20 | 1 (5.3) |
| 20–24.9 | 6 (31.6) |
| 25–29.9 | 4 (21.1) |
| 30–34.9 | 7 (36.8) |
| 35–39.9 | 1 (5.3) |
| Mean blood pressure ± SD in mmHg (n = 19)* | |
| Systolic | 122.15 ± 14.54 |
| Diastolic | 74.57 ± 11.96 |
| Duration of diabetes in years | |
| <5 | 3 (15.0) |
| 5–10 | 2 (10.0) |
| >10 | 7 (35.0) |
| Unknown | 8 (40.0) |
| Haemoglobin A1C in % | |
| <6 | 2 (10.0) |
| 6–6.9 | 3 (15.0) |
| 7–7.9 | 2 (10.0) |
| 8–8.9 | 5 (25.0) |
| 9–9.9 | 2 (10.0) |
| >10 | 4 (20.0) |
| Not done | 2 (10.0) |
| Mean haemoglobin A1C ± SD in % (n = 18)* | 8.48 ± 1.89 |
| Mean serum creatinine level ± SD in μmol/L | 92.85 ± 24.25 |
| GFR | |
| <45 | 0 (0.0) |
| 45–59 | 7 (35.0) |
| >60 | 13 (65.0) |
| Reason for cardiac transplant (n = 20)† | |
| Cardiomyopathy | 19 (95.0) |
| Coronary heart disease | 8 (40.0) |
| End-stage heart failure | 3 (15.0) |
| Recurrent arrhythmias not controlled with all other treatment options | 1 (5.0) |
| Cardiovascular disease past medical history n = 20‡ | |
| Coronary disease | 12 (60.0) |
| Cerebrovascular disease | 1 (5.0) |
| Heart failure | 11 (55.0) |
| History in the last 12 months prior to prescription | |
| Genital infection | 0 (0.0) |
| Urinary tract infections | 0 (0.0) |
| Hospitalisation for hypoglycaemia | 0 (0.0) |
| Hospitalisation for heart failure | 7 (35.0) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Renal Transplantation Outcomes and Treatments · Adenosine and Purinergic Signaling
1. Introduction
Empagliflozin is an oral antidiabetic agent that belongs to the class of sodium-glucose transport protein 2 (SGLT2) inhibitors. It acts on the SGLT2 receptors located in the proximal tubules of the nephrons, inhibiting the reabsorption of filtered glucose.^1^ This unique, insulin-independent mechanism of action results in glycosuria and a net loss of sodium and water, thereby helping to regulate glucose homeostasis.
For many decades, the focus of diabetes care has been to achieve reasonable glycaemic control. However, the publication of the EMPA-REG trial in 2015 significantly altered this landscape.^2^ This trial demonstrated that, besides improving glycaemic control, empagliflozin reduced the risk of major adverse cardiovascular events by 13%. Moreover, patients who used empagliflozin experienced a decreased risk of cardiovascular mortality. This landmark trial shifted clinicians’ focus from a glucocentric approach to prioritising cardiovascular risk reduction in patients with diabetes. Additional evidence from the EMPEROR-Reduced and EMPEROR-Preserved randomised controlled trials further confirmed that empagliflozin effectively reduced the risk of cardiovascular mortality and heart failure-related hospital admissions regardless of the presence or absence of diabetes.^34^
A meta-analysis of 6 randomised controlled trials involving over 46,000 patients with type 2 diabetes treated with 4 different types of SGLT2 inhibitors demonstrates that SGLT2 inhibitors, as a class, have favourable effects on cardiovascular risk reduction.^5^ Likewise, another meta-analysis of 8 randomised controlled trials, which included over 60,000 patients taking a different drug class, glucagon-like peptide-1, has demonstrated similar results in improving glycaemic control and minimising cardiovascular risks.^6^
Rivinius et al. report that nearly one-third of cardiac transplant recipients have pre-existing type 2 diabetes, which increases their risk of graft failure and mortality within 5 years.^7^ Similarly, approximately 25% of cardiac transplant recipients are at heightened risk of developing post-transplant diabetes mellitus (PTDM).^8^ The development of PTDM significantly increases morbidity and mortality rates among these transplant patients.^8^ While extensive evidence supports the use of empagliflozin in high-risk diabetes patients with enhanced cardiovascular risk, there is a paucity of evidence regarding its use in cardiac transplant recipients who are taking immunosuppressive drugs, which heightens the risk of infections as well as cardiac and renal impairment.^5^
This study aimed to investigate the safety and efficacy of empagliflozin in cardiac transplant recipients with pre-existing type 2 diabetes. Additionally, it seeks to evaluate efficacy parameters, including haemoglobin A1C (HbA1c), weight, body mass index (BMI) and serum creatinine levels, as well as safety parameters, such as genitourinary infection risk.
2. Methods
This retrospective study identified patients from the cardiac transplant registry at the King Faisal Specialist Hospital & Research Centre in Riyadh, Saudi Arabia, June 2003 to May 2024 using the keywords ‘diabetes’, ‘empagliflozin’, ‘Synjardy’ and ‘Jardiance’. The study included all patients who initiated empagliflozin post-transplant for the treatment of pre-existing type 2 diabetes. Electronic medical records of the study population were reviewed. The study also included patients who used the study drug for at least 6 months and had baseline and follow-up clinical data from 2 clinic visits. The first follow-up data were recorded between the second and fourth months, and the second follow-up data were collected between the fifth and seventh months from baseline. Safety parameters were assessed, including episodes of genitourinary infections and hypoglycaemia. Efficacy parameters were also evaluated, including changes in HbA1c, weight, serum creatinine and estimated glomerular filtration rate (eGFR).
Baseline characteristics were summarised using continuous variables and presented as means and standard deviations. Frequencies, percentages and graphs were used to present summary data for both continuous and categorical variables. Data were collected using the password-protected REDCap software (Vanderbilt University, Nashville, USA).
3. Results
A total of 20 patients were included. Of these, 12 patients received an empagliflozin and metformin combination (Synjardy) and continued this regimen; 5 patients took empagliflozin at a dosage of 25 mg daily; 3 patients took empagliflozin at a dosage of 10 mg daily. The patients had a mean age of 49.6 ± 16.4 years and 75.0% were male. The mean body weight was 73.24 ± 18.03 kg and more than 60% of the patients fell into the overweight to obese category. The mean HbA1c level was 8.48 ± 1.89%. The predominant reason for requiring cardiac transplantation was cardiomyopathy (95.0%), followed by coronary artery disease (40.0%). The patients had a significant history of cardiovascular disease, with 60.0% having coronary artery disease, 55.0% having heart failure and 35.0% having a history of hospitalisation due to heart failure in the preceding 12 months [Table 1]. Most patients were prescribed more than 1 anti-rejection medication. All patients were taking steroids (2 patients were on cyclosporine, 17 patients were on tacrolimus and 18 patients were on mycophenolate).
HbA1c improved from a mean baseline of 8.48 ± 1.89% to 8.02 ± 2.90% at the second follow-up [Fig. 1]. Body weight decreased from 73.24 ± 18.03 kg to 72.27 ± 19.40 kg [Fig. 2]. BMI improved from 27.47 kg/m^2^ to 26.72 kg/m^2^ [Fig. 3]. The eGFR remained stable, increasing from a baseline of 62.3 ± 6.82 mL/min/1.73m^2^ to 64.33 ± 5.74 mL/min/1.73m^2^. Serum creatinine levels decreased from a baseline of 92.85 ± 24.25 μmol/L to 79.33 ± 28.80 μmol/L [Fig. 4]. All patients underwent a post-transplant echocardiogram within 3 months, and the ejection fraction (EF) was >50%. Additionally, 18 patients had echocardiogram results available at 6 months; EF was >50% in 12 patients, between 40–49% in 2 patients and <40% in 4 patients. Only 1 patient experienced transplant rejection between 3- and 6-months post-transplant. Additionally, the patient developed a genitourinary infection that required oral antibiotic treatment. No patients experienced hypoglycaemic episodes or diabetic ketoacidosis (DKA) that necessitated hospitalisation. However, 4 patients were treated in the hospital for renal impairment during the follow-up period; empagliflozin was temporarily withheld and subsequently resumed upon their discharge from the hospital.
*Change in glycated haemoglobin in patients from the current study HbA1c = glycated haemoglobin; SD = standard deviation; IQR = interquartile range. Missing information in 2 patients.
*Change in body weight in patients from the current study.SD = standard deviation; IQR = interquartile range. Missing information in 1 patient.
*Change in the body mass index in patients from the current study.BMI = body mass index; SD = standard deviation; IQR = interquartile range. Missing information in 1 patient.
Change in serum creatinine in patients from the current study. SD = standard deviation; IQR = interquartile range.
4. Discussion
Patients taking SGLT2 inhibitors are at an increased risk of genitourinary infections.^2^ This risk is further enhanced when patients are also taking immunosuppressive drugs post-cardiac transplant. In this study, only 1 patient experienced a genitourinary infection, which was amicably treated with oral antibiotics. The patient did not require hospitalisation or withdrawal of empagliflozin.
DKA is a rare occurrence in patients with type 2 diabetes. However, there have been reports of euglycemic ketoacidosis in individuals taking SGLT2 inhibitors.^9^ This risk can be mitigated by temporarily omitting the use of these medications during acute illnesses and perioperative periods. In this study, no patients developed DKA, which supports the safe use of empagliflozin in cardiac transplant recipients.
Hypoglycaemia is an undesirable but well-recognised side effect of any diabetes management regimen. It is often seen in patients taking either insulin or medications that stimulate insulin secretion. Empagliflozin operates through an insulin-independent mechanism by promoting glucose excretion in the urine; therefore, it does not increase the risk of hypoglycaemia, particularly when not used in conjunction with either insulin or insulin secretagogues.^1^ None of the patients reported in the current study experiencing hypoglycaemia that required hospitalisation or third-party assistance.
Dehydration and renal impairment resulted in the hospitalisation of 3 patients. During the acute illness and treatment, empagliflozin was temporarily discontinued and subsequently restarted once the patients recovered prior to discharge from the hospital. Treatment with SGLT2 inhibitors can lead to an increase in urine volume of approximately 300 mL/day.^1^ This fluid loss is usually inconsequential for most patients with diabetes. However, in patients with significant comorbidities, such as heart transplant recipients, the concurrent use of diuretics can elevate the risk of dehydration. This risk is further exacerbated by the high temperatures recorded in Saudi Arabia, which can reach up to 50°C in the summer, contributing to dehydration. Clinicians should exercise caution when prescribing SGLT2 inhibitors to patients with comorbidities, particularly those who are also using diuretics.
This study's results are consistent with those observed by Cehic et al. in their cohort of 22 patients regarding safety and efficacy.^10^ While these are small observational studies, definitive evidence is expected from the ongoing randomised controlled trial investigating the use of empagliflozin in cardiac transplant recipients.^11^
This study draws its strength from the availability of unique data on cardiac transplant recipients with type 2 diabetes who are using empagliflozin, a population that is otherwise under-studied or under-published. Diabetes is a prevalent condition, and empagliflozin is a well-established oral antidiabetic agent. Given these parameters, although this study sample size was small, it should still be considered significant. Furthermore, this study focused on a niche population of heart transplant recipients, which renders the sample size reasonable.
However, this study has several weaknesses, including its retrospective design. The results are derived only from the Saudi population in Saudi Arabia and may not be applicable to other geographical regions or ethnic groups. Furthermore, most patients in this study did not have any recorded results for proteinuria. Proteinuria is common among transplant recipients and is multifactorial, often resulting from the use of immunosuppressive drugs such as cyclosporine, tacrolimus, sirolimus and everolimus as well as the presence of diabetes, hypertension and episodes of transplant rejection. Regular monitoring of urine protein is essential. The use of therapies such as angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers can help reduce proteinuria. Additionally, effective control of blood pressure and diabetes will be invaluable. Future studies should include the measurement of proteinuria.
5. Conclusion
Although larger studies are needed to examine the use of empagliflozin in cardiac transplant patients, this small study provides assurance that empagliflozin is safe for use in cardiac transplant recipients.
Funding
No funding was received for this study.
Ethics Statement
Approval for conducting the study was obtained from the institutional research committee at King Faisal Specialist Hospital & Research Centre (2245141). The study adhered to the CARE checklist for case series throughout the study period and all data were anonymised in accordance with institutional confidentiality guidelines.
Conflict of Interest
The authors declare that there are no conflicts of interest.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contributions
MIB conceptualised and designed the study. RMHA, NA and RA collected the data, while MIB, NA and RA analysed it. NA and RA prepared the tables and figures. MIB drafted the manuscript. All authors critically revised the manuscript and approved the final version.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fonseca-Correa JI Correa-Rotter R. Sodium-glucose cotransporter 2 inhibitors mechanisms of action: A review. Front Med (Lausanne) 2021; 8:777861. https://doi.org/10.3389/fmed.2021.777861.10.3389/fmed.2021.77786134988095 PMC 8720766 · doi ↗ · pubmed ↗
- 2Zinman B Wanner C Lachin JM Fitchett D Bluhmki E Hantel S. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015; 373:2117–28. https://doi.org/10.1056/NEJ Moa 1504720.10.1056/NEJ Moa 150472026378978 · doi ↗ · pubmed ↗
- 3Packer M Anker SD Butler J Filippatos G Pocock SJ Carson P. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med 2020; 383:1413–24. https://doi.org/10.1056/NEJ Moa 2022190.10.1056/NEJ Moa 202219032865377 · doi ↗ · pubmed ↗
- 4Anker SD Butler J Filippatos G Ferreira JP Bocchi EBöhm M. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med 2021; 385:1451–61. https://doi.org/10.1056/NEJ Moa 2107038.10.1056/NEJ Moa 210703834449189 · doi ↗ · pubmed ↗
- 5Mc Guire DK Shih WJ Cosentino F Charbonnel B Cherney DZI Dagogo-Jack S. Association of SGLT 2 inhibitors with cardiovascular and kidney outcomes in patients with type 2 diabetes: A meta-analysis. JAMA Cardiol 2021; 6:148–58. https://doi.org/10.1001/jamacardio.2020.4511.10.1001/jamacardio.2020.451133031522 PMC 7542529 · doi ↗ · pubmed ↗
- 6Giugliano D Scappaticcio L Longo M Caruso P Maiorino MI Bellastella G. GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: An updated meta-analysis of eight CVO Ts. Cardiovasc Diabetol 2021; 20:189. https://doi.org/10.1186/s 12933-021-01366-8.10.1186/s 12933-021-01366-834526024 PMC 8442438 · doi ↗ · pubmed ↗
- 7Rivinius R Gralla C Helmschrott M Darche FF Ehlermann P Bruckner T. Pre-transplant type 2 diabetes mellitus is associated with higher graft failure and increased 5-year mortality after heart transplantation. Front Cardiovasc Med 2022; 9:890359. https://doi.org/10.3389/fcvm.2022.890359.10.3389/fcvm.2022.89035935757347 PMC 9218221 · doi ↗ · pubmed ↗
- 8Kim HJ Jung SH Kim JJ Yun TJ Kim JB Choo SJ. New-onset diabetes mellitus after heart transplantation – Incidence, risk factors and impact on clinical outcome. Circ J 2017; 81:806–14. https://doi.org/10.1253/circj.CJ-16-0963.10.1253/circj.CJ-16-096328344200 · doi ↗ · pubmed ↗